Too Much Or Too Little Testosterone?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One Man’s Saw Palmetto Is Another Woman’s Serenoa Repens…
Today we’re going to look at saw palmetto. So, first:
What is it?
Saw palmetto is a type of palm native to the southeastern United States. Its scientific name is “Serenoa repens”, so if that name appears in studies we cite, it’s the same thing. By whichever name, it’s widely enjoyed as a herbal supplement.
Why do people take it?
Here’s where it gets interesting, because people take it for some completely opposite reasons…
Indeed, searching for it on the Internet will cause Google to suggest “…for men” and “…for women” as the top suggestions.
That’s because it works on testosterone, and testosterone can be a bit of a double-edged sword, so some people want to increase or decrease certain testosterone-related effects on their body.
And it works for both! Here be science:
- Testosterone (henceforth, “T”) is produced in the human body.
- Yes, all human bodies, to some extent.
- An enzyme called 5-alpha-reductase converts T in to DHT (dihydrogen testosterone)
- DHT is a much more potent androgen (masculinizing agent) than T alone, such that its effects are often unwanted, including:
- Enlarged prostate (if you have one)
- Hair loss (especially in men)
- New facial hair growth (usually unwanted by women)
- Women are more likely to get this due to PCOS and/or the menopause
To avoid those effects, you really want less of your T to be converted into DHT.
Saw palmetto is a 5α-reductase inhibitor, so if you take it, you’ll have less DHT, and you’ll consequently lose less hair, have fewer prostate problems, etc.
^The above study showed that saw palmetto extract performed comparably to finasteride. Finasteride is the world’s main go-to prescription drug for treating enlarged prostate and/or hair loss.
See also: Natural Hair Supplement: Friend or Foe? Saw Palmetto, a Systematic Review in Alopecia
Hair today… Growing tomorrow!
So, what was that about increasing T levels?
Men usually suffer declining T levels as they get older, with a marked drop around the age of 45. With lower T comes lower energy, lower mood, lower libido, erectile dysfunction, etc.
Guess what… It’s T that’s needed for those things, not DHT. So if you block the conversion of T to DHT, you’ll have higher blood serum T levels, higher energy, higher mood, higher libido, and all that.
(the above assumes you have testicles, without which, your T levels will certainly not increase)
Saw Palmetto Against Enlarged Prostate?
With higher DHT levels in mid-late life, prostate enlargement (benign prostatic hyperlasia) can become a problem for many men. The size of that problem ranges from urinary inconvenience (common, when the prostate presses against the bladder) to prostate cancer (less common, much more serious). Saw palmetto, like other 5α-reductase inhibitors such as finasteride, may be used to prevent or treat this.
Wondering how safe/reliable it is? We found a very high-quality fifteen-year longitudinal observational study of the use of saw palmetto, and it found:
❝The 15 years’ study results suggest that taking S. repens plant extract continuously at a daily dose of 320 mg is an effective and safe way to prevent the progression of benign prostatic hyperplasia.❞
Want a second opinion? We also found a 10-year study (by different researchers with different people taking it), which reached the same conclusion:
❝The results of study showed the absence of progression, both on subjective criteria (IPSS, and QoL scores), and objective criteria (prostate volume, the rate of urination, residual urine volume). Furthermore, patients had no undesirable effects directly related to the use of this drug.❞
- IPSS = International Prostate Symptom Score
- QoL = Quality of Life
❝But wait a minute; I, a man over the age of 45 with potentially declining T levels but a fabulous beard, remember that you said just a minute ago that saw palmetto is used by women to avoid having facial hair; I don’t want to lose mine!❞
You won’t. Once your facial hair follicles were fully developed and activated during puberty, they’ll carry on doing what they do for life. That’s no longer regulated by hormones once they’re up and running.
The use of saw palmetto can only be used to limit facial hair if caught early—so it’s more useful at the onset of menopause, for those who have (or will have) such, or else upon the arrival of PCOS symptoms or hirsuitism from some other cause.
Take The Test!
Do you have a prostate, and would like to know your IPSS score, and what that means for your prostate health?
(takes 1 minute, no need to pee or go probing for anything)
Bottom Line on Saw Palmetto
- It blocks the conversion of T into DHT
- It will increase blood serum T levels, thus boosting mood, energy, libido, etc in men (who typically have more T, but whose T levels decline with age)
- It will decrease DHT levels, thus limiting hair loss (especially in men) and later-life new facial hair growth (especially in women).
- It can be used to prevent or treat prostate enlargement
- Bonus: it’s a potent antioxidant and thus reduces general inflammation (in everyone)
Want To Try Saw Palmetto?
We don’t sell it (or anything else), but for your convenience…
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Is it OK if my child eats lots of fruit but no vegetables?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Does it seem like most vegetables you serve your children end up left on the plate, or worse, strewn across the floor? But mention dessert, and your fruit skewers are polished off in an instant.
Or maybe the carrot and cucumber sticks keep coming home in your child’s lunchbox untouched, yet the orange slices are nowhere to be seen.
If you’re facing these struggles with your child, you’re not alone. Many children prefer fruit to vegetables.
So if your child eats lots of fruit but minimal or no vegetables, is that OK? And how can you get them to eat more veggies?
Children have an innate preference for fruit
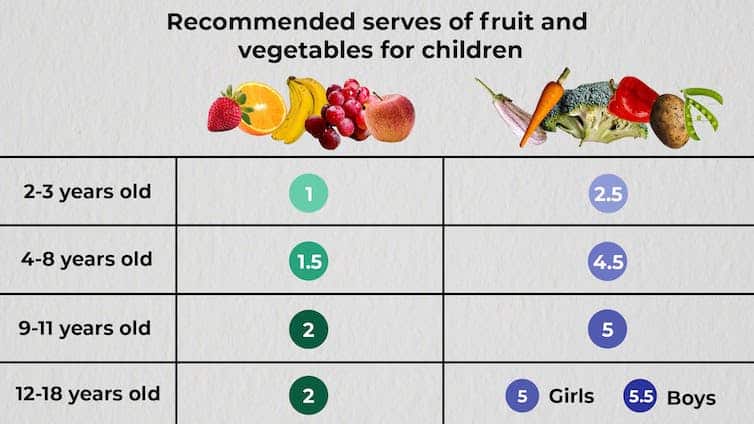
The Australian Dietary Guidelines’ recommended daily intakes for vegetables and fruit depend on a child’s age.

Fruit and vegetable serving sizes by age. The Conversation.
National Health and Medical Research Council, CC BY-SAConsumption among Australian children falls well below recommendations. Around 62.6% of children aged over two meet the recommended daily fruit intake, but only 9% meet the recommended vegetable intake.
This is not surprising given children have a natural preference for fruit. At least in part, this is due to its sweetness and texture, whether crispy, crunchy or juicy. The texture of fruit has been linked to a positive sensory experience among children.
Vegetables, on the other hand, are more of an acquired taste, and certain types, such as cruciferous vegetables, can be perceived by children as bitter.
The reason children often prefer fruit over vegetables could also be related to the parents’ preferences. Some research has even suggested we develop food preferences before birth based on what our mother consumes during pregnancy.
Balance is key
So, a preference for fruit is common. But is it OK if your child eats lots of fruit but little to no vegetables? This is a question we, as dietitians, get asked regularly.
You might be thinking, at least my child is eating fruit. They could be eating no veggies and no fruit. This is true. But while it’s great your child loves fruit, vegetables are just as important as part of a balanced eating pattern.
Vegetables provide us with energy, essential vitamins and minerals, as well as water and fibre, which help keep our bowels regular. They also support a strong immune system.
If your child is only eating fruit, they are missing some essential nutrients. But the same is true if they are eating only veggies.
Fruit likewise provides the body with a variety of essential vitamins and minerals, as well as phytochemicals, which can help reduce inflammation.
Evidence shows healthy consumption of fruit and vegetables protects against chronic diseases including high blood pressure, heart disease and stroke.
Consumed together, fruit and vegetables in a variety of colours provide different nutrients we need, some of which we can’t get from other foods. We should encourage kids to eat a “rainbow” of fruit and vegetables each day to support their growth and development.
What if my child eats too much fruit?
If your child is eating slightly more fruit than what’s recommended each day, it’s not usually a problem.
Fruit contains natural sugar which is good for you. But too much of a good thing, even if it’s natural, can create problems. Fruit also contains virtually no fat and very little to no protein, both essential for a growing child.
When overindulging in fruit starts to displace other food groups such as vegetables, dairy products and meat, that’s when things can get tricky.
6 tips to get your kids to love vegetables
1. Get them involved
Take your child with you when you go shopping. Let them choose new vegetables. See if you can find vegetables even you haven’t tried, so you’re both having a new experience. Then ask them to help you with preparing or cooking the vegetables using a recipe you have chosen together. This will expose your child to veggies in a positive way and encourage them to eat more.
2. Sensory learning
Try to expose your child to vegetables rather than hiding them. Kids are more likely to eat veggies when they see, smell and feel them. This is called sensory learning.
3. Have fun with food
Use colourful vegetables of different sizes and textures. Make them fun by creating scenes or faces on your child’s plate. Add edible flowers or mint for decoration. You can even serve this with a side of veggie-based dip such as hummus or guacamole for some bonus healthy fats.
4. Teach them to grow their own
Teach your child how to grow their own vegetables. Evidence shows kids are more inclined to try the food they have helped and watched grow. You don’t need to have a big backyard to do this. A windowsill with a pot plant is a perfect start.
5. Lead by example
Your child learns from you, and your eating habits will influence theirs. Ensure they see you eating and enjoying veggies, whether in meals or as snacks.
6. Practise persistence
If your child refuses a particular vegetable once, don’t give up. It can take many attempts to encourage children to try a new food.

Yasmine Probst, Associate Professor, School of Medical, Indigenous and Health Sciences, University of Wollongong; Olivia Wills, Accredited Practising Dietitian, PhD candidate, University of Wollongong, and Shoroog Allogmanny, Accredited Practising Dietitian, PhD candidate, University of Wollongong
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

The Emperor’s New Klotho, Or Something More?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Unzipping The Genes Of Aging?
Klotho is an enzyme encoded in humans’ genes—specifically, in the KL gene.
It’s found throughout all living parts of the human body (and can even circulate about in its hormonal form, or come to rest in its membranaceous form), and its subgroups are especially found:
- α-klotho: in the brain
- β-klotho: in the liver
- γ-klotho: in the kidneys
Great! Why do we care?
Klotho, its varieties and variants, its presence or absence, are very important in aging.
Almost every biological manifestation of aging in humans has some klotho-related indicator; usually the decrease or mutation of some kind of klotho.
Which way around the cause and effect go has been the subject of much debate and research: do we get old because we don’t have enough klotho, or do we make less klotho because we’re getting old?
Of course, everything has to be tested per variant and per system, so that can take a while (punctuated by research scientists begging for more grants to do the next one). Given that it’s about aging, testing in humans would take an incredibly long while, so most studies so far have been rodent studies.
The general gist of the results of rodent studies is “reduced klotho hastens aging; increased klotho slows it”.
(this can be known by artificially increasing or decreasing the level of klotho expression, again something easier in mice as it is harder to arrange transgenic humans for the studies)
Here’s one example of many, of that vast set of rodent studies:
Suppression of Aging in Mice by the Hormone Klotho
Relevance for Alzheimer’s, and a science-based advice
A few years ago (2020), an Alzheimer’s study was undertaken; they noted that the famous apolipoprotein E4 (apoE4) allele is the strongest genetic risk factor for Alzheimer’s, and that klotho may be another. FGF21 (secreted by the liver, mostly during fasting) binds to its own receptor (FGFR1) and its co-receptor β-klotho. Since this is a known neuroprotective factor, they wondered whether klotho itself may interact with β-amyloid (Aβ), and found:
❝Aβ can enhance the ability of klotho to draw FGF21 to regions of incipient neurodegeneration in AD❞
In other words: β-amyloid, the substance whose accumulation is associated with neurodegeneration in Alzheimer’s disease, is a mediator in klotho bringing a known neuroprotective factor, FGF21, to the areas of neurodegeneration
In fewer words: klotho calls the firefighters to the scene of the fire
Read more: Alignment of Alzheimer’s disease amyloid β-peptide and klotho
The advice based on this? Consider practicing intermittent fasting, if that is viable for you, as it will give your liver more FGF21-secreting time, and the more FGF21, the more firefighters arrive when klotho sounds the alarm.
See also: Intermittent Fasting: What’s the truth?
…and while you’re at it:
Does intermittent fasting have benefits for our brain?
A more recent (2023) study with a slightly different (but connected) purpose, found results consistent with this:
Longevity factor klotho enhances cognition in aged nonhuman primates
…and, for that matter this (2023) study that found:
Associations between klotho and telomere biology in high stress caregivers
…which looks promising, but we’d like to see it repeated with a sounder method (they sorted caregiving into “high-stress” and “low-stress” depending on whether a child was diagnosed with ASD or not, which is by no means a reliable way of sorting this). They did ask for reported subjective stress levels, but to be more objective, we’d like to see clinical markers of stress (e.g. cortisol levels, blood pressure, heart rate changes, etc).
A very recent (April 2024) study found that it has implications for more aspects of aging—and this time, in humans (but using a population-based cohort study, rather than lab conditions):
Can I get it as a supplement?
Not with today’s technology and today’s paucity of clinical trials, you can’t. Maybe in the future!
However… The presence of senescent (old, badly copied, stumbling and staggering onwards when they should have been killed and eaten and recycled already) cells actively reduces klotho levels, which means that taking supplements that are senolytic (i.e., that kill those senescent cells) can increase serum klotho levels:
Orally-active, clinically-translatable senolytics restore α-Klotho in mice and humans
Ok, what can I take for that?
We wrote about a senolytic supplement that you might enjoy, recently:
Fisetin: The Anti-Aging Assassin
Want to know more?
If you have the time, Dr. Peter Attia interviews Dr. Dena Dubal (researcher in several of the above studies) here:
Click Here If The Embedded Video Doesn’t Load Automatically
Enjoy!
Share This Post
-

The Art of Being Unflappable (Tricks For Daily Life)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Art of Being Unflappable
From Stoicism to CBT, thinkers through the ages have sought the unflappable life.
Today, in true 10almonds fashion, we’re going to distil it down to some concentrated essentials that we can all apply in our daily lives:
Most Common/Impactful Cognitive Distortions To Catch (And Thus Avoid)
These are like the rhetorical fallacies with which you might be familiar (ad hominem, no true Scotsman, begging the question, tu quoque, straw man, etc), but are about what goes on between your own ears, pertaining to your own life.
If we learn about them and how to recognize them, however, we can catch them before they sabotage us, and remain “unflappable” in situations that could otherwise turn disastrous.
Let’s take a look at a few:
Catastrophizing / Crystal Ball
- Distortion: not just blowing something out of proportion, but taking an idea and running with it to its worst possible conclusion. For example, we cook one meal that’s a “miss” and conclude we are a terrible cook, and in fact for this reason a terrible housewife/mother/friend/etc, and for this reason everyone will probably abandon us and would be right to do so
- Reality: by tomorrow, you’ll probably be the only one who even remembers it happened
Mind Reading
- Distortion: attributing motivations that may or may not be there, and making assumptions about other people’s thoughts/feelings. An example is the joke about two partners’ diary entries; one is long and full of feelings about how the other is surely dissatisfied in their marriage, has been acting “off” with them all day, is closed and distant, probably wants to divorce, may be having an affair and is wondering which way to jump, and/or is just wondering how to break the news—the other partner’s diary entry is short, and reads “motorcycle won’t start; can’t figure out why”
- Reality: sometimes, asking open questions is better than guessing, and much better than assuming!
All-or-Nothing Thinking / Disqualifying the Positive / Magnifying the Negative
- Distortion: having a negative bias that not only finds a cloud in every silver lining, but stretches it out so that it’s all that we can see. In a relationship, this might mean that one argument makes us feel like our relationship is nothing but strife. In life in general, it may lead us to feel like we are “naturally unlucky”.
- Reality: those negative things wouldn’t even register as negative to us if there weren’t a commensurate positive we’ve experienced to hold them in contrast against. So, find and remember that positive too.
For brevity, we put a spotlight on (and in some cases, clumped together) the ones we think have the most bang-for-buck to know about, but there are many more.
So for the curious, here’s some further reading:
Share This Post
Related Posts
-

Can I Eat That? – by Jenefer Roberts
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The answer to the question in the title is: you can eat pretty much anything, if you’re prepared for the consequences!
This book looks to give you the information to make your own decisions in that regard. There’s a large section on the science of glucose metabolism in the context of food (other aspects of glucose metabolism aren’t covered), so you will not simply be told “raw carrots are good; mashed potatoes are bad”, you’ll understand many factors that affect it, e.g:
- Macronutrient profiles of food and resultant base glycemic indices
- How the glycemic index changes if you cut something, crush it, mash it, juice it, etc
- How the glycemic index changes if you chill something, heat it, fry it, boil it, etc
- The many “this food works differently in the presence of this other food” factors
- How your relative level of insulin resistance affects things itself
…and much more.
The style is simple and explanatory, without deep science, but with good science and comprehensive advice.
There are also the promised recipes; they’re in an appendix at the back and aren’t the main meat of the book, though.
Bottom line: if you’ve ever found it confusing working out what works how in the mysterious world of diabetes nutrition, this book is a top tier demystifier.
Click here to check out Can I Eat That?, and gain confidence in your food choices!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Your Brain on Art – by Susan Magsamen & Ivy Ross
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The notion of art therapy is popularly considered a little wishy-washy. As it turns out, however, there are thousands of studies showing its effectiveness.
Nor is this just a matter of self-expression. As authors Magsamen and Ross explore, different kinds of engagement with art can convey different benefits.
That’s one of the greatest strengths of this book: “this form of engagement with art will give these benefits, according to these studies”
With benefits ranging from reducing stress and anxiety, to overcoming psychological trauma or physical pain, there’s a lot to be said for art!
And because the book covers many kinds of art, if you can’t imagine yourself taking paintbrush to canvas, that’s fine too. We learn of the very specific cognitive benefits of coloring in mandalas (yes, really), of sculpting something terrible in clay, or even just of repainting the kitchen, and more. Each thing has its set of benefits.
The book’s main goal is to encourage the reader to cultivate what the authors call an aesthetic mindset, which involves four key attributes:
- a high level of curiosity
- a love of playful, open-ended exploration
- a keen sensory awareness
- a drive to engage in creative activities
And, that latter? It’s as a maker and/or a beholder. We learn about what we can gain just by engaging with art that someone else made, too.
Bottom line: come for the evidence-based cognitive benefits; stay for the childlike wonder of the universe. If you already love art, or have thought it’s just “not for you”, then this book is for you.
Click here to check out Your Brain On Art, and open up whole new worlds of experience!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How stigma perpetuates substance use
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In 2022, 54.6 million people 12 and older in the United States needed substance use disorder (SUD) treatment. Of those, only 24 percent received treatment, according to the most recent National Survey on Drug Use and Health.
SUD is a treatable, chronic medical condition that causes people to have difficulty controlling their use of legal or illegal substances, such as alcohol, tobacco, prescription opioids, heroin, methamphetamine, or cocaine. Using these substances may impact people’s health and ability to function in their daily life.
While help is available for people with SUD, the stigma they face—negative attitudes, stereotypes, and discrimination—often leads to shame, worsens their condition, and keeps them from seeking help.
Read on to find out more about how stigma perpetuates substance use.
Stigma can keep people from seeking treatment
Suzan M. Walters, assistant professor at New York University’s Grossman School of Medicine, has seen this firsthand in her research on stigma and health disparities.
She explains that people with SUD may be treated differently at a hospital or another health care setting because of their drug use, appearance (including track marks on their arms), or housing situation, which may discourage them from seeking care.
“And this is not just one case; this is a trend that I’m seeing with people who use drugs,” Walters tells PGN. “Someone said, ‘If I overdose, I’m not even going to the [emergency room] to get help because of this, because of the way I’m treated. Because I know I’m going to be treated differently.’”
People experience stigma not only because of their addiction, but also because of other aspects of their identities, Walters says, including “immigration or race and ethnicity. Hispanic folks, brown folks, Black folks [are] being treated differently and experiencing different outcomes.”
And despite the effective harm reduction tools and treatment options available for SUD, research has shown that stigma creates barriers to access.
Syringe services programs, for example, provide infectious disease testing, Narcan, and fentanyl test strips. These programs have been proven to save lives and reduce the spread of HIV and hepatitis C. SSPs don’t increase crime, but they’re often mistakenly “viewed by communities as potential settings of drug-related crime;” this myth persists despite decades of research proving that SSPs make communities safer.
To improve this bias, Walters says it’s helpful for people to take a step back and recognize how we use substances, like alcohol, in our own lives, while also humanizing those with addiction. She says, “There’s a lack of understanding that these are human beings and people … [who] are living lives, and many times very functional lives.”
Misconceptions lead to stigma
SUD results from changes in the brain that make it difficult for a person to stop using a substance. But research has shown that a big misconception that leads to stigma is that addiction is a choice and reflects a person’s willpower.
Michelle Maloney, executive clinical director of mental health and addiction recovery services for Rogers Behavioral Health, tells PGN that statements such as “you should be able to stop” can keep a patient from seeking treatment. This belief goes back to the 1980s and the War on Drugs, she adds.
“We think about public service announcements that occurred during that time: ‘Just say no to drugs,’” Maloney says. “People who have struggled, whether that be with nicotine, alcohol, or opioids, [know] it’s not as easy as just saying no.”
Stigma can worsen addiction
Stigma can also lead people with SUD to feel guilt and shame and blame themselves for their medical condition. These feelings, according to the National Institute on Drug Abuse, may “reinforce drug-seeking behavior.”
In a 2020 article, Dr. Nora D. Volkow, the director of NIDA, said that “when internalized, stigma and the painful isolation it produces encourage further drug taking, directly exacerbating the disease.”
Overall, research agrees that stigma harms people experiencing addiction and can make the condition worse. Experts also agree that debunking myths about the condition and using non-stigmatizing language (like saying someone is a person with a substance use disorder, not an addict) can go a long way toward reducing stigma.
Resources to mitigate stigma:
- CDC: Stigma Reduction
- National Harm Reduction Coalition: Respect To Connect: Undoing Stigma
- NIDA:
- Shatterproof: Addiction language guide (Disclosure: The Public Good Projects, PGN’s parent company, is a Shatterproof partner)
This article first appeared on Public Good News and is republished here under a Creative Commons license.

Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: