
Is it OK if my child eats lots of fruit but no vegetables?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Does it seem like most vegetables you serve your children end up left on the plate, or worse, strewn across the floor? But mention dessert, and your fruit skewers are polished off in an instant.
Or maybe the carrot and cucumber sticks keep coming home in your child’s lunchbox untouched, yet the orange slices are nowhere to be seen.
If you’re facing these struggles with your child, you’re not alone. Many children prefer fruit to vegetables.
So if your child eats lots of fruit but minimal or no vegetables, is that OK? And how can you get them to eat more veggies?
Children have an innate preference for fruit
The Australian Dietary Guidelines’ recommended daily intakes for vegetables and fruit depend on a child’s age.
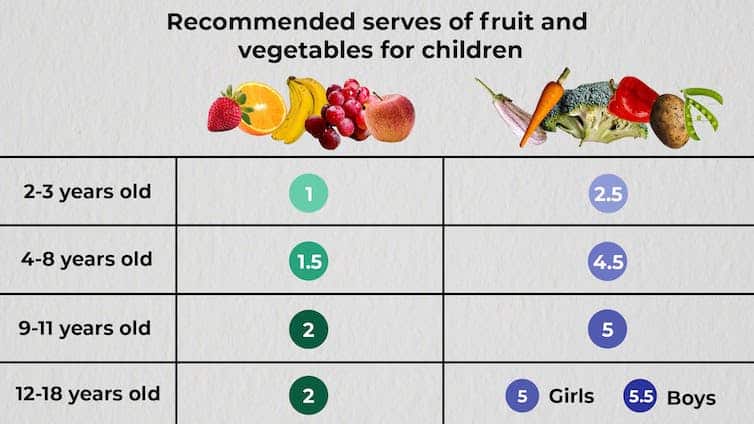
National Health and Medical Research Council, CC BY-SA
Consumption among Australian children falls well below recommendations. Around 62.6% of children aged over two meet the recommended daily fruit intake, but only 9% meet the recommended vegetable intake.
This is not surprising given children have a natural preference for fruit. At least in part, this is due to its sweetness and texture, whether crispy, crunchy or juicy. The texture of fruit has been linked to a positive sensory experience among children.
Vegetables, on the other hand, are more of an acquired taste, and certain types, such as cruciferous vegetables, can be perceived by children as bitter.
The reason children often prefer fruit over vegetables could also be related to the parents’ preferences. Some research has even suggested we develop food preferences before birth based on what our mother consumes during pregnancy.
Balance is key
So, a preference for fruit is common. But is it OK if your child eats lots of fruit but little to no vegetables? This is a question we, as dietitians, get asked regularly.
You might be thinking, at least my child is eating fruit. They could be eating no veggies and no fruit. This is true. But while it’s great your child loves fruit, vegetables are just as important as part of a balanced eating pattern.
Vegetables provide us with energy, essential vitamins and minerals, as well as water and fibre, which help keep our bowels regular. They also support a strong immune system.
If your child is only eating fruit, they are missing some essential nutrients. But the same is true if they are eating only veggies.
Fruit likewise provides the body with a variety of essential vitamins and minerals, as well as phytochemicals, which can help reduce inflammation.
Evidence shows healthy consumption of fruit and vegetables protects against chronic diseases including high blood pressure, heart disease and stroke.
Consumed together, fruit and vegetables in a variety of colours provide different nutrients we need, some of which we can’t get from other foods. We should encourage kids to eat a “rainbow” of fruit and vegetables each day to support their growth and development.
What if my child eats too much fruit?
If your child is eating slightly more fruit than what’s recommended each day, it’s not usually a problem.
Fruit contains natural sugar which is good for you. But too much of a good thing, even if it’s natural, can create problems. Fruit also contains virtually no fat and very little to no protein, both essential for a growing child.
When overindulging in fruit starts to displace other food groups such as vegetables, dairy products and meat, that’s when things can get tricky.
6 tips to get your kids to love vegetables
1. Get them involved
Take your child with you when you go shopping. Let them choose new vegetables. See if you can find vegetables even you haven’t tried, so you’re both having a new experience. Then ask them to help you with preparing or cooking the vegetables using a recipe you have chosen together. This will expose your child to veggies in a positive way and encourage them to eat more.
2. Sensory learning
Try to expose your child to vegetables rather than hiding them. Kids are more likely to eat veggies when they see, smell and feel them. This is called sensory learning.
3. Have fun with food
Use colourful vegetables of different sizes and textures. Make them fun by creating scenes or faces on your child’s plate. Add edible flowers or mint for decoration. You can even serve this with a side of veggie-based dip such as hummus or guacamole for some bonus healthy fats.
4. Teach them to grow their own
Teach your child how to grow their own vegetables. Evidence shows kids are more inclined to try the food they have helped and watched grow. You don’t need to have a big backyard to do this. A windowsill with a pot plant is a perfect start.
5. Lead by example
Your child learns from you, and your eating habits will influence theirs. Ensure they see you eating and enjoying veggies, whether in meals or as snacks.
6. Practise persistence
If your child refuses a particular vegetable once, don’t give up. It can take many attempts to encourage children to try a new food.![]()
Yasmine Probst, Associate Professor, School of Medical, Indigenous and Health Sciences, University of Wollongong; Olivia Wills, Accredited Practising Dietitian, PhD candidate, University of Wollongong, and Shoroog Allogmanny, Accredited Practising Dietitian, PhD candidate, University of Wollongong
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Lychee vs Pear – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing lychees to pears, we picked the lychees.
Why?
Both have their strong points:
In terms of macros, the only meaningful difference is that pears have nearly 3x the fiber—other macros have only negligible differences (i.e. within the margin of variation, so it’d depend on the individual plant you got it from), so this is a clear deciding factor here is the fiber, and it’s clearly in pears’ favor.
In the category of vitamins, lychees have more of vitamins B2, B3, B6, B7, B9, C, and choline, while pears have more of vitamins A, E, and K. Notably, lychees are an especially good source of vitamin C, with 1 cup providing 1.5x the daily requirement. In any case, lychees are also the winner here by strength of numbers in total.
When it comes to minerals, lychees have more copper, iron, magnesium, manganese, phosphorus, potassium, and selenium, while pears have more calcium and zinc. Another win for lychees!
Adding up the sections makes for an overall win for lychees, but pears are great too, especially for fiber, so do by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Share This Post
-
Brussels Sprouts vs Spinach – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing Brussels sprouts to spinach, we picked the spinach.
Why?
It was close! Which is hardly surprising, as Brussels sprouts almost always win head-to-head comparisons with most things. In this case…
In terms of macros, the sprouts have more fiber, carbs, and protein, making them the more nutrient-dense option in the macros category.
In the category of vitamins, sprouts have more of vitamins B1, B5, B6, and C, while spinach has more of vitamins A, B2, B3, B9, E, and K, thus a win for spinach here.
When it comes to minerals, sprouts have more phosphorus and selenium, while spinach has more calcium, copper, iron, magnesium, manganese, potassium, and zinc—another win for spinach.
With regard to phytochemicals, spinach has a higher polyphenol content (mostly flavonols), and on the flipside, spinach has a much higher oxalate content (that’s not a problem for most people, but bad if you have certain kidney issues). So this category could be swung any which way depending on the state of your kidneys. For simplicity, we’ll record this round as a tie, but its constituent parts are worth bearing in mind.
Thus, adding up the sections makes for an overall win for spinach, unless you have kidney problems that necessitate keeping your oxalate levels down, in which case, Brussels sprouts. Either way, it was close, so do enjoy either or both; diversity is good!
Want to learn more?
You might like:
Enjoy!
Share This Post
-
When They Don’t Recognize You Anymore
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It happened more than a decade ago, but the moment remains with her.
Sara Stewart was talking at the dining room table with her mother, Barbara Cole, 86 at the time, in Bar Harbor, Maine. Stewart, then 59, a lawyer, was making one of her extended visits from out of state.
Two or three years earlier, Cole had begun showing troubling signs of dementia, probably from a series of small strokes. “I didn’t want to yank her out of her home,” Stewart said.
So with a squadron of helpers — a housekeeper, regular family visitors, a watchful neighbor, and a meal delivery service — Cole remained in the house she and her late husband had built 30-odd years earlier.
She was managing, and she usually seemed cheerful and chatty. But this conversation in 2014 took a different turn.
“She said to me: ‘Now, where is it we know each other from? Was it from school?’” her daughter and firstborn recalled. “I felt like I’d been kicked.”
Stewart remembers thinking, “In the natural course of things, you were supposed to die before me. But you were never supposed to forget who I am.” Later, alone, she wept.
People with advancing dementia do regularly fail to recognize beloved spouses, partners, children, and siblings. By the time Stewart and her youngest brother moved Cole into a memory-care facility a year later, she had almost completely lost the ability to remember their names or their relationship to her.
“It’s pretty universal at the later stages” of the disease, said Alison Lynn, director of social work at the Penn Memory Center, who has led support groups for dementia caregivers for a decade.
She has heard many variations of this account, a moment described with grief, anger, frustration, relief, or some combination thereof.
These caregivers “see a lot of losses, reverse milestones, and this is one of those benchmarks, a fundamental shift” in a close relationship, she said. “It can throw people into an existential crisis.”
It’s hard to determine what people with dementia — a category that includes Alzheimer’s disease and many other cognitive disorders — know or feel. “We don’t have a way of asking the person or looking at an MRI,” Lynn noted. “It’s all deductive.”
But researchers are starting to investigate how family members respond when a loved one no longer appears to know them. A qualitative study recently published in the journal Dementia analyzed in-depth interviews with adult children caring for mothers with dementia who, at least once, did not recognize them.
“It’s very destabilizing,” said Kristie Wood, a clinical research psychologist at the University of Colorado Anschutz Medical Campus and co-author of the study. “Recognition affirms identity, and when it’s gone, people feel like they’ve lost part of themselves.”
Although they understood that nonrecognition was not rejection but a symptom of their mothers’ disease, she added, some adult children nevertheless blamed themselves.
“They questioned their role. ‘Was I not important enough to remember?’” Wood said. They might withdraw or visit less often.
Pauline Boss, the family therapist who developed the theory of “ambiguous loss” decades ago, points out that it can involve physical absence — as when a soldier is missing in action — or psychological absence, including nonrecognition because of dementia.
Society has no way to acknowledge the transition when “a person is physically present but psychologically absent,” Boss said. There is “no death certificate, no ritual where friends and neighbors come sit with you and comfort you.”
“People feel guilty if they grieve for someone who’s still alive,” she continued. “But while it’s not the same as a verified death, it is a real loss and it just keeps coming.”
Nonrecognition takes different forms. Some relatives report that while a loved one with dementia can no longer retrieve a name or an exact relationship, they still seem happy to see them.
“She stopped knowing who I was in the narrative sense, that I was her daughter Janet,” Janet Keller, 69, an actress in Port Townsend, Washington, said in an email about her late mother, diagnosed with Alzheimer’s. “But she always knew that I was someone she liked and wanted to laugh with and hold hands with.”
It comforts caregivers to still feel a sense of connection. But one of the respondents in the Dementia study reported that her mother felt like a stranger and that the relationship no longer provided any emotional reward.
“I might as well be visiting the mailman,” she told the interviewer.
Larry Levine, 67, a retired health care administrator in Rockville, Maryland, watched his husband’s ability to recognize him shift unpredictably.
He and Arthur Windreich, a couple for 43 years, had married when Washington, D.C., legalized same-sex marriage in 2010. The following year, Windreich received a diagnosis of early-onset Alzheimer’s.
Levine became his caregiver until his death at 70, in late 2023.
“His condition sort of zigzagged,” Levine said. Windreich had moved into a memory-care unit. “One day, he’d call me ‘the nice man who comes to visit’,” Levine said. “The next day he’d call me by name.”
Even in his final years when, like many dementia patients, Windreich became largely nonverbal, “there was some acknowledgment,” his husband said. “Sometimes you could see it in his eyes, this sparkle instead of the blank expression he usually wore.”
At other times, however, “there was no affect at all.” Levine often left the facility in tears.
He sought help from his therapist and his sisters, and recently joined a support group for LGBTQ+ dementia caregivers even though his husband has died. Support groups, in person or online, “are medicine for the caregiver,” Boss said. “It’s important not to stay isolated.”
Lynn encourages participants in her groups to also find personal rituals to mark the loss of recognition and other reverse milestones. “Maybe they light a candle. Maybe they say a prayer,” she said.
Someone who would sit shiva, part of the Jewish mourning ritual, might gather a small group of friends or family to reminisce and share stories, even though the loved one with dementia hasn’t died.
“To have someone else participate can be very validating,” Lynn said. “It says, ‘I see the pain you’re going through.’”
Once in a while, the fog of dementia seems to lift briefly.
Researchers at Penn and elsewhere have pointed to a startling phenomenon called “paradoxical lucidity.” Someone with severe dementia, after being noncommunicative for months or years, suddenly regains alertness and may come up with a name, say a few appropriate words, crack a joke, make eye contact, or sing along with a radio.
Though common, these episodes generally last only seconds and don’t mark a real change in the person’s decline. Efforts to recreate the experiences tend to fail.
“It’s a blip,” Lynn said. But caregivers often respond with shock and joy; some interpret the episode as evidence that despite deepening dementia, they are not truly forgotten.
Stewart encountered such a blip a few months before her mother died. She was in her mother’s apartment when a nurse asked her to come down the hall.
“As I left the room, my mother called out my name,” she said. Though Cole usually seemed pleased to see her, “she hadn’t used my name for as long as I could remember.”
It didn’t happen again, but that didn’t matter. “It was wonderful,” Stewart said.
The New Old Age is produced through a partnership with The New York Times.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Share This Post



-

Vitamin K2 And The Calcium Paradox – by Kate Rhéaume-Bleue
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The premise of this book is that many people get enough calcium and vitamin D, but then a lot of that calcium doesn’t make it past the arteries.
Thus, the calcium paradox: we want to get (usually: more) calcium, but we want it building our bones, not lining our arteries. How, then, to resolve this problem, and simultaneously fight the dual threats of calcium deficiency (osteoporosis) and calcium excess (atherosclerosis)?
The answer, the author argues, is in vitamin K2, of which most people do not get enough, and which is needed to get calcium to where it’s supposed to be.
You may be wondering whether this is somehow 288 pages to say “take vitamin K2”. And, it somewhat is, but there are a lot of details when it comes to things that have historically raised or lowered the amount of vitamin K2 in our diet, what can be done about it in dietary terms if preferring to go all-natural (hint: nattō is an excellent option, but far from the only one), and what other effects vitamin K2 (or its deficiency) can have on us, in many of the body’s systems, far beyond just bone health (and including things as varied as fertility and avoidance of Alzheimer’s).
The style is very easy-reading pop-science, making this quite a quick read, but no less informative. There’s a fair bibliography at the back.
Bottom line: if you’d like to build/maintain your bone density, then the role of vitamin K2 is an important thing to take into account, and if you’re the sort of person who likes to understand things rather than just take them on faith, this book can explain it all very clearly.
Click here to check out Vitamin K2 And The Calcium Paradox, and look after your bones and more!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Ice baths are booming in popularity – but they come with health risks
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Walk through any trendy suburb and you might find a new “wellness” studio offering ice baths or “contrast therapy” (a sauna and ice bath combo).
Scroll social media, and you’re likely to come across influencers preaching the cold plunge gospel with cult-like zeal.
Ice baths have gone mainstream. Initially practised mainly among high-performance athletes, cold water immersion is now a booming business model: sold as recovery, discipline and therapy all in one.
But the benefits are questionable and, importantly, ice baths can have health risks – particularly for people who have limited experience using them.

Michele Ursi/Getty Images From Roman times to today
Cold water immersion isn’t a new concept.
The “frigidarium” – a room with a cold plunge pool or bath – was a feature in most Roman bathhouses.
For decades, athletes have used cold water immersion, such as swims in cold water, for recovery.
But in recent years, with the proliferation of commercial cold plunge centres, there’s been an explosion in people using ice baths recreationally.
Many people are even setting up their own ice baths at home. The global cold plunge tub market was valued at close to US$338 million in 2024 and is projected to reach nearly $483 million by 2033.
Social media shows serene influencers meditating through the pain, claiming it boosts mental health, serotonin, testosterone, and their metabolism. But does the evidence stack up?
Ice baths can reduce muscle soreness after intense training, however the effect is modest and short-lived.
Some research shows cold water immersion can improve mood after a single exposure in young, healthy people, but other research doesn’t find these benefits.
Most claims about mental health, testosterone and weight loss aren’t backed by strong evidence. Rather, they’re anecdotal and amplified by influencers.
What does an ice bath involve?
At commercial establishments, patrons can often use the ice baths as they please during a booked session. Ice bath temperatures often range anywhere from 3°C to 15°C. There normally isn’t actual ice in the bath, but some people add blocks of ice to their ice baths at home.
Businesses offering ice baths don’t always actively supervise patrons or monitor a person’s time in the ice bath. They may leave their customers to self-regulate, assuming people will know to get out of the water before they pass their body’s limits.
So what are the risks?
Cold water immersion triggers a powerful physiological response. When you hit cold water below 15°C, your body launches into cold shock. Gasping occurs and breathing becomes rapid and uncontrollable. Heart rate spikes. Blood pressure rises.
Staying in the water for too long can lead to hypothermia, a condition where a person’s core body temperature drops dangerously low.
Shivering may begin within minutes in cold water. Confusion or fainting are more serious signs that hypothermia may be developing.
Occasionally, this “cold shock” response can lead to a heart attack or stroke – especially if you have an undiagnosed condition affecting your heart, blood vessels or brain.
As far back as 1969, researchers found even experienced swimmers could struggle after just a few minutes in cold water. Participants were immersed in water at 4.7°C while fully clothed and asked to swim as if trying to reach safety. Some developed serious respiratory distress and had to stop swimming within as little as 90 seconds, well before any measurable drop in core body temperature.
Even after you get out, your core temperature can continue to fall – a phenomenon known as afterdrop. So you can encounter problems, such as collapse, even after leaving the water.
And even young, healthy people can be caught off guard. The body isn’t designed to endure freezing water for extended periods.
Recently one of us (Sam Cornell) had to provide first aid at an ice bath venue in Sydney. A young man collapsed after staying in an ice bath for ten minutes. He was shivering uncontrollably and clearly suffering from cold shock.
Cold exposure can also cause long-term damage to nerves and blood vessels in the hands and feet, known as non-freezing cold injury. This is more likely if someone spends an extended period immersed in cold water. Symptoms such as numbness, pain and sensitivity to cold can persist for years.
6 tips for safer recreational ice bath use
The ice bath trend is part of a broader wellness movement, promoted to young men in particular, where discomfort is repackaged as discipline. Push through the pain. Master your body. If you feel terrible, you must be doing it right.
But behind the hype lies a less appealing truth. Ice baths can be dangerous.
We advise caution, but if you do choose to try an ice bath, treat it seriously and follow these tips to reduce the risk of harm.
1. Talk to your doctor: get checked out first. If you or your family have any heart, stroke or respiratory risk, skip it
2. Know your limits: being fit doesn’t protect you from cold shock
3. Start gradually: begin with short warm to cold showers before full immersion
4. Never go alone: always have someone with you, especially if you’re new to ice baths
5. Keep it short and watch the temperature: limit sessions to 3–5 minutes and remember, problems can still occur after you get out
6. Recognise the signs of danger: symptoms such as shivering, numbness and confusion can all seem like part of the experience to someone bent on pushing themselves. But these can be signs of hypothermia.
Samuel Cornell, PhD Candidate in Public Health & Community Medicine, School of Population Health, UNSW Sydney and Michael Tipton, Professor of Human and Applied Physiology, University of Portsmouth
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The Eye Drops That Instantly Correct Myopia With Just One Drop
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
These days, there are increasingly many ways to give our eyes medical attention. Laser surgery opened a lot of doors (not to mention cutting into the window to your soul and all that), and even that may be becoming obsolete as science marches on. That said, some methods still seem a little too exciting for complete comfort, such as: Laser Eye Surgery Without The Laser Or The Surgery! ← uses electrochemical corneal refraction to reshape it!
But what about eye drops? Taking them is not most people’s favorite hobby, but they can help with minor conditions; dry eyes being the most obvious. Yet even these being gradually sidelined as other technologies step forwards, for example: A New Free App Offers Relief For Dry Eyes (Yes, Really)
But they can do more complex things too, as we’ve written about before, such as: New Eye Drops vs Age-Related Macular Degeneration
So, what’s this about treating myopia with eye drops?
Let’s take a close-up look at the evidence
Researchers (Dr. Lisa Ostrin & Dr. Barsha Lal) investigated this, and found that a single low-dose atropine eye drop (0.01%–0.1%) caused significant improvements to pupil size and focusing ability that lasted at least 24 hours, while not changing eye length, retinal thickness, or choroidal thickness over that period (that’s good).
How they tested it: it was a small (n=20) randomized controlled trial (RCT), in which healthy adults (average age 25.5) received placebo or one of four atropine concentrations in one eye across five randomized, double-masked sessions, with measurements taken at baseline, 1 hour, and 24 hours.
The results, in numbers:
❝The superficial vascular plexus perfusion density in the 1.0–2.5 mm annulus showed significant decrease (P = 0.02) with time after atropine instillation, but not with concentration (P > 0.05); post hoc analysis showed significant decrease from baseline at 1 h (P = 0.03) compared to 24 h (P = 0.28)❞
In other words: it helps significantly, and quickly. However, the results are temporary, and meaning that while one drop per eye is sufficient to gain these changes for a day, it’d be necessary to take it again later to get the same effect again. On the other hand, the temporary nature of the effects does suggest a good safety profile.
Or as Dr. Ostrin herself put it:
❝Characterizing these short-term effects is important for a better understanding of the physiological responses to atropine in clinical and research settings.
By linking objective ocular responses with subjective visual experience, this work advances our understanding of how atropine works and supports more precise, evidence-based, and individualized approaches to myopia management❞
~ Dr. Lisa Ostrin, Professor of Optometry
You can read the paper in full, here: Short-term effects of atropine on the retina and choroid in young adults
Note: yes, “young adults” per the average age of 25.5 that we mentioned above, though there’s no reason to assume this won’t work similarly for older adults; that’s just the science that’s been done so far, and scientists like to claim only what they can be confident their study actually shows.
Not a fan of eye drops?
Well, first you might want to check out: Tips For Putting In Eye Drops (3 Techniques That Work!) ← this writer uses technique #3; how about you?
But if you want a no-med, entirely DIY approach to better eyesight, then do consider this highly recommendable book we reviewed a while back:
Vision for Life, Revised Edition: Ten Steps to Natural Eyesight Improvement – by Dr. Meir Schneider
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:



