The Emperor’s New Klotho, Or Something More?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Unzipping The Genes Of Aging?
Klotho is an enzyme encoded in humans’ genes—specifically, in the KL gene.
It’s found throughout all living parts of the human body (and can even circulate about in its hormonal form, or come to rest in its membranaceous form), and its subgroups are especially found:
- α-klotho: in the brain
- β-klotho: in the liver
- γ-klotho: in the kidneys
Great! Why do we care?
Klotho, its varieties and variants, its presence or absence, are very important in aging.
Almost every biological manifestation of aging in humans has some klotho-related indicator; usually the decrease or mutation of some kind of klotho.
Which way around the cause and effect go has been the subject of much debate and research: do we get old because we don’t have enough klotho, or do we make less klotho because we’re getting old?
Of course, everything has to be tested per variant and per system, so that can take a while (punctuated by research scientists begging for more grants to do the next one). Given that it’s about aging, testing in humans would take an incredibly long while, so most studies so far have been rodent studies.
The general gist of the results of rodent studies is “reduced klotho hastens aging; increased klotho slows it”.
(this can be known by artificially increasing or decreasing the level of klotho expression, again something easier in mice as it is harder to arrange transgenic humans for the studies)
Here’s one example of many, of that vast set of rodent studies:
Suppression of Aging in Mice by the Hormone Klotho
Relevance for Alzheimer’s, and a science-based advice
A few years ago (2020), an Alzheimer’s study was undertaken; they noted that the famous apolipoprotein E4 (apoE4) allele is the strongest genetic risk factor for Alzheimer’s, and that klotho may be another. FGF21 (secreted by the liver, mostly during fasting) binds to its own receptor (FGFR1) and its co-receptor β-klotho. Since this is a known neuroprotective factor, they wondered whether klotho itself may interact with β-amyloid (Aβ), and found:
❝Aβ can enhance the ability of klotho to draw FGF21 to regions of incipient neurodegeneration in AD❞
In other words: β-amyloid, the substance whose accumulation is associated with neurodegeneration in Alzheimer’s disease, is a mediator in klotho bringing a known neuroprotective factor, FGF21, to the areas of neurodegeneration
In fewer words: klotho calls the firefighters to the scene of the fire
Read more: Alignment of Alzheimer’s disease amyloid β-peptide and klotho
The advice based on this? Consider practicing intermittent fasting, if that is viable for you, as it will give your liver more FGF21-secreting time, and the more FGF21, the more firefighters arrive when klotho sounds the alarm.
See also: Intermittent Fasting: What’s the truth?
…and while you’re at it:
Does intermittent fasting have benefits for our brain?
A more recent (2023) study with a slightly different (but connected) purpose, found results consistent with this:
Longevity factor klotho enhances cognition in aged nonhuman primates
…and, for that matter this (2023) study that found:
Associations between klotho and telomere biology in high stress caregivers
…which looks promising, but we’d like to see it repeated with a sounder method (they sorted caregiving into “high-stress” and “low-stress” depending on whether a child was diagnosed with ASD or not, which is by no means a reliable way of sorting this). They did ask for reported subjective stress levels, but to be more objective, we’d like to see clinical markers of stress (e.g. cortisol levels, blood pressure, heart rate changes, etc).
A very recent (April 2024) study found that it has implications for more aspects of aging—and this time, in humans (but using a population-based cohort study, rather than lab conditions):
Can I get it as a supplement?
Not with today’s technology and today’s paucity of clinical trials, you can’t. Maybe in the future!
However… The presence of senescent (old, badly copied, stumbling and staggering onwards when they should have been killed and eaten and recycled already) cells actively reduces klotho levels, which means that taking supplements that are senolytic (i.e., that kill those senescent cells) can increase serum klotho levels:
Orally-active, clinically-translatable senolytics restore α-Klotho in mice and humans
Ok, what can I take for that?
We wrote about a senolytic supplement that you might enjoy, recently:
Fisetin: The Anti-Aging Assassin
Want to know more?
If you have the time, Dr. Peter Attia interviews Dr. Dena Dubal (researcher in several of the above studies) here:
Click Here If The Embedded Video Doesn’t Load Automatically
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Tempeh vs Tofu – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing tempeh to tofu, we picked the tempeh.
Why?
Per 100g, tempeh has about 1.5x as many calories, about 2x as much protein, about 3x as much fiber, and about 4x the carbohydrates.
Which latter sounds like a lot, but really, the amounts here are small—tempeh is under 12% carbohydrates, and most of that is treated by the body as fiber (e.g. it’s a resistant starch).
Both have no sugar, and both have more or less the same (tiny) amount of fat.
Micronutrients, you ask? As they’re both made from soybeans, the micronutrient profiles are similar, but exact amounts will depend on the method used, so by all means check labels if comparing products in store. By and large, there’s usually not much difference, though.
You can see sample stats here:
In summary
Both are great, and/but tempeh is the more nutrient-dense of the two.
Therefore, tempeh is the healthier option, unless you are on a very strictly calorie-controlled diet, in which case, tofu will give you more quantity per calorie.
Enjoy!
Share This Post
-

Some women’s breasts can’t make enough milk, and the effects can be devastating
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many new mothers worry about their milk supply. For some, support from a breastfeeding counsellor or lactation consultant helps.
Others cannot make enough milk no matter how hard they try. These are women whose breasts are not physically capable of producing enough milk.
Our recently published research gives us clues about breast features that might make it difficult for some women to produce enough milk. Another of our studies shows the devastating consequences for women who dream of breastfeeding but find they cannot.
Some breasts just don’t develop
Unlike other organs, breasts are not fully developed at birth. There are key developmental stages as an embryo, then again during puberty and pregnancy.
At birth, the breast consists of a simple network of ducts. Usually during puberty, the glandular (milk-making) tissue part of the breast begins to develop and the ductal network expands. Then typically, further growth of the ductal network and glandular tissue during pregnancy prepares the breast for lactation.
But our online survey of women who report low milk supply gives us clues to anomalies in how some women’s breasts develop.
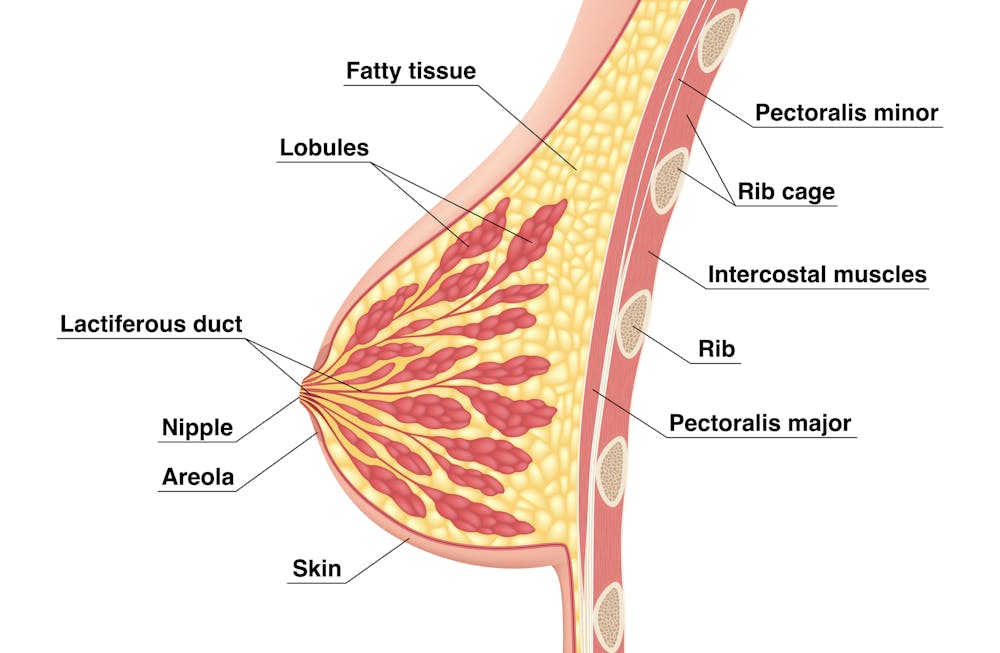
We’re not talking about women with small breasts, but women whose glandular tissue (shown in this diagram as “lobules”) is underdeveloped and have a condition called breast hypoplasia.

Sometimes not enough glandular tissue, shown here as lobules, develop.
Tsuyna/ShutterstockWe don’t know how common this is. But it has been linked with lower rates of exclusive breastfeeding.
We also don’t know what causes it, with much of the research conducted in animals and not humans.
However, certain health conditions have been associated with it, including polycystic ovary syndrome and other endocrine (hormonal) conditions. A high body-mass index around the time of puberty may be another indicator.
Could I have breast hypoplasia?
Our survey and other research give clues about who may have breast hypoplasia.
But it’s important to note these characteristics are indicators and do not mean women exhibiting them will definitely be unable to exclusively breastfeed.
Indicators include:
- a wider than usual gap between the breasts
- tubular-shaped (rather than round) breasts
- asymmetric breasts (where the breasts are different sizes or shapes)
- lack of breast growth in pregnancy
- a delay in or absence of breast fullness in the days after giving birth
In our survey, 72% of women with low milk supply had breasts that did not change appearance during pregnancy, and about 70% reported at least one irregular-shaped breast.
The effects
Mothers with low milk supply – whether or not they have breast hyoplasia or some other condition that limits their ability to produce enough milk – report a range of emotions.
Research, including our own, shows this ranges from frustration, confusion and surprise to intense or profound feelings of failure, guilt, grief and despair.
Some mothers describe “breastfeeding grief” – a prolonged sense of loss or failure, due to being unable to connect with and nourish their baby through breastfeeding in the way they had hoped.
These feelings of failure, guilt, grief and despair can trigger symptoms of anxiety and depression for some women.
Feelings of failure, guilt, grief and despair were common.
Bricolage/ShutterstockOne woman told us:
[I became] so angry and upset with my body for not being able to produce enough milk.
Many women’s emotions intensified when they discovered that despite all their hard work, they were still unable to breastfeed their babies as planned. A few women described reaching their “breaking point”, and their experience felt “like death”, “the worst day of [my] life” or “hell”.
One participant told us:
I finally learned that ‘all women make enough milk’ was a lie. No amount of education or determination would make my breasts work. I felt deceived and let down by all my medical providers. How dare they have no answers for me when I desperately just wanted to feed my child naturally.
Others told us how they learned to accept their situation. Some women said they were relieved their infant was “finally satisfied” when they began supplementing with formula. One resolved to:
prioritise time with [my] baby over pumping for such little amounts.
Where to go for help
If you are struggling with low milk supply, it can help to see a lactation consultant for support and to determine the possible cause.
This will involve helping you try different strategies, such as optimising positioning and attachment during breastfeeding, or breastfeeding/expressing more frequently. You may need to consider taking a medication, such as domperidone, to see if your supply increases.
If these strategies do not help, there may be an underlying reason why you can’t make enough milk, such as insufficient glandular tissue (a confirmed inability to make a full supply due to breast hypoplasia).
Even if you have breast hypoplasia, you can still breastfeed by giving your baby extra milk (donor milk or formula) via a bottle or using a supplementer (which involves delivering milk at the breast via a tube linked to a bottle).
More resources
The following websites offer further information and support:
- Australian Breastfeeding Association
- Lactation Consultants of Australia and New Zealand
- Royal Women’s Hospital, Melbourne
- Supply Line Breastfeeders Support Group of Australia Facebook support group
- IGT And Low Milk Supply Support Group Facebook support group
- Breastfeeding Medicine Network Australia/New Zealand
- Supporting breastfeeding grief (a collection of resources).
Shannon Bennetts, a research fellow at La Trobe University, contributed to this article.

Renee Kam, PhD candidate and research officer, La Trobe University and Lisa Amir, Professor in Breastfeeding Research, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Caregiver smartphone use can affect a baby’s development. New parents should get more guidance
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We already know excessive smartphone use affects people’s mental health and their relationships.
But when new parents use digital technologies during care giving, they might also compromise their baby’s development.
Smartphone use in the presence of infants is associated with a range of negative developmental outcomes, including threats to the formation of a secure attachment.
The transition into parenthood is an ideal time for healthy behaviour change. Expectant parents see a range of professionals, but as we found in our new study, they don’t receive any co-ordinated support or advice on managing digital devices in babies’ presence.
One of the new mums we interviewed said:
Literally nothing has come up around […] screen time, or especially breastfeeding and things like that […] it’s interesting because it’s such a big part of our lives.
Another participant said:
I haven’t had anyone talk to me about tech use, at all.
Adult smartphone use is not mentioned in well-child checks. We argue this is a missed public health opportunity.
Secure attachment is important for a baby’s development. They need hours of gazing at their families’ faces to optimally wire their brains. This is more likely when the parent is sensitive to a baby’s cues and emotionally available.
But ubiquitous smartphone use by caregivers has the potential to disrupt attachment by interrupting this sensitivity and availability.
Babies’ central nervous system and senses are immature. But they are born into a rapidly moving world, filled with voices and faces from digital sources. This places a burden on caregivers to act as a human filter between a newborn’s neurobiology and digital distractions.
Getty Images Disrupting relationships
Psychologists have described the phenomenon of frequent disruptions and distractions during parenting – and the disconnection of the in-person relationship – as “technoference”.
A caregiver’s eyes are no longer on the infant but on the device. Their attention is gone, in a state described as “absent presence”, and the phone becomes a “social pollution”.
It’s unpleasant for anyone on the other side of this imbalance. But for babies, whose connection to their significant adults is the only thing that can make them feel safe enough to learn and grow optimally, it causes disproportionate harm because of their vulnerable developmental stage.
During the rapid phase of brain growth in infancy, babies are wired to seek messages of safety from their caregiver’s face. Smartphone use blanks caregivers’ facial expressions in ways that cause physiological stress to babies.
When a caregiver uses their phone while feeding an infant, babies are more likely to be overfed. The number of audible notifications on a parent’s device relates to a child’s language development, with more alerts associated with fewer words at 18 months.
If that’s not reason enough to reign in phone use, evidence also shows that smartphone use can be a source of stress and guilt for parents. This suggests parents themselves would benefit from more purposeful and reduced smartphone habits.
Some public health researchers are urging healthcare workers to consider the parent-infant relationship in addition to the respective health of the baby and caregiver themselves.
This relational space between people is suffering as a result of the social pollution of smartphone-distracted care. Babies’ brains grow so fast, we mustn’t let this process be compromised by the distraction of the attention economy.
Our research shows new parents could use information and support around the use of digital devices. We also recommend that other family members modify their smartphone habits around a new baby. Whānau can create a family media plan and make sure they have someone to talk to about this issue.
Health policies should focus on early investment in parents and children, by prioritising education and action on smartphone use around babies. This would benefit the wellbeing of new parents and the lifelong development of infants.
Miriam McCaleb, Fellow in Public Health, University of Canterbury
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



-

Unprocess Your Life – by Rob Hobson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Rob Hobson is not a doctor, but he is a nutritionist with half the alphabet after his name (BSc, PGDip, MSc, AFN, SENR) and decades of experience in the field.
The book covers, in jargon-free fashion, the science of ultra-processed foods, and why for example that pack of frozen chicken nuggets are bad but a pack of tofu (which obviously also took some processing, because it didn’t grow on the plant like that) isn’t.
This kind of explanation puts to rest a lot of the “does this count?” queries that a reader might have when giving the shopping list a once-over.
He also covers practical considerations such as kitchen equipment that’s worth investing in if you don’t already have it, and an “unprocessed pantry” shopping list.
The recipes (yes, there are recipes, nearly a hundred of them) are not plant-based by default, but there is a section of vegan and vegetarian recipes. Given that the theme of the book is replacing ultra-processed foods, it doesn’t mean a life of abstemiousness—there are recipes for all manner of things from hot sauce to cakes. Just, healthier unprocessed ones! There are classically healthy recipes too, of course.
Bottom line: if you’ve been wishing for a while that you could get rid of those processed products that are just so convenient that you haven’t got around to replacing them with healthier options, this book can indeed help you do just that.
Click here to check out Unprocess Your Life, and unprocess your life!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

I’m So Effing Tired – by Dr. Amy Shah
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s easy sometimes to feel like we know more or less what we should be doing… If only we had the energy to get going!
- We know we want a better diet… But we don’t have the time/energy to cook so will go for the quickest option even when it’s not the best?
- We know we should exercise… But feel we just need to crash out on the couch for a bit first?
- We would dearly love to get better sleep… But our responsibilities aren’t facilitating that?
…and so on. Happily, Dr. Amy Shah is here with ways to cut through the Gordian Knot that is this otherwise self-perpetuating cycle of exhaustion.
Most of the book is based around tackling what Dr. Shah calls “the energy trifecta“:
- Hormone levels
- Immune system
- Gut health
You’ll note (perhaps with relief) that none of these things require an initial investment of energy that you don’t have… She’s not asking you to hit the gym at 5am, or magically bludgeon your sleep schedule into its proper place, say.
Instead, what she gives is practical, actionable, easy changes that don’t require much effort, to gently slide us back into the fast lane of actually having energy to do stuff!
In short: if you’ve ever felt like you’d like to implement a lot of very common “best practice” lifestyle advice, but just haven’t had the energy to get going, there’s more value in this handbook than in a thousand motivational pep talks.
Click here to check out “I’m So Effing Tired” and get on a better track of life!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How safe are the chemicals in sunscreen? A pharmacology expert explains
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Last week, the Therapeutic Goods Administration (TGA) released its safety review of seven active ingredients commonly used in sunscreens.
It found five were low-risk and appropriate for use in sunscreens at their current concentrations.
However, the TGA recommended tighter restrictions on two ingredients – homosalate and oxybenzone – to reduce how much can be used in a product. This is based on uncertainty about their potential effects on the endocrine system, which creates and releases hormones.
This news, together with recent reports some products may have inflated their claims of SPF coverage, might make Australians worried about whether their sunscreen products are working – and safe.
But it’s not time to abandon sunscreens. In Australia, all sunscreens must pass a strict approval process before going on the market. The TGA tests the safety and efficacy of all ingredients, and this recent review is part of the TGA’s continuing commitment to safety.
The greatest threat sunscreen poses to Australians’ health is not using it.
Australia has the highest incidence of melanoma and non-melanoma skin cancer worldwide, and approximately 95% of melanoma cases in Australia are linked to ultraviolet (UV) exposure.
Still, it’s understandable people want to know what’s in their products, and any changes that might affect them. So let’s take a closer look at the safety review and what it found.
aquaArts studio/Getty What are the active ingredients in sunscreen?
There are two main types of sunscreen: physical and chemical. This is based on the different active ingredients they use.
An active ingredient is a chemical component in a product that has an effect on the body – basically, what makes the product “work”.
In sunscreens, this is the compound that absorbs UV rays from the Sun. The other ingredients – for example, those that give the sunscreen its smell or help the skin absorb it – are “inactive”.
Physical sunscreens typically use minerals, such as titanium dioxide and zinc oxide, that can absorb the Sun’s rays but also reflect some of them.
Chemical sunscreens use a variety of chemical ingredients to absorb or scatter UV light, both long wave (UVA) or short wave (UVB).
The seven active ingredients in this review are in chemical sunscreens.
Why did the TGA do the review?
Our current limits for the concentrations of these chemicals in sunscreen are generally consistent with other regulatory agencies, such as the European Union and the US Food and Drug Administration.
However, safety is an evolving subject. The TGA periodically reexamines the safety of all therapeutic goods.
Last year, the TGA revised its method of estimating sunscreen exposure to more closely model how skin is exposed to sunscreens over time.
This model considers how much sunscreen someone typically applies, how much skin they cover (whole body versus face and hands, or just face) and how it’s absorbed through the skin.
Given this new model – along with changes in the EU and US approaches to sunscreen regulation – the TGA selected seven common sunscreen ingredients to investigate in depth.
Determining what’s safe
When evaluating whether chemicals are safe for human use, testing will often consider studies in animals – especially when there is no or limited data on humans. These animal tests are done by the manufacturers, not the TGA.
To take into account any unforeseen sensitivity humans may have to these chemicals, a “margin of safety” is built in. This is typically a concentration 50–100 times lower than the dose at which no negative effect was seen in animals.
The sunscreen review used a margin of safety 100 times lower than this dose as the safety threshold.
For most of the seven investigated sunscreen chemicals, the TGA found the margin of safety was above 100.
This means they’re considered safe and low-risk for long-term use.
However, two ingredients, homosalate and oxybenzone, were found to be below 100. This was based on the highest estimated sunscreen exposure, applied to the body at the maximum permitted concentration: 15% for homosalate, 10% for oxybenzone.
At lower concentrations, other uses – such as just the hands and face – could be considered low-risk for both ingredients.
What are the health concerns?
Homosalate and oxybenzone have low acute oral toxicity – meaning you would need to swallow a lot of it to experience toxic effects, nearly half a kilogram of these chemicals – and don’t cause irritation to eyes or skin.
There is inconclusive evidence about oxybenzone potentially causing cancer in rats and mice – but only at concentrations to which humans will never be exposed via sunscreens.
The key issue is whether the two ingredients affect the endocrine system.
While effects have been seen at high concentrations in animal studies, it is not clear whether these translate to humans exposed to sunscreen levels.
No effect has been seen in clinical studies on fertility, hormones, weight gain and, in pregnant women, fetal development.
The TGA is being very cautious here, using a very wide margin of safety under worst-case scenarios.
What are the recommendations?
The TGA recommends the allowed concentration of homosalate and oxybenzone be reduced.
But exactly how much it will be lowered is complicated, depending on whether the product is intended for adults or children, specifically for face, or the whole body, and so on.
However, some sunscreens would need to be reformulated or warning labels placed on particular formulations. The exact changes will be decided after public consultation. Submissions close on August 12.
What about benzophenone?
There is also some evidence benzophenone – a chemical produced when sunscreen that contains octocrylene degrades – may cause cancer at high concentrations.
This is based on studies in which mice and rats were fed benzophenone well above the concentration in sunscreens.
Octocrylene degrades slowly over time to benzophenone. Heat makes it degrade faster, especially at temperatures above 40°C.
The TGA has recommended restricting benzophenone to 0.0383% in sunscreens to ensure it remains safe during the product’s shelf life.
The Cancer Council advises storing sunscreens below 30°C.
The bottom line
The proposed restrictions are very conservative, based on worst-case scenarios.
But even in worst-case scenarios, the margin of safety for these ingredients is still below the level at which any negative effect was seen in animals.
The threat of cancer from sun exposure is far more serious than any potential negative effect from sunscreens.
If you do wish to avoid these chemicals before new limits are imposed, several sunscreens are available that provide high levels of protection with little or no homosalate and oxybenzone. For more information, consult product labels.
Ian Musgrave, Senior Lecturer in Pharmacology, University of Adelaide
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: