The Drug & Supplement Combo That Reverses Aging
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
So far, its effects have been dramatic (in a good way) in mice; human trials are now underway.
How does it work?
It builds from previous work, in which a Japanese research team created an “anti-aging vaccine”, that responded to a problem more specific than aging as a whole, namely atherosclerosis.
They found that a certain* protein was upregulated (i.e., it was made at a greater rate resulting in greater quantities) in patients (mouse and human alike) with atherosclerosis. So, they immunized the mice against that protein, and long story short, everything improved for them, from their atherosclerosis to general markers of aging—including growing back fur that had been lost due to age-related balding (just like in humans). They also lived longer, as is to be expected of a mouse who is now biologically younger.
*To avoid being mysterious: it was glycoprotein nonmetastatic melanoma protein B, known to its friends as GPNMB.
You may be wondering: how can one be immunized against a protein? If so, do bear in mind, a virus is also a protein. In this case, they developed an RNA vaccine, that works in a similar way to the COVID vaccines we all know and love (albeit with a different target).
You can read about this in abundant detail here: Senolytic vaccination improves normal and pathological age-related phenotypes and increases lifespan in progeroid mice
Hot on the heels of that, new approaches were found, including…
The combination
We’ll not keep you waiting; the combination is dasatinib plus quercetin, or else fisetin alone.
It’s about killing senescent (aging) “zombie cells” while sparing healthy cells, which that drug (dasatinib) and those supplements (quercetin and fisetin) do.
The researchers noted:
❝Senescent cells are resistant to apoptosis, which is governed through the upregulation of senescent cell anti-apoptotic pathways (SCAPs). Compounds were subsequently identified that disrupted the SCAPs, inducing death of senescent cells while leaving healthy cells unaffected. Forty-six potential senolytic agents were discovered through this process. To advance translational efforts, the majority of research has focused on agents with known safety profiles and limited off-target effects (Kirkland and Tchkonia, 2020).
The best characterized senolytic agents are dasatinib, a tyrosine kinase inhibitor approved for use in humans for cancer treatment, and quercetin, a naturally occurring plant flavonoid. The agents have a synergistic effect, making their combination more potent for senescent cell clearance (Zhu et al., 2015). As senescent cells do not divide and accumulate over a period of weeks, they can be administered using an intermittent approach, which further serves to reduce the risk of side effects (Kirkland and Tchkonia, 2020).
In preclinical trials, the combination of dasatinib and quercetin (D + Q) have been found to alleviate numerous chronic medical conditions including vascular stiffness, osteoporosis, frailty, and hepatic stenosis❞
Source: A geroscience motivated approach to treat Alzheimer’s disease: Senolytics move to clinical trials
As to how they expanded on this research:
❝In our study, oral D + Q were intermittently administered to tau transgenic mice with late-stage pathology (approximated to a 70-year-old human with advanced AD) (Musi et al., 2018). The treatment effectively reduced cellular senescence and associated senescence-associated secretory phenotype incidence. The 35 % reduction in neurofibrillary tangles was accompanied by enhanced neuron density, decreased ventricular enlargement, diminished tau accumulation, and restoration of aberrant cerebral blood flow. A subsequent preclinical study validated the findings, reporting that intermittently administered D + Q cleared senescent cells in the central nervous system, reduced amyloid-β plaques, attenuated neuroinflammation, and enhanced cognition❞
Source: Ibid.
And now taking it to humans:
❝The first clinical trial of D + Q for early-stage Alzheimer’s Disease (AD) has completed enrollment (Gonzales et al., 2021). The primary aim of the open-label pilot study was to examine the central nervous system penetrance of D and Q in a small sample of older adults with early-stage AD (NCT04063124). In addition, two placebo-controlled trials of D + Q for neurodegenerative disease are underway (NCT04685590 and NCT04785300).
One of the trials in development is a multi-site, double-blind, randomized, placebo-controlled study of senolytic therapy in older adults with amnestic mild cognitive impairment (MCI) or early-stage dementia (Clinical Dementia Rating Scale (CDR) Global 0.5–1) due to AD (elevated CSF total tau/Aβ42 ratio).
The treatment regimen will consist of 12-weeks of intermittently administered oral D + Q.❞
Source: Ibid.
The study is actually completed now, but its results are not yet published (again, at time of writing). Which means: they have the data, and now they’re writing the paper.
We look forward to providing an update about that, when the paper is published!
In the meantime…
Dasatinib is a drug usually prescribed to people with certain kinds of leukemia, and suffice it to say, it’s prescription-only. And unlike drugs that are often prescribed off-label (such as metformin for weight loss), getting your doctor to prescribe you an anticancer drug is unlikely unless you have the cancer in question.
You may be wondering: how is an anticancer drug helpful against aging? And the answer is that cancer and aging are very interrelated, and both have to do with “these old cells just won’t die, and are using the resources needed for young healthy cells”. So in both cases, killing those “zombie cells” while sparing healthy ones, is what’s needed. However, your doctor will probably not buy that as a reason to prescribe you a drug that is technically chemotherapy.
Quercetin, on the other hand, is a readily-available supplement, as is fisetin, and both have glowing (in a good way) safety profiles.
Want to know more?
You can read more about each of quercetin and fisetin (including how to get them), here:
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

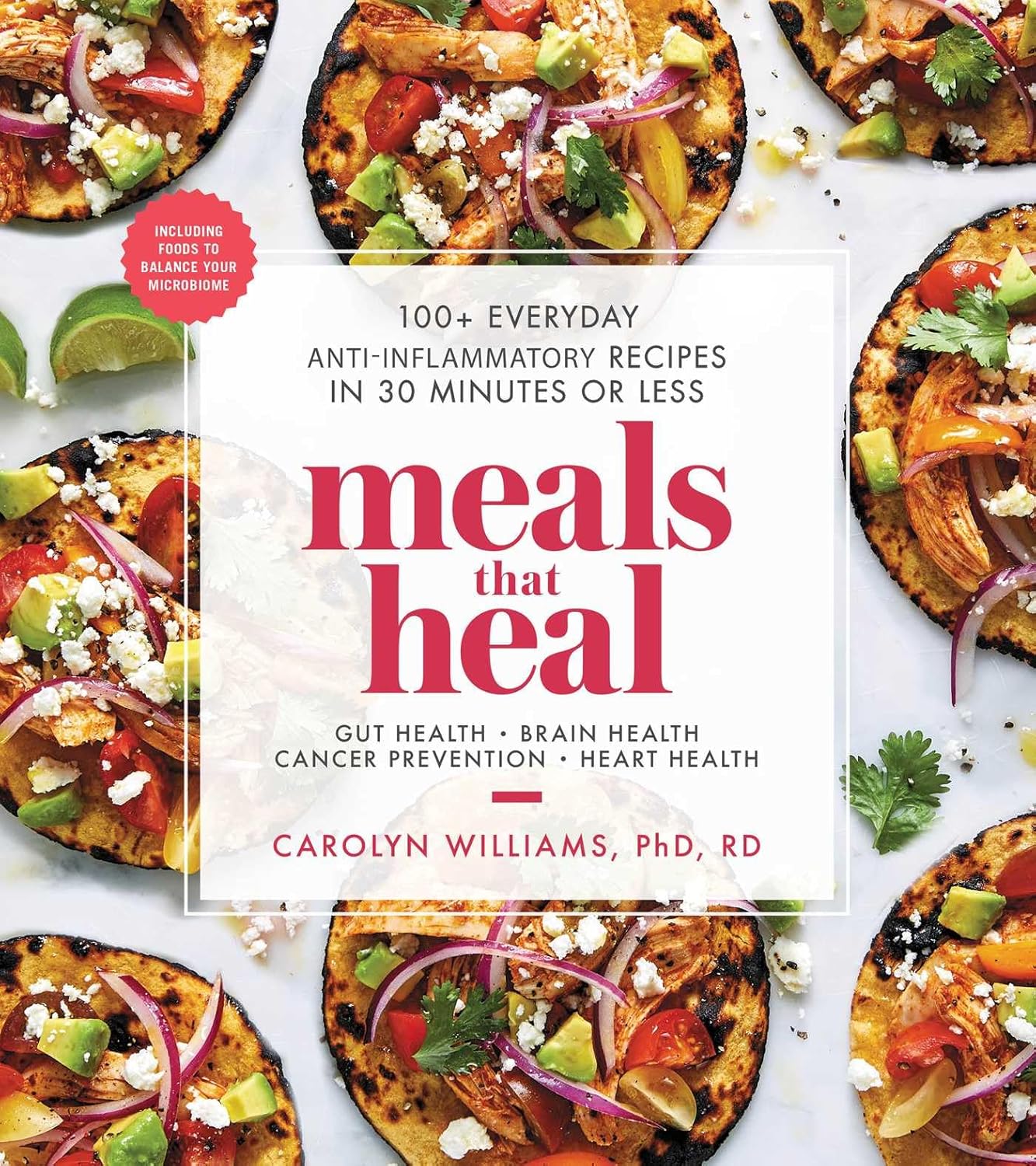
Meals That Heal – by Dr. Carolyn Williams

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Inflammation is implicated as a contributory or casual factor in almost all chronic diseases (and still exacerbates the ones in which it’s not directly implicated causally), so if there’s one area of health to focus on with one’s diet, then reducing inflammation is a top candidate.
This book sets about doing exactly that.
You may be wondering whether, per the book’s subtitle, they can really all be done in 30 minutes or under. The answer is: no, not unless you have a team of sous-chefs to do all the prep work for you, and line up everything mise-en-place style for when you start the clock. If you do have that team of sous-chefs working for you, then you can probably do most of them in under 30 minutes. If you don’t have that team, then budget about an hour in total, sometimes less, sometimes more, depending on the recipe.
The recipes themselves are mostly Mediterranean-inspired, though you might want to do a few swaps where the author has oddly recommended using seed oils instead of olive oil, or plant milk in place of where she has used dairy milk in a couple of “recipes” for smoothies. You might also want to be a little more generous with the seasonings, if you’re anything like this reviewer.
Bottom line: if you’re looking for an anti-inflammatory starter cookbook, you could do worse than this. You could probably do better, too, such as starting with The Inflammation Spectrum – by Dr. Will Cole.
Alternatively, click here if you want to check out Meals That Heal, and dive straight in!
Share This Post
-

Life After Death? (Your Life; A Loved One’s Death)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Show Must Go On
We’ve previously written about the topics of death and dying. It’s not cheery, but it is important to tackle.
Sooner is better than later, in the case of:
Preparations For Managing Your Own Mortality
And for those who are left behind, of course it is hardest of all:
What Grief Does To Your Body (And How To Manage It)
But what about what comes next? For those who are left behind, that is.
Life goes on
In cases when the death is that of a close loved one, the early days after death can seem like a surreal blur. How can the world go ticking on as normal when [loved one] is dead?
But incontrovertibly, it does, so we can only ask again: how?
And, we get to choose that, to a degree. The above-linked article about grief gives a “101” rundown, but it’s (by necessity, for space) a scant preparation for one of the biggest challenges in life that most of us will ever face.
For many people, processing grief involves a kind of “saying goodbye”. For others, it doesn’t, as in the following cases of grieving the loss of one’s child—something no parent should ever have to face, but it happens:
Dr. Ken Druck | The Love That Never Dies
(with warning, the above article is a little heavy)
In short: for those who choose not to “say goodbye” in the case of the death of a loved one, it’s more often not a case of cold neglect, but rather the opposite—a holding on. Not in the “denial” sense of holding on, but rather in the sense of “I am not letting go of this feeling of love, no matter how much it might hurt to hold onto; it’s all I have”.
What about widows, and love after death?
Note: we’ll use the feminine “widow” here as a) it’s the most common and b) most scientific literature focuses on widows, but there is no reason why most of the same things won’t also apply to widowers.
We say “most”, as society does tend to treat widows and widowers differently, having different expectations about a respectful mourning period, one’s comportment during same, and so on.
As an aside: most scientific literature also assumes heterosexuality, which is again statistically reasonable, and for the mostpart the main difference is any extra challenges presented by non-recognition of marriages, and/or homophobic in-laws. But otherwise, grief is grief, and as the saying goes, love is love.
One last specificity before we get into the meat of this: we are generally assuming marriages to be monogamous here. Polyamorous arrangements will likely sidestep most of these issues completely, but again, they’re not the norm.
Firstly, there’s a big difference between remarrying (or similar) after being widowed, and remarrying (or similar) after a divorce, and that largely lies in the difference of how they begin. A divorce is (however stressful it may often be) more often seen as a transition into a new period of freedom, whereas bereavement is almost always felt as a terrible loss.
The science, by the way, shows the stats for this; people are less likely to remarry, and slower to remarry if they do, in instances of bereavement rather than divorce, for example:
Timing of Remarriage Among Divorced and Widowed Parents
Love after death: the options
For widows, then, there seem to be multiple options:
- Hold on to the feelings for one’s deceased partner; never remarry
- Grieve, move on, find new love, relegating the old to history
- Try to balance the two (this is tricky but can be done*)
*Why is balancing the two tricky, and how can it be done?
It’s tricky because ultimately there are three people’s wishes at hand:
- The deceased (“they would want me to be happy” vs “I feel I would be betraying them”—which two feelings can also absolutely come together, by the way)
- Yourself (whether you actually want to get a new partner, or just remain single—this is your 100% your choice either way, and your decision should be made consciously)
- The new love (how comfortable are they with your continued feelings for your late love, really?)
And obviously only two of the above can be polled for opinions, and the latter one might say what they think we want to hear, only to secretly and/or later resent it.
One piece of solid advice for the happily married: talk with your partner now about how you each would feel about the other potentially remarrying in the event of your death. Do they have your pre-emptive blessing to do whatever, do you ask a respectable mourning period first (how long?), would the thought just plain make you jealous? Be honest, and bid your partner be honest too.
One piece of solid advice for everyone: make sure you, and your partner(s), as applicable, have a good emotional safety net, if you can. Close friends or family members that you genuinely completely trust to be there through thick and thin, to hold your/their hand through the emotional wreck that will likely follow.
Because, while depression and social loneliness are expected and looked out for, it’s emotional loneliness that actually hits the hardest, for most people:
Longitudinal Examination of Emotional Functioning in Older Adults After Spousal Bereavement
…which means that having even just one close friend or family member with whom one can be at one’s absolute worst, express emotions without censure, not have to put on the socially expected appearance of emotional stability… Having that one person (ideally more, but having at least one is critical) can make a huge difference.
But what if a person has nobody?
That’s definitely a hard place to be, but here’s a good starting point:
How To Beat Loneliness & Isolation
Take care!
Share This Post
-

What’s the difference between a heart attack and cardiac arrest? One’s about plumbing, the other wiring
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In July 2023, rising US basketball star Bronny James collapsed on the court during practice and was sent to hospital. The 18-year-old athlete, son of famous LA Lakers’ veteran LeBron James, had experienced a cardiac arrest.
Many media outlets incorrectly referred to the event as a “heart attack” or used the terms interchangeably.
A cardiac arrest and a heart attack are distinct yet overlapping concepts associated with the heart.
With some background in how the heart works, we can see how they differ and how they’re related.

Explode/Shutterstock Understanding the heart
The heart is a muscle that contracts to work as a pump. When it contracts it pushes blood – containing oxygen and nutrients – to all the tissues of our body.
For the heart muscle to work effectively as a pump, it needs to be fed its own blood supply, delivered by the coronary arteries. If these arteries are blocked, the heart muscle doesn’t get the blood it needs.
This can cause the heart muscle to become injured or die, and results in the heart not pumping properly.
Heart attack or cardiac arrest?
Simply put, a heart attack, technically known as a myocardial infarction, describes injury to, or death of, the heart muscle.
A cardiac arrest, sometimes called a sudden cardiac arrest, is when the heart stops beating, or put another way, stops working as an effective pump.
In other words, both relate to the heart not working as it should, but for different reasons. As we’ll see later, one can lead to the other.
Why do they happen? Who’s at risk?
Heart attacks typically result from blockages in the coronary arteries. Sometimes this is called coronary artery disease, but in Australia, we tend to refer to it as ischaemic heart disease.
The underlying cause in about 75% of people is a process called atherosclerosis. This is where fatty and fibrous tissue build up in the walls of the coronary arteries, forming a plaque. The plaque can block the blood vessel or, in some instances, lead to the formation of a blood clot.
Atherosclerosis is a long-term, stealthy process, with a number of risk factors that can sneak up on anyone. High blood pressure, high cholesterol, diet, diabetes, stress, and your genes have all been implicated in this plaque-building process.
Other causes of heart attacks include spasms of the coronary arteries (causing them to constrict), chest trauma, or anything else that reduces blood flow to the heart muscle.
Regardless of the cause, blocking or reducing the flow of blood through these pipes can result in the heart muscle not receiving enough oxygen and nutrients. So cells in the heart muscle can be injured or die.
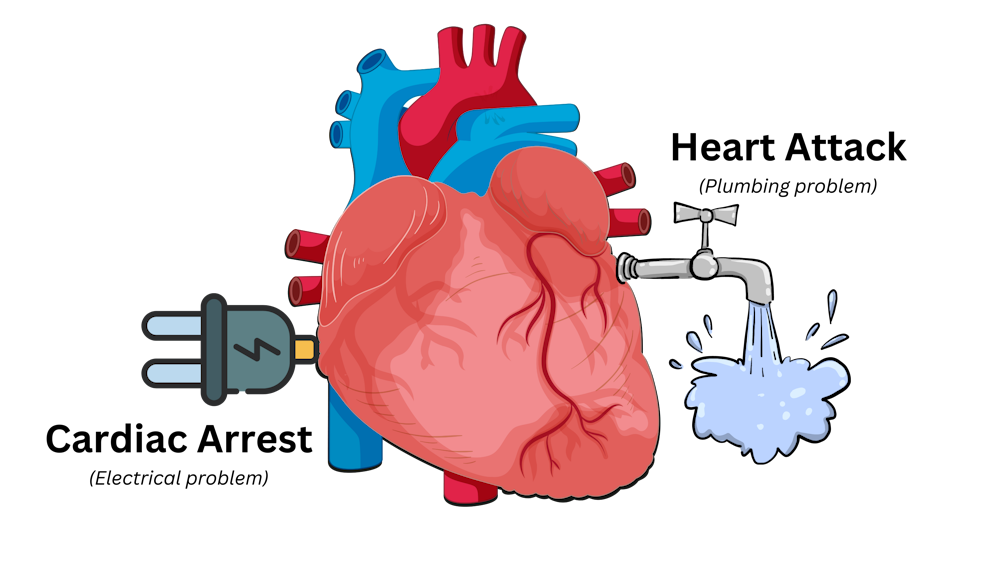
Here’s a simple way to remember the difference. Author provided But a cardiac arrest is the result of heartbeat irregularities, making it harder for the heart to pump blood effectively around the body. These heartbeat irregularities are generally due to electrical malfunctions in the heart. There are four distinct types:
- ventricular tachycardia: a rapid and abnormal heart rhythm in which the heartbeat is more than 100 beats per minute (normal adult, resting heart rate is generally 60-90 beats per minute). This fast heart rate prevents the heart from filling with blood and thus pumping adequately
- ventricular fibrillation: instead of regular beats, the heart quivers or “fibrillates”, resembling a bag of worms, resulting in an irregular heartbeat greater than 300 beats per minute
- pulseless electrical activity: arises when the heart muscle fails to generate sufficient pumping force after electrical stimulation, resulting in no pulse
- asystole: the classic flat-line heart rhythm you see in movies, indicating no electrical activity in the heart.
Remember this flat-line rhythm from the movies? It’s asystole, when there’s no electrical activity in the heart. Kateryna Kon/Shutterstock Cardiac arrest can arise from numerous underlying conditions, both heart-related and not, such as drowning, trauma, asphyxia, electrical shock and drug overdose. James’ cardiac arrest was attributed to a congenital heart defect, a heart condition he was born with.
But among the many causes of a cardiac arrest, ischaemic heart disease, such as a heart attack, stands out as the most common cause, accounting for 70% of all cases.
So how can a heart attack cause a cardiac arrest? You’ll remember that during a heart attack, heart muscle can be damaged or parts of it may die. This damaged or dead tissue can disrupt the heart’s ability to conduct electrical signals, increasing the risk of developing arrhythmias, possibly causing a cardiac arrest.
So while a heart attack is a common cause of cardiac arrest, a cardiac arrest generally does not cause a heart attack.
What do they look like?
Because a cardiac arrest results in the sudden loss of effective heart pumping, the most common signs and symptoms are a sudden loss of consciousness, absence of pulse or heartbeat, stopping of breathing, and pale or blue-tinged skin.
But the common signs and symptoms of a heart attack include chest pain or discomfort, which can show up in other regions of the body such as the arms, back, neck, jaw, or stomach. Also frequent are shortness of breath, nausea, light-headedness, looking pale, and sweating.
What’s the take-home message?
While both heart attack and cardiac arrest are disorders related to the heart, they differ in their mechanisms and outcomes.
A heart attack is like a blockage in the plumbing supplying water to a house. But a cardiac arrest is like an electrical malfunction in the house’s wiring.
Despite their different nature both conditions can have severe consequences and require immediate medical attention.
Michael Todorovic, Associate Professor of Medicine, Bond University and Matthew Barton, Senior lecturer, School of Nursing and Midwifery, Griffith University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post


-

How Does One Test Acupuncture Against Placebo Anyway?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Pinpointing The Usefulness Of Acupuncture

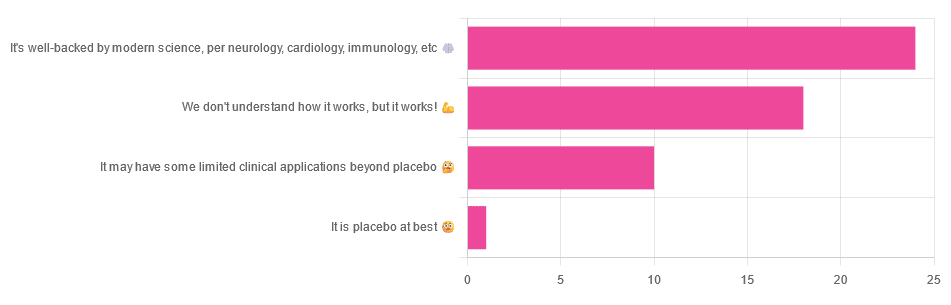
We asked you for your opinions on acupuncture, and got the above-depicted, below-described, set of answers:
- A little under half of all respondents voted for “It’s well-backed by modern science, per neurology, cardiology, immunology, etc”
- Slightly fewer respondents voted for “We don’t understand how it works, but it works!”
- A little under a fifth of respondents voted for “It may have some limited clinical applications beyond placebo”
- One (1) respondent voted for for “It’s placebo at best”
When we did a main feature about homeopathy, a couple of subscribers wrote to say that they were confused as to what homeopathy was, so this time, we’ll start with a quick definition first.
First, what is acupuncture? For the convenience of a quick definition so that we can move on to the science, let’s borrow from Wikipedia:
❝Acupuncture is a form of alternative medicine and a component of traditional Chinese medicine in which thin needles are inserted into the body.
Acupuncture is a pseudoscience; the theories and practices of TCM are not based on scientific knowledge, and it has been characterized as quackery.❞
Now, that’s not a promising start, but we will not be deterred! We will instead examine the science itself, rather than relying on tertiary sources like Wikipedia.
It’s worth noting before we move on, however, that there is vigorous debate behind the scenes of that article. The gist of the argument is:
- On one side: “Acupuncture is not pseudoscience/quackery! This has long been disproved and there are peer-reviewed research papers on the subject.”
- On the other: “Yes, but only in disreputable quack journals created specifically for that purpose”
The latter counterclaim is a) potentially a “no true Scotsman” rhetorical ploy b) potentially true regardless
Some counterclaims exhibit specific sinophobia, per “if the source is Chinese, don’t believe it”. That’s not helpful either.
Well, the waters sure are muddy. Where to begin? Let’s start with a relatively easy one:
It may have some clinical applications beyond placebo: True or False?
True! Admittedly, “may” is doing some of the heavy lifting here, but we’ll take what we can get to get us going.
One of the least controversial uses of acupuncture is to alleviate chronic pain. Dr. Vickers et al, in a study published under the auspices of JAMA (a very respectable journal, and based in the US, not China), found:
❝Acupuncture is effective for the treatment of chronic pain and is therefore a reasonable referral option. Significant differences between true and sham acupuncture indicate that acupuncture is more than a placebo.
However, these differences are relatively modest, suggesting that factors in addition to the specific effects of needling are important contributors to the therapeutic effects of acupuncture❞
Source: Acupuncture for Chronic Pain: Individual Patient Data Meta-analysis
If you’re feeling sharp today, you may be wondering how the differences are described as “significant” and “relatively modest” in the same text. That’s because these words have different meanings in academic literature:
- Significant = p<0.05, where p is the probability of the achieved results occurring randomly
- Modest = the differences between the test group and the control group were small
In other words, “significant modest differences” means “the sample sizes were large, and the test group reliably got slightly better results than placebo”
We don’t understand how it works, but it works: True or False
Broadly False. When it works, we generally have an idea how.
Placebo is, of course, the main explanation. And even in examples such as the above, how is placebo acupuncture given?
By inserting acupuncture needles off-target rather than in accord with established meridians and points (the lines and dots that, per Traditional Chinese Medicine, indicate the flow of qi, our body’s vital energy, and welling-points of such).
So, if a patient feels that needles are being inserted randomly, they may no longer have the same confidence that they aren’t in the control group receiving placebo, which could explain the “modest” difference, without there being anything “to” acupuncture beyond placebo. After all, placebo works less well if you believe you are only receiving placebo!
Indeed, a (Korean, for the record) group of researchers wrote about this—and how this confounding factor cuts both ways:
❝Given the current research evidence that sham acupuncture can exert not only the originally expected non-specific effects but also sham acupuncture-specific effects, it would be misleading to simply regard sham acupuncture as the same as placebo.
Therefore, researchers should be cautious when using the term sham acupuncture in clinical investigations.❞
Source: Sham Acupuncture Is Not Just a Placebo
It’s well-backed by modern science, per neurology, cardiology, immunology, etc: True or False?
False, for the most part.
While yes, the meridians and points of acupuncture charts broadly correspond to nerves and vasculature, there is no evidence that inserting needles into those points does anything for one’s qi, itself a concept that has not made it into Western science—as a unified concept, anyway…
Note that our bodies are indeed full of energy. Electrical energy in our nerves, chemical energy in every living cell, kinetic energy in all our moving parts. Even, to stretch the point a bit, gravitational potential energy based on our mass.
All of these things could broadly be described as qi, if we so wish. Indeed, the ki in the Japanese martial art of aikido is the latter kinds; kinetic energy and gravitational potential energy based on our mass. Same goes, therefore for the ki in kiatsu, a kind of Japanese massage, while the ki in reiki, a Japanese spiritual healing practice, is rather more mystical.
The qi in Chinese qigong is mostly about oxygen, thus indirectly chemical energy, and the electrical energy of the nerves that are receiving oxygenated blood at higher or lower levels.
On the other hand, the efficacy of the use of acupuncture for various kinds of pain is well-enough evidenced. Indeed, even the UK’s famously thrifty NHS (that certainly would not spend money on something it did not find to work) offers it as a complementary therapy for some kinds of pain:
❝Western medical acupuncture (dry needling) is the use of acupuncture following a medical diagnosis. It involves stimulating sensory nerves under the skin and in the muscles.
This results in the body producing natural substances, such as pain-relieving endorphins. It’s likely that these naturally released substances are responsible for the beneficial effects experienced with acupuncture.❞
Source: NHS | Acupuncture
Meanwhile, the NIH’s National Cancer Institute recommends it… But not as a cancer treatment.
Rather, they recommend it as a complementary therapy for pain management, and also against nausea, for which there is also evidence that it can help.
Frustratingly, while they mention that there is lots of evidence for this, they don’t actually link the studies they’re citing, or give enough information to find them. Instead, they say things like “seven randomized clinical trials found that…” and provide links that look reassuring until one finds, upon clicking on them, that it’s just a link to the definition of “randomized clinical trial”:
Source: NIH | Nactional Cancer Institute | Acupuncture (PDQ®)–Patient Version
However, doing our own searches finds many studies (mostly in specialized, potentially biased, journals such as the Journal of Acupuncture and Meridian Studies) finding significant modest outperformance of [what passes for] placebo.
Sometimes, the existence of papers with promising titles, and statements of how acupuncture might work for things other than relief of pain and nausea, hides the fact that the papers themselves do not, in fact, contain any evidence to support the hypothesis. Here’s an example:
❝The underlying mechanisms behind the benefits of acupuncture may be linked with the regulation of the hypothalamic-pituitary-gonadal (adrenal) axis and activation of the Wnt/β-catenin and OPG/RANKL/RANK signaling pathways.
In summary, strong evidence may still come from prospective and well-designed clinical trials to shed light on the potential role of acupuncture in preserving bone loss❞
Source: Acupuncture for Osteoporosis: a Review of Its Clinical and Preclinical Studies
So, here they offered a very sciencey hypothesis, and to support that hypothesis, “strong evidence may still come”.
“We must keep faith” is not usually considered evidence worthy of inclusion in a paper!
PS: the above link is just to the abstract, because the “Full Text” link offered in that abstract leads to a completely unrelated article about HIV/AIDS-related cryptococcosis, in a completely different journal, nothing to do with acupuncture or osteoporosis).
Again, this is not the kind of professionalism we expect from peer-reviewed academic journals.
Bottom line:
Acupuncture reliably performs slightly better than sham acupuncture for the management of pain, and may also help against nausea.
Beyond placebo and the stimulation of endorphin release, there is no consistently reliable evidence that is has any other discernible medical effect by any mechanism known to Western science—though there are plenty of hypotheses.
That said, absence of evidence is not evidence of absence, and the logistical difficulty of testing acupuncture against placebo makes for slow research. Maybe one day we’ll know more.
For now:
- If you find it helps you: great! Enjoy
- If you think it might help you: try it! By a licensed professional with a good reputation, please.
- If you are not inclined to having needles put in you unnecessarily: skip it! Extant science suggests that at worst, you’ll be missing out on slight relief of pain/nausea.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Unlock Your Flexibility With These 4 New Stretches
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
People often stick to the same few stretches, which may limit flexibility progress, especially as the most common stretches often miss deeper, harder-to-reach areas.
So, here are some new (well, probably new to most people, at least) stretches that can get things moving in different directions:
Diversity Continues To Be Good!
The stretches are:
90/90 Hip stretch with a twist:
- Sit with your knees forming 90° angles; add an arm bar and twist your chest upward.
- Hold for 5 deep breaths and repeat.
- This one targets top glute muscles and quadratus lumborum in the lower back.
Shoulder mobility stretch using a wall:
- Kneel in front of a wall with your forearms placed shoulder-width apart, hands turned outward.
- Lift your hips, push your chest toward your legs, and use the wall and your body weight for deeper leverage.
- This one targets multiple shoulder and rotator cuff muscles through external rotation.
Quad stretch using body weight:
- Sit with your feet hip-width apart, lift your hips, step one foot back, and tuck in your tailbone.
- Focus on pointing your knee down and forward for a deep quad stretch.
- This one targets all four quad muscles, hip flexors, plantar fascia, and opens chest/shoulders.
Chicken wing stretch for upper back:
- Sit with bent knees, place the back of one hand on your waist (chicken wing position).
- Tuck the “wing” into the inner thigh, press your knee inward while resisting with the arm.
- This one broadens the shoulder blade and stretches rear shoulder/upper back muscles; it’s particularly effective for reaching difficult upper back areas not typically stretched.
For more on each of these plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Yoga Teacher: “If I wanted to get flexible in 2025, here’s what I’d do”
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Dealing with Thirst!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Busting The Myth of “Eight Glasses Of Water A Day”
Everyone knows we must drink 8 glasses of water a day, or else we’re going to get a failing grade at being a healthy human—like not flossing, or not using adequate sunscreen.
But… Do we? And does tea count? How about (we dare but whisper it) coffee? And soda drinks are mostly water, right? But aren’t some drinks dehydrating? Are special electrolyte drinks really better? There are so many things to consider, so many differing advices, and it’s easy to give up, or just choose what to believe in as a leap of faith.
A quick brain-teaser for you first, though:
If coffee and soda don’t count because they’re dehydrating, then what if you were to take:
– A concentrated tiny cup of espresso, and then a glass of water, would the glass of water count?
– Or (we don’t relish the thought) what if you took a spoonful of soda syrup, and then a glass of water, would the glass of water count?
If your answer was “yes, it’s a glass of water”, then why would it not count if it were taken all at once (e.g. as an Americano coffee, or a regular soda)?
If your answer was “yes, but that water might only offset the dehydration caused by the coffee/syrup, so I might only be breaking even”, then you were thinking about this the right way:
How much water you need depends on many factors that can be affected by what else you are consuming and what else you are doing. Science loves averages, so eight glasses a day may be great if you are of average health, and average body size, in a temperate climate, doing moderate exercise, and so on and so on.
If you’re not the most average person of all time? You may need to take into account a lot of factors, ranging from what you ate for dinner to how much you perspired during your morning exercises. As you (probably) don’t live in laboratory conditions, this can become an impossible task—and if you missed (or guessed incorrectly) even one factor, the whole calculation will be thrown off. But is there any other way to know?
What of the infamous pee test? Drink enough to make your urine as clear as possible, and if it’s dark, you’re dehydrated, common wisdom says.
In reality, however, that tells you not what’s in your body, but rather, what got ejected from your body. If your urine is dark, it might mean you had too little water, but it also could just mean you had the right amount of water but too much sodium, for instance. A study of this was done on athletes, and found no correlation between urine color and actual bodily hydration when measured directly via a blood test.
So, if we can’t just have an app tell us “drink this many glasses of water”, and we can’t trust urine color, what can we do?
What we can do is trust that our body comes with (for free!) a wonderful homeostatic system and it will try to correct any imbalances. If you are thirsty, you’re dehydrated. Drink something with plenty of water in, if not plain water.
But what about special electrolyte drinks? If you need salts, you will crave them. Craving a salty snack? Go for it! Or if you prefer not to snack, do a salt lick test (just put a little salt on your finger, and taste it; if it tastes good, wait a minute or two, and then have a little more, and repeat until it doesn’t).
Bonus Tip:
- Make sure you always have a source of hydration (that you enjoy!) to hand. Maybe it’s chilled water, maybe it’s a pot of tea, maybe it’s a sports drink, it doesn’t matter too much. Even coffee is actually fine, by the way (but don’t overdo it).
- Make a personal rule: “I will always make time for hydration”. That means, if you’re thirsty, have something with water in it now. Not when you’ve finished what you’re doing (unless you really can’t stop, because you are a racecar driver mid-race, or a surgeon mid-operation, or something), but now. Do not postpone it until after you’ve done some other thing first; you will forget and it will keep getting postponed. Always make time for water.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: