10 Tips To Reduce Morning Pain & Stiffness With Arthritis
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Physiotherapist and osteoarthritis specialist Dr. Alyssa Kuhn has professional advice:
Just the tips
We’ll not keep them a mystery; they are:
- Perform movements that target the range of motion in stiff joints, especially in knees and hips, to prevent them from being stuck in limited positions overnight.
- Use relaxation techniques like a hot shower, heating pad, or light reading before bed to reduce muscle tension and stiffness upon waking.
- Manage joint swelling during the day through gentle movement, compression sleeves, and self-massage .
- Maintain a balanced level of activity throughout the day to avoid excessive stiffness from either overactivity or, on the flipside, prolonged inactivity.
- Use pillows to support joints, such as placing one between your knees for hip and knee arthritis, and ensure you have a comfortable pillow for neck support.
- Eat anti-inflammatory foods prioritizing fruits and vegetables to reduce joint stiffness, and avoid foods high in added sugar, trans-fats, and saturated fats.
- Perform simple morning exercises targeting stiff areas to quickly relieve stiffness and ease into your daily routine.
- Engage in strength training exercises 2–3 times per week to build stronger muscles around the joints, which can reduce stiffness and pain.
- Ensure you get 7–8 hours of restful sleep, as poor sleep can increase stiffness and pain sensitivity the next day. 10almonds note: we realize there’s a degree of “catch 22” here, but we’re simply reporting her advice. Of course, do what you can to prioritize being able to get the best quality sleep you can.
- Perform gentle movements or stretches before bed to keep joints limber, focusing on exercises that feel comfortable and soothing.
For more on each of these plus some visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Avoiding/Managing Osteoarthritis
- Avoiding/Managing Rheumatoid Arthritis
- Managing Chronic Pain (Realistically!)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Walnuts vs Cashews – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing walnuts to cashews, we picked the walnuts.
Why?
It was close! In terms of macros, walnuts have about 2x the fiber, while cashews have slightly more protein. In the specific category of fats, walnuts have more fat. Looking further into it: walnuts’ fats are mostly polyunsaturated, while cashews’ fats are mostly monounsaturated, both of which are considered healthy.
Notwithstanding being both high in calories, neither nut is associated with weight gain—largely because of their low glycemic indices (of which, walnuts enjoy the slightly lower GI, but both are low-GI foods)
When it comes to vitamins, walnuts have more of vitamins A, B2, B3 B6, B9, and C, while cashews have more of vitamins B1, B5, E, and K. Because of the variation in their respective margins of difference, this is at best a moderate victory for walnuts, though.
In the category of minerals, cashews get their day, as walnuts have more calcium and manganese, while cashews have more copper, iron, magnesium, phosphorus, potassium, selenium, and zinc.
In short: unless you’re allergic, we recommend enjoying both of these nuts (and others) for a full range of benefits. However, if you’re going to pick one, walnuts win the day.
Want to learn more?
You might like to read:
Why You Should Diversify Your Nuts
Take care!
Share This Post
-

Health Benefits Of Cranberries (But: You’d Better Watch Out)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Health Benefits Of Cranberries (But: You’d Better Watch Out)
Quick clarification first: today we’re going to be talking about cranberries. Not “cranberry juice drink” that is loaded with sugar, nor “cranberry jelly” or similar that is more added sugar than it is cranberry.
We’re going to keep this short today, because “eat berries” is probably something you know already, but there are some things you should be aware of!
The benefits
Cranberries, even more than most berries, are full of polyphenols and flavonoids that do “those three things that usually come together”: antioxidant properties, anti-inflammatory properties, and anti-cancer properties
Unsurprisingly, this also means they’re good for the immune system and thus quite a boon in flu season:
They’re also good for heart health:
Quick Tip: we’re giving you one study for each of these things for brevity, but if you click through on any of our PubMed study links, you’ll (almost) always see a heading “Similar articles” heading beneath it, which will (almost) always show you plenty more.
Perhaps the most popular reason people take cranberry supplements, though, is their effectiveness at prevention of urinary tract infections:
Indeed, their effectiveness is such that researchers have considered them a putative alternative to antibiotics, particularly in individuals with recurrent UTIs:
Is it safe?
Cranberries are generally considered a very healthful food. However, there are two known possible exceptions:
If you are taking warfarin, it is possible that cranberry consumption may cause additional anti-clotting effects that you don’t want.
If you are at increased risk of kidney stones, the science is currently unclear as to whether this will help or hinder:
- Influence of cranberry juice on the urinary risk factors for calcium oxalate kidney stone formation ← this one concluded “Cranberry juice has antilithogenic properties and, as such, deserves consideration as a conservative therapeutic protocol in managing calcium oxalate urolithiasis”
- Dietary supplementation with cranberry concentrate tablets may increase the risk of nephrolithiasis ← this one, as you can see, concluded the opposite
- Safety of Cranberry: Evaluation of Evidence of Kidney Stone Formation and Botanical Drug-Interactions ← this one acknowledges “contradictory data regarding the role of cranberry in kidney stone formation”
Where can I get some?
You can probably buy fresh, frozen, or dried cranberries from wherever you normally do your grocery shopping.
However, if you prefer to take it in supplement form, then here’s an example product on Amazon
Enjoy!
Share This Post
-
Unlock Your Flexibility With These 4 New Stretches
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
People often stick to the same few stretches, which may limit flexibility progress, especially as the most common stretches often miss deeper, harder-to-reach areas.
So, here are some new (well, probably new to most people, at least) stretches that can get things moving in different directions:
Diversity Continues To Be Good!
The stretches are:
90/90 Hip stretch with a twist:
- Sit with your knees forming 90° angles; add an arm bar and twist your chest upward.
- Hold for 5 deep breaths and repeat.
- This one targets top glute muscles and quadratus lumborum in the lower back.
Shoulder mobility stretch using a wall:
- Kneel in front of a wall with your forearms placed shoulder-width apart, hands turned outward.
- Lift your hips, push your chest toward your legs, and use the wall and your body weight for deeper leverage.
- This one targets multiple shoulder and rotator cuff muscles through external rotation.
Quad stretch using body weight:
- Sit with your feet hip-width apart, lift your hips, step one foot back, and tuck in your tailbone.
- Focus on pointing your knee down and forward for a deep quad stretch.
- This one targets all four quad muscles, hip flexors, plantar fascia, and opens chest/shoulders.
Chicken wing stretch for upper back:
- Sit with bent knees, place the back of one hand on your waist (chicken wing position).
- Tuck the “wing” into the inner thigh, press your knee inward while resisting with the arm.
- This one broadens the shoulder blade and stretches rear shoulder/upper back muscles; it’s particularly effective for reaching difficult upper back areas not typically stretched.
For more on each of these plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Yoga Teacher: “If I wanted to get flexible in 2025, here’s what I’d do”
Take care!
Share This Post
Related Posts
-

Which Osteoporosis Medication, If Any, Is Right For You?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Which Osteoporosis Medication, If Any, Is Right For You?
We’ve written about osteoporosis before, so here’s a quick recap first in case you missed these:
- The Bare-bones Truth About Osteoporosis
- Exercises To Do (And Exercises To Avoid) If You Have Osteoporosis
- We Are Such Stuff As Fish Are Made Of
- Vit D + Calcium: Too Much Of A Good Thing?
All of those look and diet and/or exercise, with “diet” including supplementation. But what of medications?
So many choices (not all of them right for everyone)
The UK’s Royal Osteoporosis Society says of the very many osteoporosis meds available:
❝In terms of effectiveness, they all reduce your risk of broken bones by roughly the same amount.
Which treatment is right for you will depend on a number of things.❞
…before then going on to list a pageful of things it will depend on, and giving no specific information about what prescriptions or proscriptions may be made based on those factors.
Source: Royal Osteoporosis Society | Which medication should I take?
We’ll try to do better than that here, though we have less space. So let’s get down to it…
First line drug offerings
After diet/supplementation and (if applicable) hormones, the first line of actual drug offerings are generally biphosphates.
Biphosphates work by slowing down your osteoclasts—the cells that break down your bones. They may sound like terrible things to have in the body at all, but remember, your body is always rebuilding itself and destruction is a necessary act to facilitate creation. However, sometimes things can get out of balance, and biphosphates help tip things back into balance.
Common biphosphates include Alendronate/Fosamax, Risedronate/Actonel, Ibandronate/Boniva, and Zolendronic acid/Reclast.
A common downside is that they aren’t absorbed well by the stomach (despite being mostly oral administration, though IV versions exist too) and can cause heartburn / general stomach upset.
An uncommon downside is that messing with the body’s ability to break down bones can cause bones to be rebuilt-in-place slightly incorrectly, which can—paradoxically—cause fractures. But that’s rare and is more common if the drugs are taken in much higher doses (as for bone cancer rather than osteoporosis).
Bone-builders
If you already have low bone density (so you’re fighting to rebuild your bones, not just slow deterioration), then you may need more of a boost.
Bone-building medications include Teriparatide/Forteo, Abaloparatide/Tymlos, and Romosozumab/Evenity.
These are usually given by injection, usually for a course of one or two years.
Once the bone has been built up, it’ll probably be recommended that you switch to a biphosphate or other bone-stabilizing medication.
Estrogen-like effects, without estrogen
If your osteoporosis (or osteoporosis risk) comes from being post-menopausal, estrogen is a very common (and effective!) prescription. However, some people may wish to avoid it, if for example you have a heightened breast cancer risk, which estrogen can exacerbate.
So, medications that have estrogen-like effects post-menopause, but without actually increasing estrogen levels, include: Raloxifene/Evista, and also all the meds we mentioned in the bone-building category above.
Raloxifene/Evista specifically mimics the action of estrogen on bones, while at the same time blocking the effect of estrogen on other tissues.
Learn more…
Want a more thorough grounding than we have room for here? You might find the following resource useful:
List of 82 Osteoporosis Medications Compared (this has a big table which is sortable by various variables)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

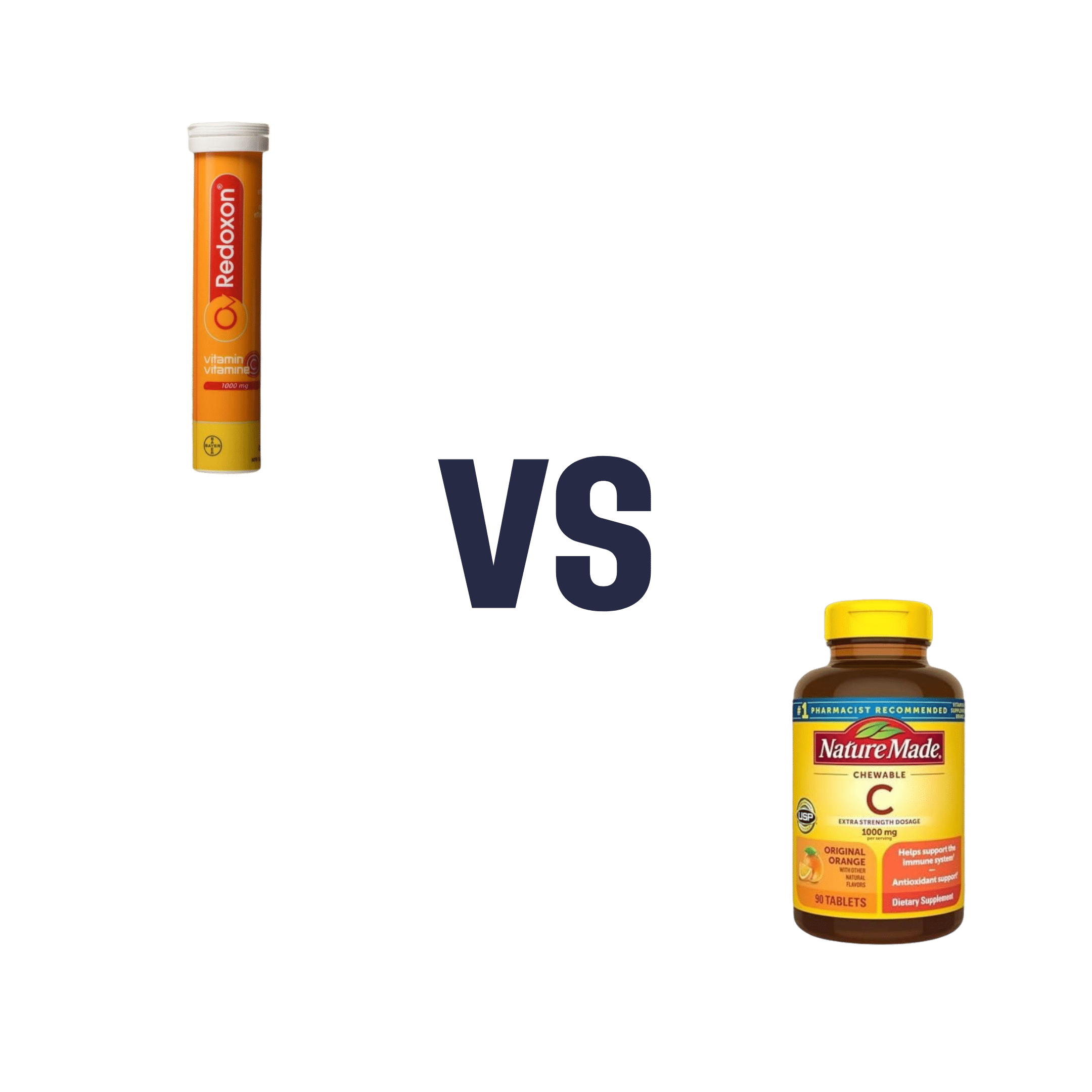
Vitamin C (Drinkable) vs Vitamin C (Chewable) – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing vitamin C (drinkable) to vitamin C (chewable), we picked the drinkable.
Why?
First let’s look at what’s more or less the same in each:
- The usable vitamin C content is comparable
- The bioavailability is comparable
- The additives to hold it together are comparable
So what’s the difference?
With the drinkable, you also drink a glass of water
If you’d like to read more about how to get the most out of the vitamins you take, you can do so here:
Are You Wasting Your Vitamins? Maybe, But You Don’t Have To
If you’d like to get some of the drinkable vitamin C, here’s an example product on Amazon
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Recognize The Early Symptoms Of Parkinson’s Disease
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Parkinson’s disease is a degenerative condition with wide-reaching implications for health. While there is currently no known cure, there are treatments, so knowing about it sooner rather than later is important.
Spot The Signs
There are two main kinds of symptoms, motor and non-motor.
Motor symptoms include:
- trembling that occurs when muscles are relaxed; often especially visible in the fingers
- handwriting changes—not just because of the above, but also often getting smaller
- blank expression, on account of fewer instruction signals getting through to the face
- frozen gait—especially difficulty starting walking, and a reduced arm swing
Non-motor symptoms include:
- loss of sense of smell—complete, or a persistent reduction of
- sleepwalking, or sleep-talking, or generally acting out dreams while asleep
- constipation—on an ongoing basis
- depression/anxiety, especially if there was no prior history of these conditions
For more detail on each of these, as well as what steps you might want to take, check out what Dr. Luis Zayas has to say:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Citicoline vs Parkinson’s (And More)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: