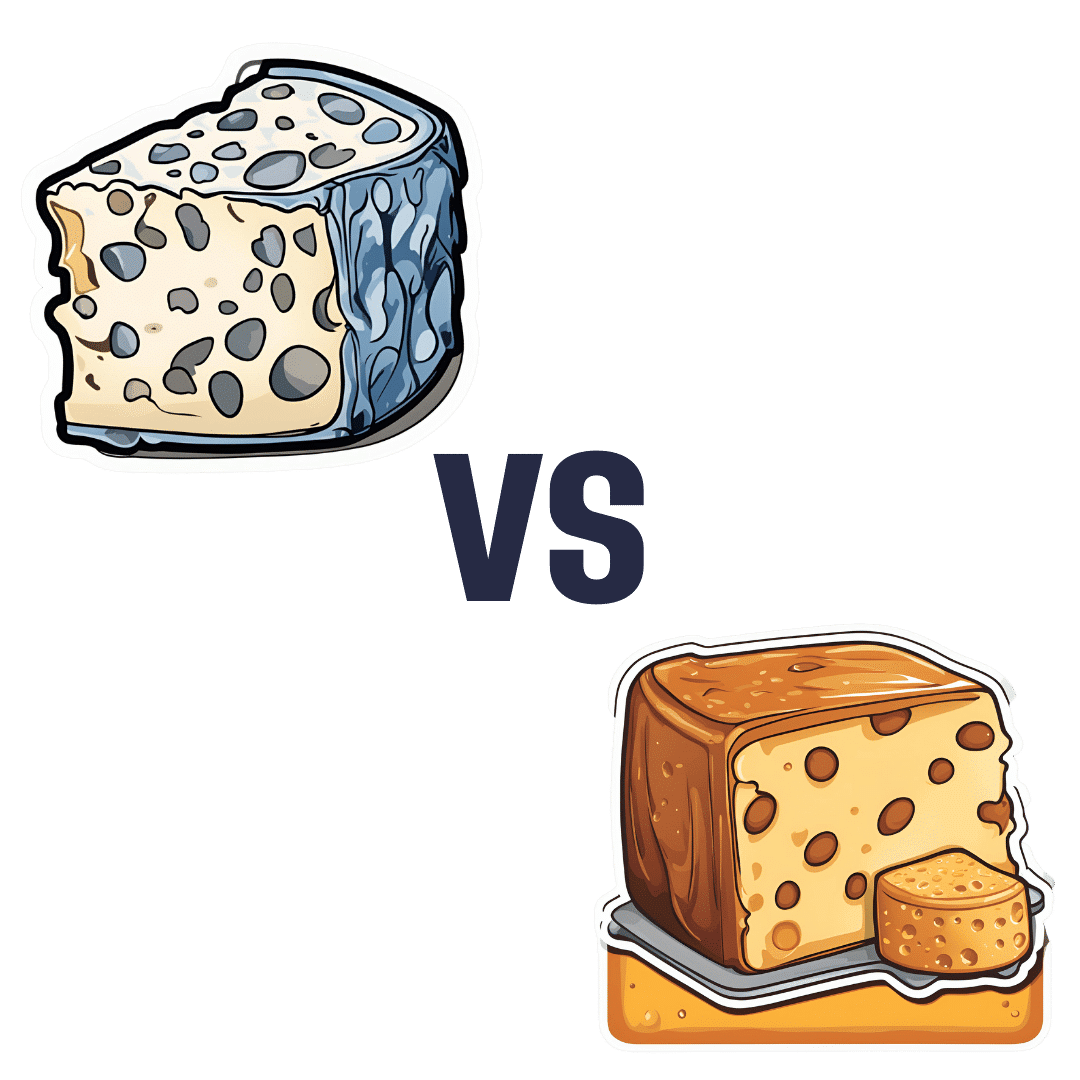
Blue Cheese vs Brunost – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing blue cheese to brunost, we picked the brunost.
Why?
First, for the unfamiliar, as brunost isn’t necessarily as popular as blue cheese in N. America where most of our readers are:
Brunost, literally “brown cheese” is a traditional Norwegian affair made from aggressively boiling milk, cream, and whey in an iron cauldron. Whereas the blue in blue cheese comes from mold, the brown in brown cheese comes from caramelizing the milk sugars in the cauldron. When we say “cauldron”, yes, there is nowadays mass-produced brunost that is no longer made in something that could be mistaken for a witch’s brew, but the use of cast iron is actually important to the process, and has been the subject of regulatory controversy in Norway; first the cast iron was abandoned, then because that changed the cheese they fortified the product with added iron supplementation, then that was banned, then they reversed it because it affected iron levels in the general population. Nowadays, it is usually made with iron, one way or another.
Ok, so let’s see how they stack up against each other:
In terms of macronutrients, the two cheeses are comparable in fat, but brunost has more carbs—because whereas bacteria (and to a lesser extent, the mold) ate nearly all the carbs in the blue cheese, the caramelization of the milk sugars in brunost meant the result stayed higher in carbs. Both are considered “low GI” foods, but this category is still at least a moderate win for blue cheese.
When it comes to vitamins, brunost is higher in vitamins A, B1, B2, B3, B5, B6, and B12, while blue cheese is higher in vitamin B9. In other words, a clear and easy win for brunost.
In the category of minerals, brunost has more copper, iron, magnesium, manganese, phosphorus, and potassium. Meanwhile, blue cheese contains more zinc, although we can also mention that blue cheese has about 2x the sodium, which is generally not considered a benefit. The two cheeses are about equal in calcium and selenium. Adding these up makes for another clear and easy win for brunost.
In short, unless you are strongly avoiding [even low-GI foods’] carbs for some reason, brunost wins the day by virtue of its overwhelmingly better vitamin and mineral content.
Still, like most fermented dairy products, both cheeses can be enjoyed in moderation as part of a healthy diet (assuming you don’t have an allergy/intolerance).
Want to learn more?
You might like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Walking… Better.

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Walking… Better.
We recently reviewed “52 Ways To Walk” by Annabel Streets. You asked us to share some more of our learnings from that book, and… Obviously we can’t do all 52, nor go into such detail, but here are three top tips inspired by that book…
Walk in the cold!
While cold weather is often seen as a reason to not walk, in fact, it has numerous health benefits, the most exciting of which might be:
Walking in the cold causes us to convert white and yellow fat into the healthier brown fat. If you didn’t know about this, neither did scientists until about 15 years ago.
In fact, scientists didn’t even know that adult humans could even have brown adipose tissue! It was really quite groundbreaking.
In case you missed it: The Changed Metabolic World with Human Brown Adipose Tissue: Therapeutic Visions
Work while you walk!
Obviously this is only appropriate for some kinds of work… but if in your life you have any kind of work that is chiefly thinking, a bunch of it can be done while walking.
Open your phone’s note-taking app, lock the screen and pocket your phone, and think on some problem that you need to solve. Whenever you have an “aha” moment, take out your phone and make a quick note on the go.
For that matter, if you have the money and space (or are fortunate to have an employer disposed towards facilitating such), you could even set up a treadmill desk… At worst, it wouldn’t harm your work (and it’ll be a LOT better than sitting for so long).
Walk within an hour of waking!
No, this doesn’t mean that if you don’t get out of the house within 60 minutes you say “Oh no, missed the window, guess it’s a day in today”
But it does mean: in the evening, make preparations to head out first thing in the morning. Set out your clothes and appropriate footwear, find your flask to fill with the beverage of your choice in the morning and set that with them.
Then, when morning arrives… do your morning necessaries (e.g. some manner of morning ablutions and perhaps a light breakfast), make that drink for your flask, and hit the road.
Why? We’ll tell you a secret:
You ever wondered why some people seem to be more able to keep a daylight-regulated circadian rhythm than others? It’s not just about smartphones and coffees…
This study found that getting sunlight (not electric light, not artificial sunlight, but actual sunlight, from the sun, even if filtered through partial cloud) between 08:30—09:00 resulted in higher levels of a protein called PER2. PER2 is critical for setting circadian rhythms, improving metabolism, and fortifying blood vessels.
Besides, on a more simplistic level, it’s also a wonderful and energizing start to a healthy and productive day!
Read: Beneficial effects of daytime light exposure on daily rhythms, metabolic state and affect
Share This Post
-

Real Superfoods – by Ocean Robbins & Nichole Dandrea-Russert
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Of the two authors, the former is a professional public speaker, and the latter is a professional dietician. As a result, we get a book that is polished and well-presented, while actually having a core of good solid science (backed up with plenty of references).
The book is divided into two parts; the first part has 9 chapters pertaining to 9 categories of superfood (with more details about top-tier examples of each, within), and the second part has 143 pages of recipes.
And yes, as usual, a couple of the recipes are “granola” and “smoothie”, but when are they not? Most of the recipes are worthwhile, though, with a lot of good dishes that should please most people.
Bottom line: this is half pop-science presentation of superfoods, and half cookbook featuring those ingredients. Definitely a good way to increase your consumption of superfoods, and get the most out of your diet.
Click here to check out Real Superfoods, and power up your health!
Share This Post
-

Water Fluoridation, Atheroma, & More
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝I watched a documentary recently on Fluoride in our drinking water & the dangers of it. Why are we poisoning our water?❞
This is a great question, and it certainly is controversial. It sounds like the documentary you watched was predominantly or entirely negative, but there’s a lot of science to back both sides of this, and it’s not even that the science is contradictory (it’s not). It’s that what differs is people’s opinions about whether benefiting one thing is worth creating a risk to another, and that means looking at:
- What is the risk associated with taking no action (error of omission)?
- What is the risk associated with taking an action (error of commission)?
The whole topic is worth a main feature, but to summarize a few key points:
- Water fluoridation is considered good for the prevention of dental cavities
- Water fluoridation aims to deliver fluoride and doses far below dangerous levels
- This requires working on consumer averages, though
- ”Where do we put the safety margins?” is to some extent a subjective question, in terms of trading off one aspect of health for another
- Too much fluoride can also be bad for the teeth (at least cosmetically, creating little white* spots)
- Detractors of fluoride tend to mostly be worried about neurological harm
- However, the doses in public water supplies are almost certainly far below the levels required to cause this harm.
- That said, again this is working on consumer averages, though.
- However, the doses in public water supplies are almost certainly far below the levels required to cause this harm.
- A good guide is: watch your teeth! Those white* spots will be “the canary in the coal mine” of more serious harm that could potentially come from higher levels due to overconsumption of fluorine.
*Teeth are not supposed to be pure white. The “Hollywood smile” is a lie. Teeth are supposed to be a slightly off-white, ivory color. Anything whiter than that is adding something else that shouldn’t be there, or stripping something off that should be there.
❝How does your diet change clean out your arteries of the bad cholesterol?❞
There’s good news and bad news here, and they can both be delivered with a one-word reply:
Slowly.
Or rather: what’s being cleaned out is mostly not the LDL (bad) cholesterol, but rather, the result of that.
When our diet is bad for cardiovascular health, our arteries get fatty deposits on their walls. Cholesterol gets stuck here too, but that’s not the main physical problem.
Our body’s natural defenses come into action and try to clean it up, but they (for example macrophages, a kind of white blood cell that consumes invaders and then dies, before being recycled by the next part of the system) often get stuck and become part of the buildup (called atheroma), which can lead to atherosclerosis and (if calcium levels are high) hardening of the arteries, which is the worst end of this.
This can then require medical attention, precisely because the body can’t remove it very well—especially if you are still maintaining a heart-unhealthy diet, thus continuing to add to the mess.
However, if it is not too bad yet, yes, a dietary change alone will reverse this process. Without new material being added to the arterial walls, the body’s continual process of rejuvenation will eventually fix it, given time (free from things making it worse) and resources.
In fact, your arteries can be one of the quickest places for your body to make something better or worse, because the blood is the means by which the body moves most things (good or bad) around the body.
All the more reason to take extra care of it, since everything else depends on it!
You might also like our previous main feature:
Share This Post


Related Posts
-

Outsmart Your Pain – by Dr. Christiane Wolf
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Wolf is a physician turned mindfulness teacher. As such, and holding an MD as well as a PhD in psychosomatic medicine, she knows her stuff.
A lot of what she teaches is mindfulness-based stress reduction (MBSR), but this book is much more specific than that. It doesn’t promise you won’t continue to experience pain—in all likelihood you will—but it does change the relationship with pain, and this greatly lessens the suffering and misery that comes with it.
For many, the most distressing thing about pain is not the sensation itself, but how crippling it can be—getting in the way of life, preventing enjoyment of other things, and making every day a constant ongoing exhausting battle… And every night, a “how much rest am I actually going to be able to get, and in what condition will I wake up, and how will I get through tomorrow?” stress-fest.
Dr. Wolf helps the reader to navigate through all these challenges and more; minimize the stress, maximize the moments of respite, and keep pain’s interference with life to a minimum. Each chapter addresses different psychological aspects of chronic pain management, and each comes with specific mindfulness meditations to explore the new ideas learned.
The style is personal and profound, while coming from a place of deep professional understanding as well as compassion.
Bottom line: if you’ve been looking for a life-ring to help you reclaim your life, this one could be it; we wholeheartedly recommend it.
Click here to check out Outsmart Your Pain, and recover the beauty and joy of life!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Knowledge That Harvard Medical School’s Clinical Instructor Dr. Monique Tello Thinks Everyone SHOULD Have About Heart Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Anyone (who has not had a double mastectomy, anyway) can get breast cancer.
Breast cancer, if diagnosed early (before it spreads), has a 98% survival rate.
That survival rate drops to 31% if diagnosed after it has spread through the body.
(The US CDC’s breast cancer “stat bite” page has more stats and interactive graphs, so click here to see those charts and get the more detailed low-down on mortality/survival rates with various different situations)
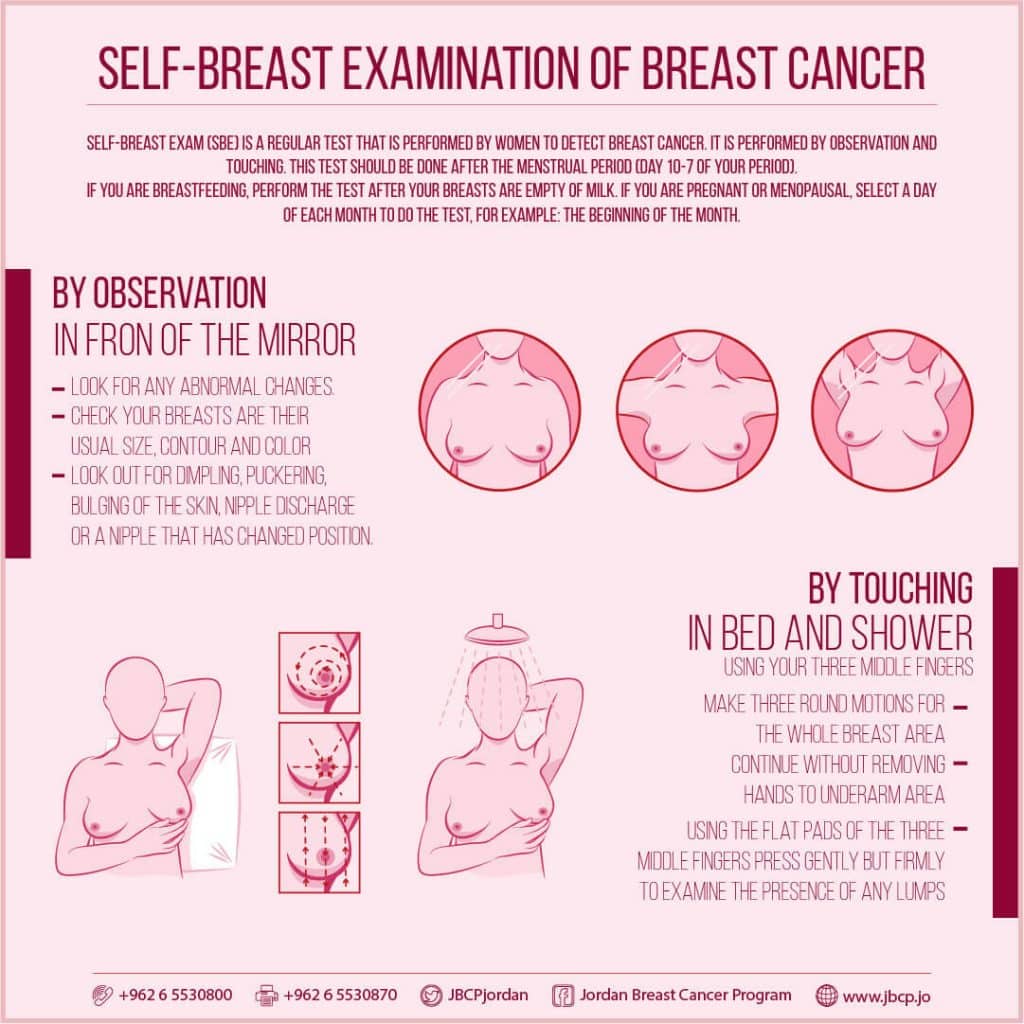
We think that the difference between 98% and 31% survival rates is more than enough reason to give ourselves a monthly self-check at the very least! You’ve probably seen how-to diagrams before, but here are instructions for your convenience:
This graphic created by the Jordan Breast Cancer Program (check them out, as they have lots of resources)

If you don’t have the opportunity to take matters into your own hands right now, rather than just promise yourself “I’ll do that later”, take this free 4-minute Breast Health Assessment from Aurora Healthcare. Again, we think the difference early diagnosis can make to your survival chances make these tests well worth it.
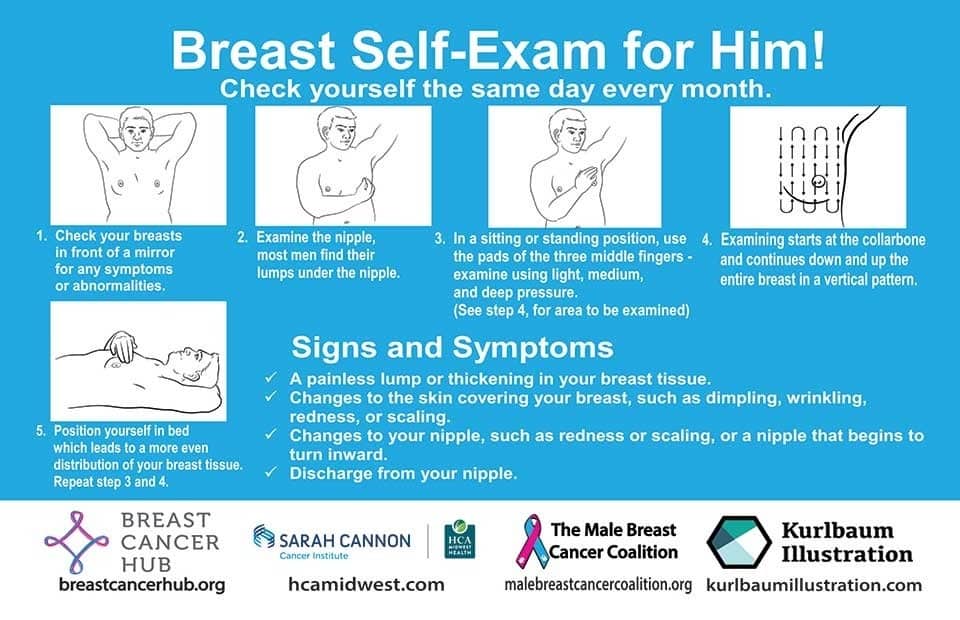
Lest we forget, men can also get breast cancer (the CDC has a page for men too), especially if over 50. But how do you check for breast cancer, when you don’t have breasts in the commonly-understood sense of the word?

So take a moment to do this (yes, really actually do it!), and set a reminder in your calendar to repeat it monthly—there really is no reason not to! Take care of yourself; you’re important.
Pssst! Did you scroll past the diagrams, looking for the online 4-minute test promised by the subtitle? If so, scroll back up; the link is in the middle!
Harvard Medical School’s Clinical Instructor’s Five-Point Plan for Heart Health
Dr. Monique Tello, M.D., M.P.H., is a practicing physician at Massachusetts General Hospital, director of research and academic affairs for the MGH DGM Healthy Lifestyle Program, clinical instructor at Harvard Medical School, and author of the evidence-based lifestyle change guide Healthy Habits for Your Heart.

Here are what she says are the five most important factors to help keep your ticker ticking:
5. Have (at most) a moderate alcohol intake! While there are polyphenols such as resveratrol in red wine that could boost heart health, there’s so little per glass that you may need 100–1000 glasses to get the dosage that provides benefits in mouse studies. If you’re not a mouse, it may not be as beneficial, and Dr. Tello recommends drinking no more than one glass per day of any alcohol. What constitutes a glass? It varies from one kind of drink to another, so here’s a handy guide.
4. Don’t smoke. Best of all to never start. But if you did, quit. Simple as that. There is no healthy amount of smoking. While paradoxically, quitting smoking may of course be stressful to you, the long term gains are considered more than worth it. As with all advice, do consult your own physician for guidance, as individual circumstances may vary, and that may change the best approach for you.
3. Maintain a healthy body weight. While BMI (Body Mass Index) is not a perfect system, it’s a system in popular use, and Dr. Tello recommends keeping a BMI between 18.5 and 24.9.
What’s your BMI? It takes into account your height and weight; here’s a Quick BMI Calculator for your convenience.
2. Keep a healthy level of physical activity—which ideally means at least 30 minutes per day vigorous activity, but obviously if you’re not used to this, take it slowly and build up over time. Even just small lifestyle changes (walking where possible, taking the stairs instead of the elevator where possible, etc) can add up to a big difference.
1. Enjoy a healthy diet. This is the single most important thing, and the best modern scientific consensus holds that the best diet contains plenty of vegetables, fruits and nuts, whole grains, and omega-3 fatty acids, while it avoids processed meats, sugar-sweetened beverages, trans fats (what are trans fats?), and too much sodium.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What’s the difference between shyness and social anxiety?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
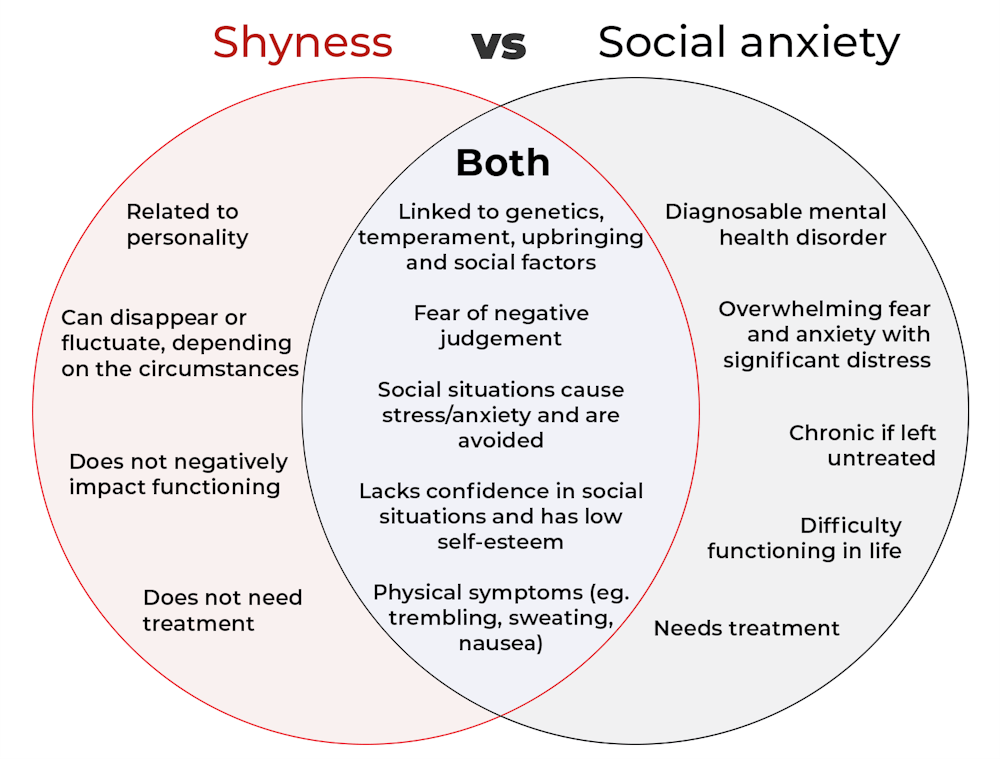
The terms “shyness” and “social anxiety” are often used interchangeably because they both involve feeling uncomfortable in social situations.
However, feeling shy, or having a shy personality, is not the same as experiencing social anxiety (short for “social anxiety disorder”).
Here are some of the similarities and differences, and what the distinction means.

pathdoc/Shutterstock How are they similar?
It can be normal to feel nervous or even stressed in new social situations or when interacting with new people. And everyone differs in how comfortable they feel when interacting with others.
For people who are shy or socially anxious, social situations can be very uncomfortable, stressful or even threatening. There can be a strong desire to avoid these situations.
People who are shy or socially anxious may respond with “flight” (by withdrawing from the situation or avoiding it entirely), “freeze” (by detaching themselves or feeling disconnected from their body), or “fawn” (by trying to appease or placate others).
A complex interaction of biological and environmental factors is also thought to influence the development of shyness and social anxiety.
For example, both shy children and adults with social anxiety have neural circuits that respond strongly to stressful social situations, such as being excluded or left out.
People who are shy or socially anxious commonly report physical symptoms of stress in certain situations, or even when anticipating them. These include sweating, blushing, trembling, an increased heart rate or hyperventilation.
How are they different?
Social anxiety is a diagnosable mental health condition and is an example of an anxiety disorder.
For people who struggle with social anxiety, social situations – including social interactions, being observed and performing in front of others – trigger intense fear or anxiety about being judged, criticised or rejected.
To be diagnosed with social anxiety disorder, social anxiety needs to be persistent (lasting more than six months) and have a significant negative impact on important areas of life such as work, school, relationships, and identity or sense of self.
Many adults with social anxiety report feeling shy, timid and lacking in confidence when they were a child. However, not all shy children go on to develop social anxiety. Also, feeling shy does not necessarily mean a person meets the criteria for social anxiety disorder.
People vary in how shy or outgoing they are, depending on where they are, who they are with and how comfortable they feel in the situation. This is particularly true for children, who sometimes appear reserved and shy with strangers and peers, and outgoing with known and trusted adults.
Individual differences in temperament, personality traits, early childhood experiences, family upbringing and environment, and parenting style, can also influence the extent to which people feel shy across social situations.
Not all shy children go on to develop social anxiety. 249 Anurak/Shutterstock However, people with social anxiety have overwhelming fears about embarrassing themselves or being negatively judged by others; they experience these fears consistently and across multiple social situations.
The intensity of this fear or anxiety often leads people to avoid situations. If avoiding a situation is not possible, they may engage in safety behaviours, such as looking at their phone, wearing sunglasses or rehearsing conversation topics.
The effect social anxiety can have on a person’s life can be far-reaching. It may include low self-esteem, breakdown of friendships or romantic relationships, difficulties pursuing and progressing in a career, and dropping out of study.
The impact this has on a person’s ability to lead a meaningful and fulfilling life, and the distress this causes, differentiates social anxiety from shyness.
Children can show similar signs or symptoms of social anxiety to adults. But they may also feel upset and teary, irritable, have temper tantrums, cling to their parents, or refuse to speak in certain situations.
If left untreated, social anxiety can set children and young people up for a future of missed opportunities, so early intervention is key. With professional and parental support, patience and guidance, children can be taught strategies to overcome social anxiety.
Why does the distinction matter?
Social anxiety disorder is a mental health condition that persists for people who do not receive adequate support or treatment.
Without treatment, it can lead to difficulties in education and at work, and in developing meaningful relationships.
Receiving a diagnosis of social anxiety disorder can be validating for some people as it recognises the level of distress and that its impact is more intense than shyness.
A diagnosis can also be an important first step in accessing appropriate, evidence-based treatment.
Different people have different support needs. However, clinical practice guidelines recommend cognitive-behavioural therapy (a kind of psychological therapy that teaches people practical coping skills). This is often used with exposure therapy (a kind of psychological therapy that helps people face their fears by breaking them down into a series of step-by-step activities). This combination is effective in-person, online and in brief treatments.
Treatment is available online as well as in-person. ImYanis/Shutterstock For more support or further reading
Online resources about social anxiety include:
- This Way Up’s online program for managing excessive shyness and fear of social situations
- Beyond Blue’s resources on social anxiety
- a guide to looking after yourself if you have social anxiety, from the Western Australian health department
- social anxiety online program for children and teens from the University of Queensland
- inroads, a self-guided online program for young adults who drink alcohol to manage their anxiety.
We thank the Black Dog Institute Lived Experience Advisory Network members for providing feedback and input for this article and our research.
Kayla Steele, Postdoctoral research fellow and clinical psychologist, UNSW Sydney and Jill Newby, Professor, NHMRC Emerging Leader & Clinical Psychologist, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: