A new emergency procedure for cardiac arrests aims to save more lives – here’s how it works
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
As of January this year, Aotearoa New Zealand became just the second country (after Canada) to adopt a groundbreaking new procedure for patients experiencing cardiac arrest.
Known as “double sequential external defibrillation” (DSED), it will change initial emergency response strategies and potentially improve survival rates for some patients.
Surviving cardiac arrest hinges crucially on effective resuscitation. When the heart is working normally, electrical pulses travel through its muscular walls creating regular, co-ordinated contractions.
But if normal electrical rhythms are disrupted, heartbeats can become unco-ordinated and ineffective, or cease entirely, leading to cardiac arrest.
Defibrillation is a cornerstone resuscitation method. It gives the heart a powerful electric shock to terminate the abnormal electrical activity. This allows the heart to re-establish its regular rhythm.
Its success hinges on the underlying dysfunctional heart rhythm and the proper positioning of the defibrillation pads that deliver the shock. The new procedure will provide a second option when standard positioning is not effective.
Using two defibrillators
During standard defibrillation, one pad is placed on the right side of the chest just below the collarbone. A second pad is placed below the left armpit. Shocks are given every two minutes.
Early defibrillation can dramatically improve the likelihood of surviving a cardiac arrest. However, around 20% of patients whose cardiac arrest is caused by “ventricular fibrillation” or “pulseless ventricular tachycardia” do not respond to the standard defibrillation approach. Both conditions are characterised by abnormal activity in the heart ventricles.
DSED is a novel method that provides rapid sequential shocks to the heart using two defibrillators. The pads are attached in two different locations: one on the front and side of the chest, the other on the front and back.
A single operator activates the defibrillators in sequence, with one hand moving from the first to the second. According to a recent randomised trial in Canada, this approach could more than double the chances of survival for patients with ventricular fibrillation or pulseless ventricular tachycardia who are not responding to standard shocks.
The second shock is thought to improve the chances of eliminating persistent abnormal electrical activity. It delivers more total energy to the heart, travelling along a different pathway closer to the heart’s left ventricle.
Evidence of success
New Zealand ambulance data from 2020 to 2023 identified about 1,390 people who could potentially benefit from novel defibrillation methods. This group has a current survival rate of only 14%.
Recognising the potential for DSED to dramatically improve survival for these patients, the National Ambulance Sector Clinical Working Group updated the clinical procedures and guidelines for emergency medical services personnel.
The guidelines now specify that if ventricular fibrillation or pulseless ventricular tachycardia persist after two shocks with standard defibrillation, the DSED method should be administered. Two defibrillators need to be available, and staff must be trained in the new approach.
Though the existing evidence for DSED is compelling, until recently it was based on theory and a small number of potentially biased observational studies. The Canadian trial was the first to directly compare DSED to standard treatment.
From a total of 261 patients, 30.4% treated with this strategy survived, compared to 13.3% when standard resuscitation protocols were followed.
The design of the trial minimised the risk of other factors confounding results. It provides confidence that survival improvements were due to the defibrillation approach and not regional differences in resources and training.
The study also corroborates and builds on existing theoretical and clinical scientific evidence. As the trial was stopped early due to the COVID-19 pandemic, however, the researchers could recruit fewer than half of the numbers planned for the study.
Despite these and other limitations, the international group of experts that advises on best practice for resuscitation updated its recommendations in 2023 in response to the trial results. It suggested (with caution) that emergency medical services consider DSED for patients with ventricular fibrillation or pulseless ventricular tachycardia who are not responding to standard treatment.
Training and implementation
Although the evidence is still emerging, implementation of DSED by emergency services in New Zealand has implications beyond the care of patients nationally. It is also a key step in advancing knowledge about optimal resuscitation strategies globally.
There are always concerns when translating an intervention from a controlled research environment to the relative disorder of the real world. But the balance of evidence was carefully considered before making the decision to change procedures for a group of patients who have a low likelihood of survival with current treatment.
Before using DSED, emergency medical personnel undergo mandatory education, simulation and training. Implementation is closely monitored to determine its impact.
Hospitals and emergency departments have been informed of the protocol changes and been given opportunities to ask questions and give feedback. As part of the implementation, the St John ambulance service will perform case reviews in addition to wider monitoring to ensure patient safety is prioritised.
Ultimately, those involved are optimistic this change to cardiac arrest management in New Zealand will have a positive impact on survival for affected patients.![]()
Vinuli Withanarachchie, PhD candidate, College of Health, Massey University; Bridget Dicker, Associate Professor of Paramedicine, Auckland University of Technology, and Sarah Maessen, Research Associate, Auckland University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Soap vs Sanitizer – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing soap to sanitizer, we picked the soap.
Why?
Both are good at killing bacteria / inactivating viruses, but there are several things that set them apart:
- Soap doesn’t just kill them; it slides them off and away down the drain. That means that any it failed to kill are also off and down the drain, not still on your hands. This is assuming good handwashing technique, of course!
- Sanitizer gel kills them, but can take up to 4 minutes of contact to do so. Given that people find 20 seconds of handwashing laborious, 240 seconds of sanitizer gel use seems too much to hope for.
Both can be dehydrating for the hands; both can have ingredients added to try to mitigate that.
We recommend a good (separate) moisturizer in either case, but the point is, the dehydration factor doesn’t swing it far either way.
So, we’ll go with the one that gets rid of the germs the most quickly: the soap
10almonds tip: splash out on the extra-nice hand-soaps for your home—this will make you and others more likely to wash your hands more often! Sometimes, making something a more pleasant experience makes all the difference.
Want to know more?
Check out:
Take care!
Share This Post
-

The Best Mobility Exercises For Each Joint
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Stiff joints and tight muscles limit movement, performance, and daily activities. They also increase the risk of injury, and increase recovery time if the injury happens. So, it’s pretty important to take care of that!
Here’s how
Key to joint health involves understanding mobility, flexibility, and stability:
- Mobility: active joint movement through a range of motion.
- Flexibility: muscle lengthening passively through a range of motion.
- Stability: body’s ability to return to position after disturbance.
Different body parts have different needs when it comes to prioritizing mobility, flexibility, and stability exercises. So, with that in mind, here’s what to do for your…
- Wrists: flexibility and stability (e.g., wrist circles, loaded flexions/extensions).
- Elbows: Stability is key; exercises like wrist and shoulder movements benefit elbows indirectly.
- Shoulders: mobility and stability; exercises include prone arm circles, passive hangs, active prone raises, easy bridges, and stick-supported movements.
- Spine: mobility and stability; recommended exercises include cat-cow and quadruped reach.
- Hips: mobility and flexibility through deep squat hip rotations; beginners can use hands for support.
- Knees: stability; exercises include elevated pistols, Bulgarian split squats, lunges, and single-leg balancing.
- Ankles: flexibility and stability; exercises include lunges, prying goblet squats, and deep squats with support if necessary.
For more on all of these, plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Building & Maintaining Mobility
Take care!
Share This Post
-

Should You Go Light Or Heavy On Carbs?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Carb-Strong or Carb-Wrong?

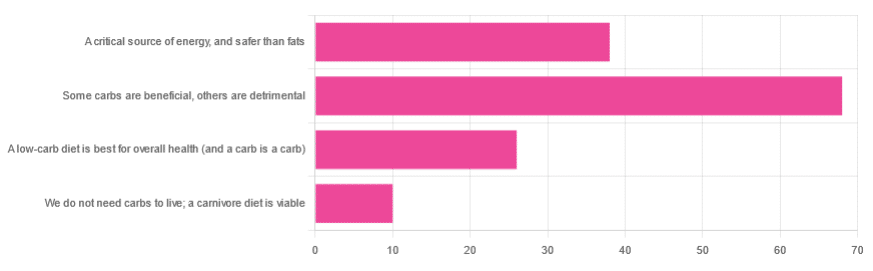
We asked you for your health-related view of carbs, and got the above-depicted, below-described, set of responses
- About 48% said “Some carbs are beneficial; others are detrimental”
- About 27% said “Carbs are a critical source of energy, and safer than fats”
- About 18% said “A low-carb diet is best for overall health (and a carb is a carb)”
- About 7% said “We do not need carbs to live; a carnivore diet is viable”
But what does the science say?
Carbs are a critical source of energy, and safer than fats: True or False?
True and False, respectively! That is: they are a critical source of energy, and carbs and fats both have an important place in our diet.
❝Diets that focus too heavily on a single macronutrient, whether extreme protein, carbohydrate, or fat intake, may adversely impact health.❞
Source: Low carb or high carb? Everything in moderation … until further notice
(the aforementioned lead author Dr. de Souza, by the way, served as an external advisor to the World Health Organization’s Nutrition Guidelines Advisory Committee)
Some carbs are beneficial; others are detrimental: True or False?
True! Glycemic index is important here. There’s a big difference between eating a raw carrot and drinking high-fructose corn syrup:
Which Sugars Are Healthier, And Which Are Just The Same?
While some say grains and/or starchy vegetables are bad, best current science recommends:
- Eat some whole grains regularly, but they should not be the main bulk of your meal (non-wheat grains are generally better)
- Starchy vegetables are not a critical food group, but in moderation they are fine.
To this end, the Mediterranean Diet is the current gold standard of healthful eating, per general scientific consensus:
A low-carb diet is best for overall health (and a carb is a carb): True or False?
True-ish and False, respectively. We covered the “a carb is a carb” falsehood earlier, so we’ll look at “a low-carb diet is best”.
Simply put: it can be. One of the biggest problems facing the low-carb diet though is that adherence tends to be poor—that is to say, people crave their carby comfort foods and eat more carbs again. As for the efficacy of a low-carb diet in the context of goals such as weight loss and glycemic control, the evidence is mixed:
❝There is probably little to no difference in weight reduction and changes in cardiovascular risk factors up to two years’ follow-up, when overweight and obese participants without and with T2DM are randomised to either low-carbohydrate or balanced-carbohydrate weight-reducing diets❞
Source: Low-carbohydrate versus balanced-carbohydrate diets for reducing weight and cardiovascular risk
❝On the basis of moderate to low certainty evidence, patients adhering to an LCD for six months may experience remission of diabetes without adverse consequences.
Limitations include continued debate around what constitutes remission of diabetes, as well as the efficacy, safety, and dietary satisfaction of longer term LCDs❞
~ Dr. Joshua Goldenberg et al.
Source: Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission
❝There should be no “one-size-fits-all” eating pattern for different patient´s profiles with diabetes.
It is clinically complex to suggest an ideal percentage of calories from carbohydrates, protein and lipids recommended for all patients with diabetes.❞
Source: Current Evidence Regarding Low-carb Diets for The Metabolic Control of Type-2 Diabetes
We do not need carbs to live; a carnivore diet is viable: True or False?
False. For a simple explanation:
The Carnivore Diet: Can You Have Too Much Meat?
There isn’t a lot of science studying the effects of consuming no plant products, largely because such a study, if anything other than observational population studies, would be unethical. Observational population studies, meanwhile, are not practical because there are so few people who try this, and those who do, do not persist after their first few hospitalizations.
Putting aside the “Carnivore Diet” as a dangerous unscientific fad, if you are inclined to meat-eating, there is some merit to the Paleo Diet, at least for short-term weight loss even if not necessarily long-term health:
What’s The Real Deal With The Paleo Diet?
For longer-term health, we refer you back up to the aforementioned Mediterranean Diet.
Enjoy!
Share This Post

-
Pine Nuts vs Macadamia Nuts – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing pine nuts to macadamias, we picked the pine nuts.
Why?
In terms of macros, it’s subjective depending on what you want to prioritize; the two nuts are equal in carbs, but pine nuts have more protein and macadamias have more fiber. We’d generally prioritize the fiber, which so far would give macadamias a win in this category, but if you prefer the protein, then consider it pine nuts. Next, we must consider fats; macadamias have slightly more fat, and of which, proportionally more saturated fat, resulting in 3x the total saturated fat compared to pine nuts, gram for gram. With this in mind, we consider this category a tie or a marginal nominal win for pine nuts.
In the category of vitamins, pine nuts have more of vitamins A, B2, B3, B9, E, K, and choline, while macadamias have more of vitamins B1, B5, B6, and C. A clear win for pine nuts this time, especially with pine nuts having more than 17x the vitamin E of macadamias.
When it comes to minerals, pine nuts have more copper, iron, magnesium, manganese, phosphorus, potassium, and zinc, while macadamias have more calcium and selenium. Another easy win for pine nuts.
In short, enjoy either or both (diversity is good), but pine nuts are the healthier by most metrics.
Want to learn more?
You might like to read:
Why You Should Diversify Your Nuts
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Once-A-Week Strategy to Stop Procrastination – by Brad Meir
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Procrastination is perhaps the most frustrating bad habit to kick!
We know we should do the things. We know why we should do the things. We want to do the things. We’re afraid of what will happen if we don’t do the things. And then we… don’t do the things? What is going on?!
Brad Meir has answers, and—what a relief—solutions. But enough about him, because first he wants to focus a little on you:
Why do you procrastinate? No, you’re probably not “just lazy”, and he’ll guide you through figuring out what it is that makes you procrastinate. There’s an exploration of various emotions here, as well as working out: what type of procrastinator are you?
Then, per what you figured out with his guidance, exercises, and tests, it’s time for an action plan.
But, importantly: one you can actually do, because it won’t fall foul of the problems you’ve been encountering so far. The exact mechanism you’ll use may vary a bit based on you, but some tools here are good for everyone—as well as an outline of the mistakes you could easily make, and how to avoid falling into those traps. And, last but very definitely not least, his “once a week plan”, per the title.
All in all, a highly recommendable and potentially life-changing book.
Grab Your Copy of “Once-A-Week Strategy to Stop Procrastination” NOW (don’t put it off!)
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Xylitol vs Erythritol – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing xylitol to erythritol, we picked the xylitol.
Why?
They’re both sugar alcohols, which so far as the body is concerned are neither sugars nor alcohols in the way those words are commonly understood; it’s just a chemical term. The sugars aren’t processed as such by the body and are passed as dietary fiber, and nor is there any intoxicating effect as one might expect from an alcohol.
In terms of macronutrients, while technically they both have carbs, for all functional purposes they don’t and just have a little fiber.
In terms of micronutrients, they don’t have any.
The one thing that sets them apart is their respective safety profiles. Xylitol is prothrombotic and associated with major adverse cardiac events (CI=95, adjusted hazard ratio=1.57, range=1.12-2.21), while erythritol is also prothrombotic and more strongly associated with major adverse cardiac events (CI=95, adjusted hazard ratio=2.21, range=1.20-4.07).
So, xylitol is bad and erythritol is worse, which means the relatively “healthier” is xylitol. We don’t recommend either, though.
Studies for both:
- Xylitol is prothrombotic and associated with cardiovascular risk
- The artificial sweetener erythritol and cardiovascular event risk
Links for the specific products we compared, in case our assessment hasn’t put you off them:
Want to learn more?
You might like to read:
- The WHO’s New View On Sugar-Free Sweeteners ← the WHO’s advice is “don’t”
- Stevia vs Acesulfame Potassium – Which is Healthier? ← stevia’s pretty much the healthiest artificial sweetener around, though, if you’re going to use one
- The Fascinating Truth About Aspartame, Cancer, & Neurotoxicity ← under the cold light of science, aspartame isn’t actually as bad as it was painted a few decades ago, mostly by a viral hoax letter. Per the WHO’s advice, it’s still good to avoid sweeteners in general, however.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: