Quit Like a Woman – by Holly Whitaker
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve reviewed “quit drinking” books before, so what makes this one different?
While others focus on the science of addiction and the tips and tricks of habit breaking/forming, this one is more about environmental factors, and that because of society being as it is, we as women often face different challenges when it comes to drinking (or not). Not necessarily easier or harder than men’s in this case, but different. And that sometimes calls for different methods to deal with them. This book explores those.
She also looks at such matters as how to quit alcohol when you’ve never stuck to a diet, and other such very down-to-earth topics, in a well-researched and non-preachy fashion.
Bottom line: if you’ve sometimes tried to quit drinking or even just to cut back, but found the deck stacked against you and things conspire to undermine your efforts, this book will give you a clearer path forward.
Click here to check out Quite Like A Woman, And Take Care Of Yourself!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Twice-Baked Stuffed Potatoes

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Packed with protein and fiber and dosed with healthy spices, these tasty treats can be enjoyed hot as they are, or cold as part of a salad dinner.
You will need
- 4 large baking potatoes
- 2 cans chickpeas, drained
- 1 can coconut milk
- ½ cup shredded mozzarella cheese, or plant-based alternative
- 1 bulb garlic (sounds like a lot, but this is about three cloves per potato; adjust if you want, though)
- 3 tbsp chopped pickled jalapeños
- 1 tbsp black pepper
- 2 tsp ground cumin
- 2 tsp dried thyme
- 1 tsp onion powder
- Toppings: smoked paprika, finely chopped parsley
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 400℉ / 200℃.
2) Wash, prick, and bake the potatoes—the latter being for an hour, or until tender.
3) Remove them from the oven and lower the temperature to 350℉ / 175℃.
4) Cut the potatoes lengthways and scoop out the insides into a food processor, leaving enough in the potato that it can hold its shape.
5) Add the remaining ingredients (except the toppings, and half the chickpeas) to the food processor, and blend until smooth.
6) Stuff the filling back into the potato shells (by simple physics of volume, you’ll have a little more than you need, but make it heaped mounds rather than a flat fill-in, and you can probably use most of it, if not all), add the other half of the chickpeas on top and then finally the paprika dusting, and bake for a further 20 minutes.
7) Serve, adding the chopped parsley garnish.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Should You Go Light Or Heavy On Carbs?
- Eat More (Of This) For Lower Blood Pressure
- Level-Up Your Fiber Intake! (Without Difficulty Or Discomfort)
- Our Top 5 Spices: How Much Is Enough For Benefits?
Take care!
Share This Post
-

Finding Geriatric Doctors for Seniors
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝[Can you write about] the availability of geriatric doctors Sometimes I feel my primary isn’t really up on my 70 year old health issues. I would love to find a doctor that understands my issues and is able to explain them to me. Ie; my worsening arthritis in regards to food I eat; in regards to meds vs homeopathic solutions.! Thanks!❞
That’s a great topic, worthy of a main feature! Because in many cases, it’s not just about specialization of skills, but also about empathy, and the gap between studying a condition and living with a condition.
About arthritis, we’re going to do a main feature specifically on that quite soon, but meanwhile, you might like our previous article:
Keep Inflammation At Bay (arthritis being an inflammatory condition)
Share This Post
-
What happens in my brain when I get a migraine? And what medications can I use to treat it?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Migraine is many things, but one thing it’s not is “just a headache”.
“Migraine” comes from the Greek word “hemicrania”, referring to the common experience of migraine being predominantly one-sided.
Some people experience an “aura” preceding the headache phase – usually a visual or sensory experience that evolves over five to 60 minutes. Auras can also involve other domains such as language, smell and limb function.
Migraine is a disease with a huge personal and societal impact. Most people cannot function at their usual level during a migraine, and anticipation of the next attack can affect productivity, relationships and a person’s mental health.
Francisco Gonzelez/Unsplash What’s happening in my brain?
The biological basis of migraine is complex, and varies according to the phase of the migraine. Put simply:
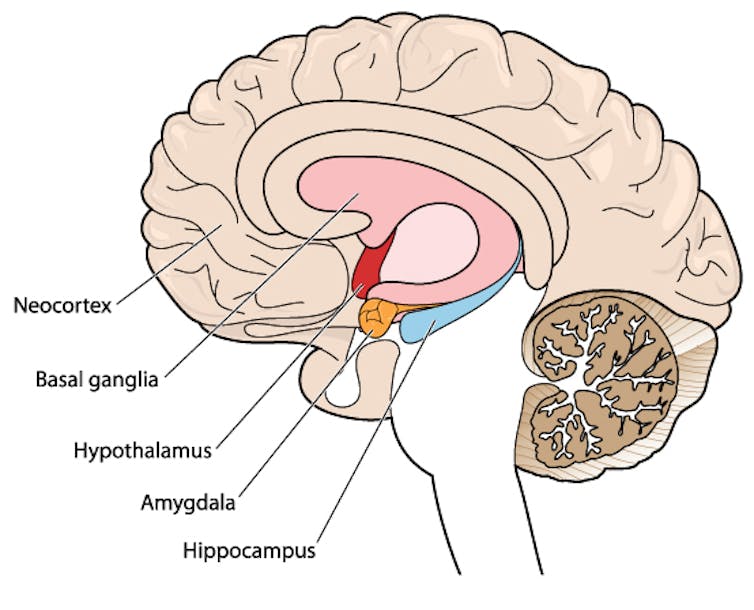
The earliest phase is called the prodrome. This is associated with activation of a part of the brain called the hypothalamus which is thought to contribute to many symptoms such as nausea, changes in appetite and blurred vision.
The hypothalamus is shown here in red. Blamb/Shutterstock Next is the aura phase, when a wave of neurochemical changes occur across the surface of the brain (the cortex) at a rate of 3–4 millimetres per minute. This explains how usually a person’s aura progresses over time. People often experience sensory disturbances such as flashes of light or tingling in their face or hands.
In the headache phase, the trigeminal nerve system is activated. This gives sensation to one side of the face, head and upper neck, leading to release of proteins such as CGRP (calcitonin gene-related peptide). This causes inflammation and dilation of blood vessels, which is the basis for the severe throbbing pain associated with the headache.
Finally, the postdromal phase occurs after the headache resolves and commonly involves changes in mood and energy.
What can you do about the acute attack?
A useful way to conceive of migraine treatment is to compare putting out campfires with bushfires. Medications are much more successful when applied at the earliest opportunity (the campfire). When the attack is fully evolved (into a bushfire), medications have a much more modest effect.
Aspirin
For people with mild migraine, non-specific anti-inflammatory medications such as high-dose aspirin, or standard dose non-steroidal medications (NSAIDS) can be very helpful. Their effectiveness is often enhanced with the use of an anti-nausea medication.
Triptans
For moderate to severe attacks, the mainstay of treatment is a class of medications called “triptans”. These act by reducing blood vessel dilation and reducing the release of inflammatory chemicals.
Triptans vary by their route of administration (tablets, wafers, injections, nasal sprays) and by their time to onset and duration of action.
The choice of a triptan depends on many factors including whether nausea and vomiting is prominent (consider a dissolving wafer or an injection) or patient tolerability (consider choosing one with a slower onset and offset of action).
As triptans constrict blood vessels, they should be used with caution (or not used) in patients with known heart disease or previous stroke.
Triptans should be used cautiously in patients with heart disease. CDC/Unsplash Gepants
Some medications that block or modulate the release of CGRP, which are used for migraine prevention (which we’ll discuss in more detail below), also have evidence of benefit in treating the acute attack. This class of medication is known as the “gepants”.
Gepants come in the form of injectable proteins (monoclonal antibodies, used for migraine prevention) or as oral medication (for example, rimegepant) for the acute attack when a person has not responded adequately to previous trials of several triptans or is intolerant of them.
They do not cause blood vessel constriction and can be used in patients with heart disease or previous stroke.
Ditans
Another class of medication, the “ditans” (for example, lasmiditan) have been approved overseas for the acute treatment of migraine. Ditans work through changing a form of serotonin receptor involved in the brain chemical changes associated with the acute attack.
However, neither the gepants nor the ditans are available through the Pharmaceutical Benefits Scheme (PBS) for the acute attack, so users must pay out-of-pocket, at a cost of approximately A$300 for eight wafers.
What about preventing migraines?
The first step is to see if lifestyle changes can reduce migraine frequency. This can include improving sleep habits, routine meal schedules, regular exercise, limiting caffeine intake and avoiding triggers such as stress or alcohol.
Despite these efforts, many people continue to have frequent migraines that can’t be managed by acute therapies alone. The choice of when to start preventive treatment varies for each person and how inclined they are to taking regular medication. Those who suffer disabling symptoms or experience more than a few migraines a month benefit the most from starting preventives.
Some people will take medicines to prevent migraines. Tbel Abuseridze/Unsplash Almost all migraine preventives have existing roles in treating other medical conditions, and the physician would commonly recommend drugs that can also help manage any pre-existing conditions. First-line preventives include:
- tablets that lower blood pressure (candesartan, metoprolol, propranolol)
- antidepressants (amitriptyline, venlafaxine)
- anticonvulsants (sodium valproate, topiramate).
Some people have none of these other conditions and can safely start medications for migraine prophylaxis alone.
For all migraine preventives, a key principle is starting at a low dose and increasing gradually. This approach makes them more tolerable and it’s often several weeks or months until an effective dose (usually 2- to 3-times the starting dose) is reached.
It is rare for noticeable benefits to be seen immediately, but with time these drugs typically reduce migraine frequency by 50% or more.
‘Nothing works for me!’
In people who didn’t see any effect of (or couldn’t tolerate) first-line preventives, new medications have been available on the PBS since 2020. These medications block the action of CGRP.
The most common PBS-listed anti-CGRP medications are injectable proteins called monoclonal antibodies (for example, galcanezumab and fremanezumab), and are self-administered by monthly injections.
These drugs have quickly become a game-changer for those with intractable migraines. The convenience of these injectables contrast with botulinum toxin injections (also effective and PBS-listed for chronic migraine) which must be administered by a trained specialist.
Up to half of adolescents and one-third of young adults are needle-phobic. If this includes you, tablet-form CGRP antagonists for migraine prevention are hopefully not far away.
Data over the past five years suggest anti-CGRP medications are safe, effective and at least as well tolerated as traditional preventives.
Nonetheless, these are used only after a number of cheaper and more readily available first-line treatments (all which have decades of safety data) have failed, and this also a criterion for their use under the PBS.
Mark Slee, Associate Professor, Clinical Academic Neurologist, Flinders University and Anthony Khoo, Lecturer, Flinders University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post





Related Posts
-

Lucid Dreaming – by Stephen LaBerge Ph.D.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For any unfamiliar: lucid dreaming means being aware that one is dreaming, while dreaming, and exercising a degree of control over the dream. Superficially, this is fun. But if one really wants to go deeper into it, it can be a lot more:
Dr. Stephen LaBerge takes a science-based approach to lucid dreaming, and in this work provides not only step-by-step instructions of several ways of inducing lucid dreaming, but also, opens the reader’s mind to things that can be done there beyond the merely recreational:
In lucid dreams, he argues and illustrates, it’s possible to talk to parts of one’s own subconscious (Inception, anyone? Yes, this book came first) and get quite an amount of self-therapy done. And that hobby you wish you had more time to practice? The possibilities just became limitless. And who wouldn’t want that?
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

When And Why Do We Pick Up Our Phones?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The School of Life’s Alain de Botton makes the argument that—if we pay attention, if we keep track—there’s an understory to why we pick up our phones:
It’s not about information
Yes, our phones (or rather, the apps therein) are designed to addict us, to draw us back, to keep us scrolling and never let us go. We indeed seek out information like our ancestors once sought out berries; searching, encouraged by a small discovery, looking for more. The neurochemistry is similar.
But when we look at the “when” of picking up our phones, de Botton says, it tells a different story:
We pick them up not to find out what’s going on with the world, but rather specifically to not find out what’s going with ourselves. We pick them up to white out some anxiety we don’t want to examine, a line of thought we don’t want to go down, memories we don’t want to consider, futures we do not want to have to worry about.
And of course, phones do have a great educational potential, are an immensely powerful tool for accessing knowledge of many kinds—if only we can remain truly conscious while using them, and not take them as the new “opiate of the masses”.
De Botton bids us, when next we pick up our phone. ask a brave question:
“If I weren’t allowed to consult my phone right now, what might I need to think about?”
As for where from there? There’s more in the video:
Click Here If The Embedded Video Doesn’t Load Automatically!
Further reading
Making Social Media Work For Your Mental Health
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Cashews vs Peanuts – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cashews to peanuts, we picked the peanuts.
Why?
Another one for “that which is more expensive is not necessarily the healthier”! Although, certainly both are good:
In terms of macros, cashews have about 2x the carbs while peanuts have a little more (healthy!) fat and more than 2x the fiber, meaning that peanuts also enjoy the lower glycemic index. All in all, a fair win for peanuts here.
When it comes to vitamins, cashews have more of vitamins B6 and K, while peanuts have a lot more of vitamins B1, B2, B3, B5, B7, B9, and E. Another easy win for peanuts.
In the category of minerals; cashews have more copper, iron, magnesium, phosphorus, and selenium, while peanuts have more calcium, manganese, and potassium. A win for cashews, this time.
Adding up the sections makes for an overall win for peanuts, but (assuming you are not allergic) enjoy either or both! In fact, enjoying both is best; diversity is good.
Want to learn more?
You might like to read:
Why You Should Diversify Your Nuts!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: