7-Minute Face Fitness For Lymphatic Drainage & Youthful Jawline
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Valeriia Veksler is a registered nurse with a background in cosmetic medicine. She’s been practicing for 7 years, and on the strength of that, is going to teach us how to give our face some love for 7 minutes:
The routine, step by step
Preparation: clean your face and apply your usual moisturizer. Breathe deeply: Inhale through the nose, exhale to release tension.
Neck massage: use fingertips in circular motion from the bottom of the neck to the hairline and back for 30 seconds. This helps promote blood flow to the face.
Sternocleidomastoid massage: use knuckles to massage in circles from the sternal area up to the jawline and down to the collarbone for 30 seconds. Keep posture straight, shoulders down, and relax muscles.
Collarbone pressure: apply and release pressure with fingertips above the collarbones for 30 seconds. This stimulates lymphatic flow and helps reduce puffiness.
Under-chin massage: use knuckles to massage side-to-side under the chin for 30 seconds. Relax the under-chin area and promote lymphatic drainage.
Jawline massage: with knuckles, massage from the chin towards the ears in circular motion for 30 seconds. Relax the jaw.
Nasolabial fold and nose massage: place index fingers near nostrils and move mouth in a “O” shape, then massage around the nostrils and up the nose for 30 seconds.
Smile line lift: press palms on the smile lines and slide hands up towards the temples for 30 seconds. This helps lift the face and sculpt cheekbones.
Under-eye massage: use index fingers in a hook shape, massaging under the eyes along the bone structure for 30 seconds. This promotes blood flow and lymphatic drainage.
Temple lift: use fingertips to lift the area near the left temple for 30 seconds, then assist with the opposite hand to lift further. Repeat on the other side. This reduces crow’s feet and lifts the corners of the eyes.
Forehead lift: place hands on the forehead, lock fingers, and gently elevate the skin upwards. Glide fingers towards the hairline for 30 seconds. This promotes blood flow and smooths the forehead.
Relax 11 Lines: place fingers at the center of the forehead, gently press into the tissue, and let them glide away from each other towards the eyebrows for 30 seconds.
Bonus:
- Ensure good posture throughout.
- Relax, stay mindful, and breathe deeply during the exercises.
- Feel the warmth and energy from improved circulation, after the routine.
For more on all of this plus a visual demonstration of everything, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Top 10 Foods That Promote Lymphatic Drainage and Lymph Flow
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Astaxanthin: Super-Antioxidant & Neuroprotectant

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Think Pink For Brain Health!
Astaxanthin is a carotenoid that’s found in:
- certain marine microalgae
- tiny crustaceans that eat the algae
- fish (and flamingos!) that eat the crustaceans
Yes, it’s the one that makes things pink.
But it does a lot more than that…
Super-antioxidant
Move over, green tea! Astaxanthin has higher antioxidant activity than most carotenoids. For example, it is 2–5 times more effective than alpha-carotene, lutein, beta-carotene, and lycopene:
Antioxidant activities of astaxanthin and related carotenoids
We can’t claim credit for naming it a super-antioxidant though, because:
Astaxanthin: A super antioxidant from microalgae and its therapeutic potential
Grow new brain cells
Axtaxanthin is a neuroprotectant, but that’s to be expected from something with such a powerful antioxidant ability.
What’s more special to astaxanthin is that it assists continued adult neurogenesis (creation of new brain cells):
❝The unique chemical structure of astaxanthin enables it to cross the blood-brain barrier and easily reach the brain, where it may positively influence adult neurogenesis.
Furthermore, astaxanthin appears to modulate neuroinflammation by suppressing the NF-κB pathway, reducing the production of pro-inflammatory cytokines, and limiting neuroinflammation associated with aging and chronic microglial activation.
By modulating these pathways, along with its potent antioxidant properties, astaxanthin may contribute to the restoration of a healthy neurogenic microenvironment, thereby preserving the activity of neurogenic niches during both normal and pathological aging. ❞
That first part is very important, by the way! There are so many things that our brain needs, and we can eat, but the molecules are unable to pass the blood-brain barrier, meaning they either get wasted, or used elsewhere, or dismantled for their constituent parts. In this case, it zips straight into the brain instead.
See also:
How To Grow New Brain Cells (At Any Age)
(Probably) good for the joints, too
First, astaxanthin got a glowing report in a study we knew not to trust blindly:
…and breathe. What a title that was! But, did you catch why it’s not to be trusted blindly? It was down at the bottom…
❝Conflict of interest statement
NOVAREX Co., Ltd. funded the study. Valensa International provided the FlexPro MD® ingredients, and NOVAREX Co., Ltd. encapsulated the test products (e.g., both FlexPro MD® and placebo)❞
Studies where a supplement company funded the study are not necessarily corrupt, but they can certainly sway publication bias, i.e. the company funds a bunch of studies and then pulls funding from the ones that aren’t going the way it wants.
So instead let’s look at:
Astaxanthin attenuates joint inflammation induced by monosodium urate crystals
and
Astaxanthin ameliorates cartilage damage in experimental osteoarthritis
…which had no such conflicts of interest.
They agree that astaxanthin indeed does the things (attenuates joint inflammation & ameliorates cartilage damage).
However, they are animal studies (rats), so we’d like to see studies with humans to be able to say for sure how much it helps these things.
Summary of benefits
Based on the available research, astaxanthin…
- is indeed a super-antioxidant
- is a neuroprotective agent
- also assists adult neurogenesis
- is probablygood for joints too
How much do I take, and is it safe?
A 2019 safety review concluded:
❝Recommended or approved doses varied in different countries and ranged between 2 and 24 mg.
We reviewed 87 human studies, none of which found safety concerns with natural astaxanthin supplementation, 35 with doses ≥12 mg/day.❞
Source: Astaxanthin: How much is too much? A safety review
In short: for most people, it’s very safe and well-tolerated. If you consume it to an extreme, you will likely turn pink, much as you would turn orange if you did the same thing with carrots. But aside from that, the risks appear to be minimal.
However! If you have a seafood allergy, please take care to get a supplement that’s made from microalgae, not one that’s made from krill or other crustaceans, or from other creatures that eat those.
Where can I get it?
We don’t sell it, but here’s an example product on Amazon, for your convenience
Enjoy!
Share This Post
-

Brain Food – by Dr. Lisa Mosconi
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We know that we should eat for brain health, but often that knowledge doesn’t go a lot further than “we should eat some nuts… but also not the wrong nuts, which would be bad”.
However, as Dr. Lisa Mosconi lays out for us, there’s a lot more than that!
This book is as much a treatise of brain health in the context of nutrition, as it is a “eat this and avoid that” guide.
Which is good, because our brains don’t exist in isolation, and nor do the nutrients that we consume. Put it this way:
We have a tendecy to think of our diets as a set of slider-bars, “ok, that’s 104% of my daily intake of fiber, I need another 10g protein and that’ll be at 100%, I’ve had 80% of the vitamin C that I need, and…”
Whereas in reality: much of what we eat interacts positively or negatively with other things, and thus needs to be kept in balance. And not only that, but other peri-nutritional factors play a big part too! From obvious things like hydration, to less obvious things like maintaining good gut microbiota, our brains rely on us to do a lot of things for them.
This book is very easy-reading, though a weakness is it doesn’t tend to summarise key ideas much, give cheat-sheets, that sort of thing. We recommend reading this book with a notebook to the side, to jot down things you want to attend to in your own dietary habits.
Bottom line: this is an excellent overview of brain health in the context of nutrition, and is more comprehensive than most “eat this for good brain health and avoid that” books.
Click here to check out “Brain Food” on Amazon and treat your brain like it deserves!
Share This Post
-

Spiced Fruit & Nut Chutney
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
‘Tis the season to make the chutney that will then be aged chutney when you want it later! And unlike supermarket varieties with their ingredients list that goes “Sugar, spirit vinegar, inverted glucose-fructose syrup,” this one has an array of health-giving fruits and nuts (just omit the nuts if you or someone you may want to give this to has an allergy), and really nothing bad in here at all. And of course, tasty healthful spices!
You will need
- 2 red onions, chopped
- 1½ cups dried apricots, chopped
- 1½ cups dried figs, chopped
- 1 cup raisins
- ½ cup apple cider vinegar
- ½ cup slivered almonds
- ½ lime, chopped and deseeded
- ¼ bulb garlic, chopped
- 1 hot pepper, chopped (your choice what kind; omit if you don’t like heat at all; multiply if you want more heat)
- 2 tablespoons honey or maple syrup (omit for a less sweet chutney; there is sweetness in the dried fruits already, after all)
- 1 tbsp freshly grated ginger
- 2 tsp sweet cinnamon
- 1 tsp nutmeg
- 1 tsp black pepper
- ½ teaspoon allspice
- ½ MSG or 1 tsp low-sodium salt
- Extra virgin olive oil
Method
(we suggest you read everything at least once before doing anything)
1) Heat some oil in a heavy-based pan that will be large enough for all ingredients to go into eventually. Fry the onions on a gentle heat for around 15 minutes. We don’t need to caramelize them yet (this will happen with time), but we do want them soft and sweet already.
2) Add the ginger, garlic, and chili, and stir in well.
3) When the onions start to brown, add the fruit and stir well to mix thoroughly.
4) Add the honey or maple syrup (if using), and the vinegar; add the remaining spices/seasonings, so everything is in there now except the almonds.
5) Cook gently for another 30 minutes while stirring. At some point it’ll become thick and sticky; add a little water as necessary. You don’t want to drown it, but you do want it to stay moist. It’ll probably take only a few tablespoons of added water in total, but add them one at a time and stir in before judging whether more is needed. By the end of the 30 minutes, it should be more solid, to the point it can stand up by itself.
6) Add the almonds, stir to combine, and leave to cool. Put it in jars until you need it (or perhaps give it as gifts).
Alternative method: if you don’t want to be standing at a stove stirring for about an hour in total, you can use a slow cooker / crock pot instead. Put the same ingredients in the same order, but don’t stir them, just leave them in layers (this is because of the pattern of heat distribution; it’ll be hotter at the bottom, so the things that need to be more cooked should be there, and the design means they won’t burn) for about two hours, then stir well to mix thoroughly, and leave it for another hour or two, before turning it off to let it cool. Put it in jars until you need it (or perhaps give it as gifts).

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Top 8 Fruits That Prevent & Kill Cancer ← figs and apricots appear here
- Apricots vs Peaches – Which is Healthier? ← have a guess
- Almonds vs Walnuts – Which is Healthier? ← almonds won, but walnuts were close and would also work in this recipe
- Pistachios vs Almonds – Which is Healthier? ← almonds won, but pistachios were close and would also work in this recipe
- Our Top 5 Spices: How Much Is Enough For Benefits? ← we scored 4/5 today!
Take care!
Share This Post



Related Posts
-
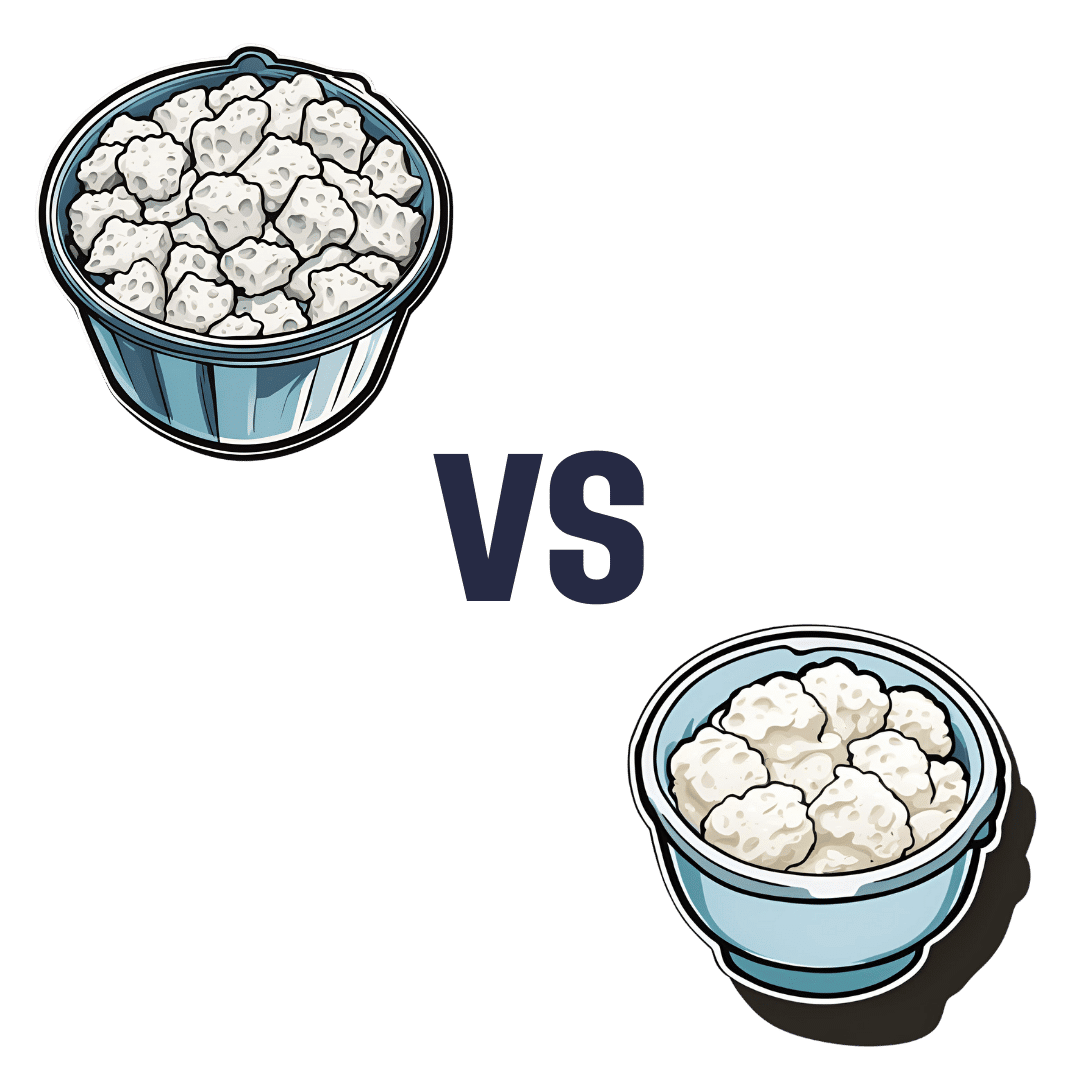
Cottage Cheese vs Ricotta – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cottage cheese to ricotta, we picked the ricotta.
Why?
Cottage cheese is a famous health food, mostly for being a low-fat, low-carb, source of protein. And yet, ricotta beats it in most respects.
Looking at the macros first, cottage cheese has more carbs, while ricotta has more protein and fat. The fat profile is pretty much the same, and in both cases it’s two thirds saturated fat, which isn’t good in either case, but cottage cheese has less overall fat which means less saturated fat in total even if the percentage is the same. Because the difference in carbs and protein is not large, while ricotta has considerably more fat, we’ll call this category a win for cottage cheese.
In terms of vitamins, cottage cheese has more of vitamins B1, B5, and B12, while ricotta has more of vitamins A, B2, B3, B9, D, E, and K, so this one’s a win for ricotta.
In the category of minerals, cottage cheese has slightly more copper, while ricotta has much more calcium, iron, magnesium, manganese, potassium, selenium, and zinc. In particular, 2.5x more calcium, and 5x more iron! An easy and clear win for ricotta here.
Taking everything into account: yes, cottage cheese has less fat (and thus, in total, less saturated fat, although the percentage is the same), but that doesn’t make up for ricotta winning in pretty much every other respect. Still, enjoy either or both (in moderation!) if you be so inclined.
Want to learn more?
You might like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Sleep Through Insomnia – by Dr. Brandon Peters
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what this is not: a guide to get better sleep tonight.
Rather, what it is: a guide to get better sleep in the near future (six weeks).
The way it delivers this is primarily Cognitive Behavioral Therapy for Insomnia (CBT-I), in 6 weekly lessons, each divided into 3 activities:
- Reflection
- Education
- Setting goals
Now, all parts are important, but we’d say the biggest value here is in the education segment, in part because it helps the reader understand why the reflection is important, and how to usefully set the goals.
“Reflection” may sound quite wishy-washy, but in fact it is very science-based, with questions as prompts, which effectively amount to the “gathering data” part of science.
“Setting goals”, for its part, is intended to be a progressive, step-by-step approach to get you to where you want to be with your sleep.
The style is instructional pop-science, with everything made easy to understand. There are an abundance of scientific references for those who wish to delve further, and sometimes he does go into more neurological detail than a book written by a psychologist might (Dr. Peters being a medical doctor, board-certified in neurology and sleep medicine, and with extensive training in CBT-I).
Bottom line: if you’d like to sleep better and you have the will to commit to a 6-week program (which will not ask anything arduous of you, but you will need to show up for it and do the things), then this book can give you a much better long-term fix than telling you to change your sheets and put your phone away.
Click here to check out Sleep Through Insomnia, and sleep easy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Reduce Your Skin Tag Risk
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝As I get older, I seem to be increasingly prone to skin tags, which appear, seemingly out of nowhere, on my face, chest and back. My dermatologist happily burns them off – but is there anything I can do to prevent them?!❞
Not a lot! But, potentially something.
The main risk factor for skin tags is genetic, and you can’t change that in any easy way.
The other main risk factors are connected to each other:
Skin folds, and chafing
Skin tags mostly appear where chafing happens. This can be, for example:
- Inside joint articulations (especially groin and armpits)
- Between fat rolls (if you have them)
So, if you have fat rolls, then losing weight will also reduce the risk of skin tags.
Additionally, obesity and some often-related problems such as diabetes, hypertension, and an atherogenic lipid profile also increase the risk of skin tags (amongst other more serious things):
See: Association of Skin Tag with Metabolic Syndrome and its Components
As for the chafing, this can be reduced in various ways, including:
- losing weight if (and only if) you are carrying excess weight
- dressing against chafing (consider your underwear choices, for example)
- keeping hair in the armpits and groin (it’s part of what it’s there for)
See also: Simply The Pits: These Underarm Myths!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: