4 Tips To Stand Without Using Hands
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The “sit-stand” test, getting up off the floor without using one’s hands, is well-recognized as a good indicator of healthy aging, and predictor of longevity. But what if you can’t do it? Rather than struggling, there are exercises to strengthen the body to be able to do this vital movement.
Step by step
Teresa Shupe has been teaching Pilates professionally full-time for over 25 years, and here’s what she has to offer in the category of safe and effective ways of improving balance and posture while doing the sitting-to-standing movement:
- Squat! Doing squats (especially deep ones) regularly strengthens all the parts necessary to effectively complete this movement. If your knees aren’t up to it at first, do the squats with your back against a wall to start with.
- Roll! On your back, cross your feet as though preparing to stand, and rock-and-roll your body forwards. To start with you can “cheat” and use your fingertips to give a slight extra lift. This exercise builds mobility in the various necessary parts of the body, and also strengthens the core—as well as getting you accustomed to using your bodyweight to move your body forwards.
- Lift! This one’s focusing on that last part, and taking it further. Because it may be difficult to get enough momentum initially, you can practice by holding small weights in your hands, to shift your centre of gravity forwards a bit. Unlike many weights exercises, in this case you’re going to transition to holding less weight rather than more, though.
- Complete! Continue from the above, without weights now; use the blades of your feet to stand. If you need to, use your fingertips to give you a touch more lift and stability, and reduce the fingers that you use until you are using none.
For more on each of these as well as a visual demonstration, enjoy this short video:
Click Here If The Embedded Video Doesn’t Load Automatically!
Further reading
For more exercises with a similar approach, check out:
Mobility As A Sporting Pursuit
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Broccoli Sprouts & Sulforaphane

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝How much science is there behind sulforaphane / broccoli spirits and its health claims??❞
So, first of all, what it is: sulforaphane is a compound found in Brassica oleracea, of which species broccoli is a cultivar. It’s found in the other Brassica oleracea cultivars too (e.g. cauliflower, various cabbages, Brussels sprouts, kale, etc), but for whatever reason*, most research has been on broccoli and broccoli sprouts.
*Likely the reason is: research begets research—it’s easier to get funding to expand upon previous research, than it is to break ground on researching a different plant, where for the first third of your paper you have almost no existing scientific literature to cite. So once they got started on broccoli sprouts, everything else has been broccoli sprouts too.
And for clarity on what broccoli sprouts are: this means that when broccoli seeds have been germinated and just begun to sprout, they are harvested and eaten. That’s the one-line explanation, anyway; there’s a little more to it than that, so anyone interested should check out our previous main feature:
Good Things Come In Small Packages: Sprout Your Seeds, Grains, Beans, Etc
…and for more depth than we have room for in a one-page article, check out this book we reviewed:
The Sprout Book: Tap Into The Power Of The Planet’s Most Nutritious Food – by Doug Evans
One thing that the science is clear on: sprouts of a given plant indeed have much higher general nutritional density than their “adult” siblings. And in the case of sulforaphane specifically, it’s about 100x higher in broccoli sprouts than in adult broccoli:
Broccoli or Sulforaphane: Is It the Source or Dose That Matters? ← we suggest skipping down to the section “broccoli-based clinical trials”
So, that prompts the next question: do we care?
In other words: is sulforaphane really particularly important?
Sulforaphane vs cancer
The most well-evidenced health-giving property of sulforaphane is its anticancer activity:
Brassicaceae-Derived Anticancer Agents: Towards a Green Approach to Beat Cancer
A lot of the research there is epidemiological rather than RCTs, and where there are RCTs, they are mostly small ones, like this 10-person broccoli soup study about bioavailability (rather than the effects themselves):
Bioavailability of Glucoraphanin and Sulforaphane from High-Glucoraphanin Broccoli
To get into sulforaphane’s anticancer potential in seriousness, we have to look at a lot of in-vitro studies trialling it to limit carcinogenesis, or to shrink tumors with it, or specifically targetting cancer stem cells with it, which make for quite compelling reading:
A quick aside: if you’re reading that and thinking “Why is sonic the hedgehog in here?” it’s because after the observation of the influence of certain genes that influence cuticular denticles (the growth of spikes) on fruit fly larvae (bearing in mind the fruit fly Drosophila melanogaster is used for so much first- or second-line genetic research, being either the go-to or the go-to after the nematode C. elegans) caused the whole group of genes to get called “hedgehog genes” and then it became scientific convention to name each newly researched gene in that set after a different kind of hedgehog. One of them, instead of being named after a real-world hedgehog species like the others, got named after the videogame character.
Unfortunately, this now means that because the gene is associated with a certain congenital brain disorder, sometimes a doctor has to explain to a family that the reason their baby has a brain defect is because of a mutated sonic hedgehog.
Ok, back to talking about cancer. Let’s just quickly drop a few more papers so it’s clear that this is well-established:
- Multi-targeted prevention of cancer by sulforaphane ← this shows how it works on the cellular level
- Cruciferous vegetables: dietary phytochemicals for cancer prevention ← this shows how it works on the population level
However, that’s not the only established benefit:
❝SFN has other beneficial effects in addition to cancer protection. SFN exhibits neuroprotective effects and is implemented in treating conditions such as traumatic brain injury, Alzheimer’s disease and Parkinson’s disease.❞
Source: Sulforaphane in broccoli: The green chemoprevention!! Role in cancer prevention and therapy
Now, after the extract we quoted above, the rest of the section “other health benefits of sulforaphane” includes a lot of speculation, weak science, and/or things attributable to other phytochemicals in broccoli, including various polyphenols, vitamins, and minerals.
About those broccoli spirits
Ok, we know it was a typo, but… Actually, there is something worth mentioning here, and that’s that sulforaphane is only activated when glucoraphanin (its inactive form) comes into contact with myrosinase (an enzyme that’s only released when the plant is damaged).
In other words, it’s necessary to injure the broccoli before consuming it, in order to release the
spiritsmyrosinase. Now, while very few people are out there swallowing adult broccoli plants whole, it could well happen that people might wolf down uncut broccoli sprouts, since they are only small, after all.For this reason, it’s best that broccoli, even if it’s broccoli sprouts, be cut while raw before consumption.
In terms of cooking, heat in excess of 140℃ / 284℉ will destroy the glucoraphanin, and less/no glucoraphanin means less/no sulforaphane.
So, enjoying them raw or lightly steaming them seems to be best for this purpose:
Impact of thermal processing on sulforaphane yield from broccoli (Brassica oleracea L. ssp. italica)
Just want a supplement?
Many studies (including some cited by the research reviews we cited above) deal with sulforaphane in extract form, rather than whole plants, so there’s no shame in taking it that way if you’re not a fan of broccoli.
We don’t sell it, but here for your convenience is an example product on Amazon 😎
Enjoy!
Share This Post
-

The Energy Plan – by James Collins
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There’s a lot of conflicting advice out there about how we should maintain our energy levels, for example:
- Eat fewer carbs!
- Eat more carbs!
- Eat slow-release carbs!
- Eat quick-release carbs!
- Practise intermittent fasting!
- Graze constantly throughout the day!
- Forget carbs and focus on fats!
- Actually it’s all about B-vitamins!
…and so on.
What Collins does differently is something much less-often seen:
Here, we’re advised on how to tailor our meals to our actual lifestyle, taking into account the day we actually have each day. For example:
- What will our energy needs be for the day?
- Will our needs be intense, or long, or both, or neither?
- What kind of recovery have we had, or do we need, from previous activities?
- Do we need to replace lost muscle glycogen, or are we looking to trim the fat?
- Are we doing a power-up or just maintenance today?
Rather than bidding us have a five-way spreadsheet and do advanced mathematics for every meal, though, Collins has done the hard work for us. The book explains the various principles in a casual format with a light conversational tone, and gives us general rules to follow.
These rules cover what to do for different times of day… and also, at different points in our life (the metabolic needs of a 13-year-old, 33-year-old, and 83-year-old, are very different!). That latter’s particularly handy, as a lot of books assume an age bracket for the reader, and this one doesn’t.
In short: a great book for anyone who wants to keep their energy levels up (throughout life’s ups and downs in activity) without piling on the pounds or starving oneself.
Click here to check out The Energy Plan on Amazon and fuel your days better!
Share This Post
-

Synergistic Brain-Training
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Let The Games Begin (But It Matters What Kind)
Exercise is good for brain health; we’ve written about this before, for example:
How To Reduce Your Alzheimer’s Risk ← there are many advices here, but exercise, especially cardiovascular exercise in this case, is an important item on the list!
Today it’s Psychology Sunday though, and we’re going to talk about looking after brain health by means of brain-training, via games.
“Brain-training” gets a lot of hype and flak:
- Hype: do sudoku every day and soon you will have an IQ of 200 and still have a sharp wit at the age of 120
- Flak: brain-training is usually training only one kind of cognitive function, with limited transferability to the rest of life
The reality is somewhere between the two. Brain training really does improve not just outwardly measurable cognitive function, but also internally measurable improvements visible on brain scans, for example:
- Cognitive training modified age-related brain changes in older adults with subjective memory decline
- Functional brain changes associated with cognitive training in healthy older adults: A preliminary ALE meta-analysis
But what about the transferability?
Let us play
This is where game-based brain-training comes in. And, the more complex the game, the better the benefits, because there is more chance of applicability to life, e.g:
- Sudoku: very limited applicability
- Crosswords: language faculties
- Chess: spatial reasoning, critical path analysis, planning, memory, focus (also unlike the previous two, chess tends to be social for most people, and also involve a lot of reading, if one is keen)
- Computer games: wildly varied depending on the game. While an arcade-style “shoot-em-up” may do little for the brain, there is a lot of potential for a lot of much more relevant brain-training in other kinds of games: it could be planning, problem-solving, social dynamics, economics, things that mirror the day-to-day challenges of running a household, even, or a business.
- It’s not that the skills are useful, by the way. Playing “Stardew Valley” will not qualify you to run a real farm, nor will playing “Civilization” qualify you to run a country. But the brain functions used and trained? Those are important.
It becomes easily explicable, then, why these two research reviews with very similar titles got very different results:
- A Game a Day Keeps Cognitive Decline Away? A Systematic Review and Meta-Analysis of Commercially-Available Brain Training Programs in Healthy and Cognitively Impaired Older Adults
- Game-based brain training for improving cognitive function in community-dwelling older adults: A systematic review and meta-regression
The first review found that game-based brain-training had negligible actual use. The “games” they looked at? BrainGymmer, BrainHQ, CogMed, CogniFit, Dakim, Lumosity, and MyBrainTrainer. In other words, made-for-purpose brain-trainers, not actual computer games per se.
The second reviewfound that game-based training was very beneficial. The games they looked at? They didn’t name them, but based on the descriptions, they were actual multiplayer online turn-based computer games, not made-for-purpose brain-trainers.
To summarize the above in few words: multiplayer online turn-based computer games outperform made-for-purpose brain-trainers for cognitive improvement.
Bringing synergy
However, before you order that expensive gaming-chair for marathon gaming sessions (research suggests a tail-off in usefulness after about an hour of continuous gaming per session, by the way), be aware that cognitive training and (physical) exercise training combined, performed close in time to each other or simultaneously, perform better than the sum of either alone:
See also:
❝Simultaneous training was the most efficacious approach for cognition, followed by sequential combinations and cognitive training alone, and significantly better than physical exercise.
Our findings suggest that simultaneously and sequentially combined interventions are efficacious for promoting cognitive alongside physical health in older adults, and therefore should be preferred over implementation of single-domain training❞
~ Dr. Hanna Malmberg Gavelin et al.
Take care!
Share This Post

Related Posts
-

With Medical Debt Burdening Millions, a Financial Regulator Steps In to Help
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When President Barack Obama signed legislation in 2010 to create the Consumer Financial Protection Bureau, he said the new agency had one priority: “looking out for people, not big banks, not lenders, not investment houses.”
Since then, the CFPB has done its share of policing mortgage brokers, student loan companies, and banks. But as the U.S. health care system turns tens of millions of Americans into debtors, this financial watchdog is increasingly working to protect beleaguered patients, adding hospitals, nursing homes, and patient financing companies to the list of institutions that regulators are probing.
In the past two years, the CFPB has penalized medical debt collectors, issued stern warnings to health care providers and lenders that target patients, and published reams of reports on how the health care system is undermining the financial security of Americans.
In its most ambitious move to date, the agency is developing rules to bar medical debt from consumer credit reports, a sweeping change that could make it easier for Americans burdened by medical debt to rent a home, buy a car, even get a job. Those rules are expected to be unveiled later this year.
“Everywhere we travel, we hear about individuals who are just trying to get by when it comes to medical bills,” said Rohit Chopra, the director of the CFPB whom President Joe Biden tapped to head the watchdog agency in 2021.
“American families should not have their financial lives ruined by medical bills,” Chopra continued.
The CFPB’s turn toward medical debt has stirred opposition from collection industry officials, who say the agency’s efforts are misguided. “There’s some concern with a financial regulator coming in and saying, ‘Oh, we’re going to sweep this problem under the rug so that people can’t see that there’s this medical debt out there,’” said Jack Brown III, a longtime collector and member of the industry trade group ACA International.
Brown and others question whether the agency has gone too far on medical billing. ACA International has suggested collectors could go to court to fight any rules barring medical debt from credit reports.
At the same time, the U.S. Supreme Court is considering a broader legal challenge to the agency’s funding that some conservative critics and financial industry officials hope will lead to the dissolution of the agency.
But CFPB’s defenders say its move to address medical debt simply reflects the scale of a crisis that now touches some 100 million Americans and that a divided Congress seems unlikely to address soon.
“The fact that the CFPB is involved in what seems like a health care issue is because our system is so dysfunctional that when people get sick and they can’t afford all their medical bills, even with insurance, it ends up affecting every aspect of their financial lives,” said Chi Chi Wu, a senior attorney at the National Consumer Law Center.
CFPB researchers documented that unpaid medical bills were historically the most common form of debt on consumers’ credit reports, representing more than half of all debts on these reports. But the agency found that medical debt is typically a poor predictor of whether someone is likely to pay off other bills and loans.
Medical debts on credit reports are also frequently riddled with errors, according to CFPB analyses of consumer complaints, which the agency found most often cite issues with bills that are the wrong amount, have already been paid, or should be billed to someone else.
“There really is such high levels of inaccuracy,” Chopra said in an interview with KFF Health News. “We do not want to see the credit reporting system being weaponized to get people to pay bills they may not even owe.”
The aggressive posture reflects Chopra, who cut his teeth helping to stand up the CFPB almost 15 years ago and made a name for himself going after the student loan industry.
Targeting for-profit colleges and lenders, Chopra said he was troubled by an increasingly corporate higher-education system that was turning millions of students into debtors. Now, he said, he sees the health care system doing the same thing, shuttling patients into loans and credit cards and reporting them to credit bureaus. “If we were to rewind decades ago,” Chopra said, “we saw a lot less reliance on tools that banks used to get people to pay.”
The push to remove medical bills from consumer credit reports culminates two years of intensive work by the CFPB on the medical debt issue.
The agency warned nursing homes against forcing residents’ friends and family to assume responsibility for residents’ debts. An investigation by KFF Health News and NPR documented widespread use of lawsuits by nursing homes in communities to pursue friends and relatives of nursing home residents.
The CFPB also has highlighted problems with how hospitals provide financial assistance to low-income patients. Regulators last year flagged the dangers of loans and credit cards that health care providers push on patients, often saddling them with more debt.
And regulators have gone after medical debt collectors. In December, the CFPB shut down a Pennsylvania company for pursuing patients without ensuring the debts were accurate.
A few months before that, the agency fined an Indiana company working with medical debt for violating collection laws. Regulators said the company had “risked harming consumers by pressuring or inducing them to pay debts they did not owe.”
With their business in the crosshairs, debt collectors are warning that cracking down on credit reporting and other collection tools may prompt more hospitals and doctors to demand patients pay upfront for care.
There are some indications this is happening already, as hospitals and clinics push patients to enroll in loans or credit cards to pay their medical bills.
Scott Purcell, CEO of ACA International, said it would be wiser for the federal government to focus on making medical care more affordable. “Here we’re coming up with a solution that only takes money away from providers,” Purcell said. “If Congress was involved, there could be more robust solutions.”
Chopra doesn’t dispute the need for bigger efforts to tackle health care costs.
“Of course, there are broader things that we would probably want to fix about our health care system,” he said, “but this is having a direct financial impact on so many Americans.”
The CFPB can’t do much about the price of a prescription or a hospital bill, Chopra continued. What the federal agency can do, he said, is protect patients if they can’t pay their bills.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Mung Beans vs Black Gram – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
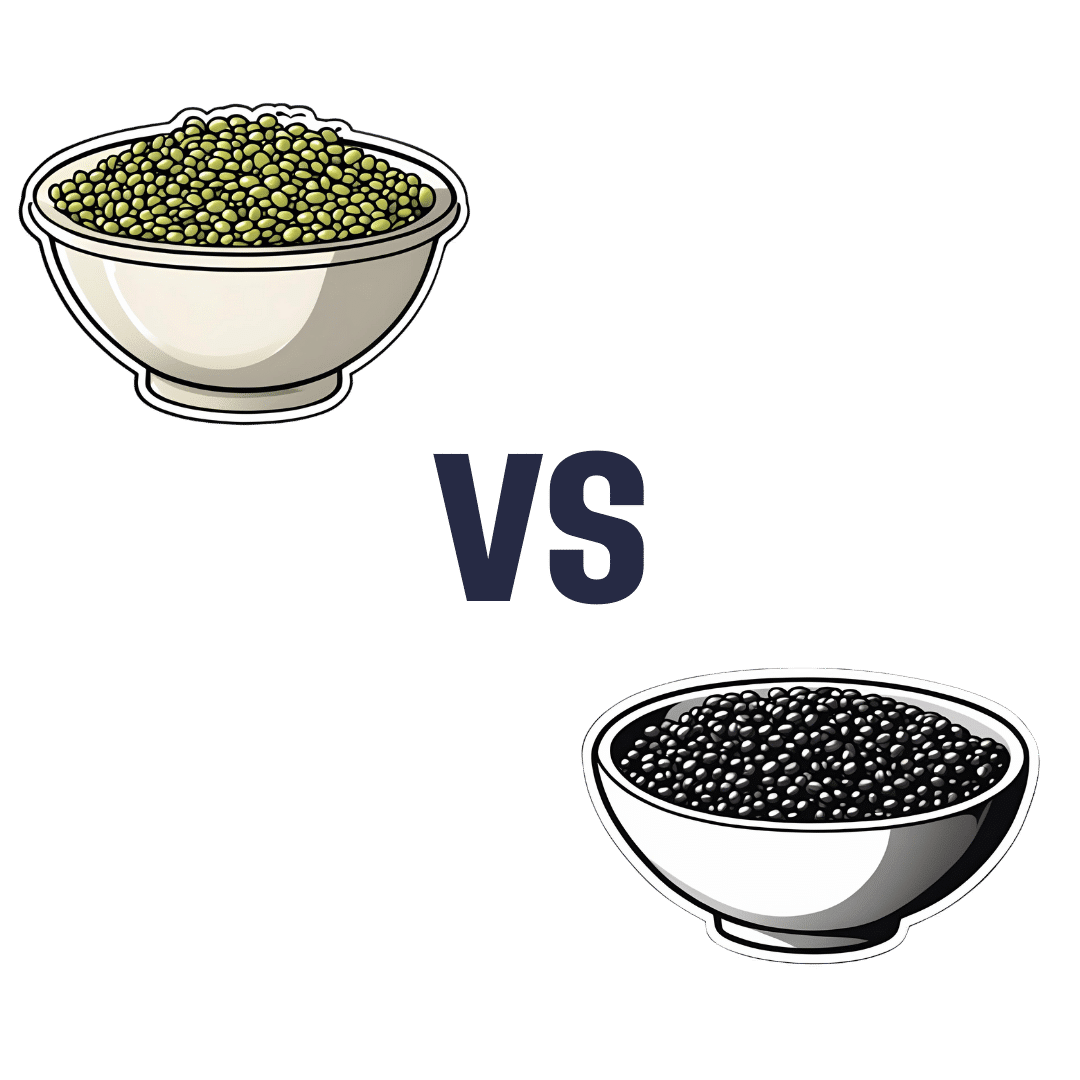
When comparing mung beans to black gram, we picked the black gram.
Why?
Both are great, and it was close!
In terms of macros, the main difference is that mung beans have slightly more fiber, while black gram has slightly more protein. So, it comes down to which we prioritize out of those two, and we’re going to call it fiber and thus hand the win in this category to mung beans—but it’s very close in either case.
In the category of vitamins, mung beans have more of vitamins B1, B6, and B9, while black gram has more of vitamins A, B2, B3, and B5. They’re equal on vitamins C, E, K, and choline. So, a marginal victory by the numbers for black gram here.
When it comes to minerals, mung beans have more copper and potassium, while black gram has more calcium, iron, magnesium, manganese, and phosphorus. They’re equal on selenium and zinc. Another win for black gram.
Adding up the sections makes for an overall win for black gram, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like to read:
What’s Your Plant Diversity Score?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Captivate – by Vanessa van Edwards
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book isn’t just for one area of human interactions. It covers everything from the boardroom to the bedroom (not necessarily a progression with the same person!), business associates, friends, partners, kids, and more.
She presents information in a layered manner, covering for example, chapter-by-chapter:
- the first five minutes
- the first five hours
- the first five days
She also covers such things as:
- starting conversations in a way that makes you memorable (without making it weird!)
- the importance of really listening (and how to do that)
- collecting like-minded people appropriately
- introducing other people! Because a) it’s not all about you, but also b) you’re the person who knows everybody now
- where to stand at parties / networking events!
- dating and early-days dating messages
- reading the room, reading the people
All in all, a great resource for anyone who wants to make (and maintain!) meaningful relationships with those around you.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: