
Your Heart In Their Hands: Surgeon Preferences & Survival Rates
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Unless you are paying entirely out-of-pocket for a heart surgery, you will not usually get final say over which surgeon you get.
The surgeon, however, will have final say over what they actually do when they open you up.
And their preferences, it seems, can make all the difference:
MAG vs SAG
When doing coronary artery bypass grafting, (CABG), surgeons may prefer to do multi-arterial grafting (MAG) or single-arterial grafting (SAG).
Recently, there was a study analysing more than a million Americans who underwent CABG on Medicare over an 18-year period, looking at outcomes for MAG vs SAG.
The superficial news: those who received MAG had much better long-term survival chances than those who received SAG.
However: this may be less to do with the relative merits of the procedures themselves, and more to do with the preferences of the surgeon.
The “eyeball test”
If surgeons look at a patient and think they will not have many years to live after surgery, they may opt for the SAG, as the long-term benefits of the MAG will only manifest in the long-term.
This may seem a little self-defeating (indeed, maybe you won’t live to see the long-term if you don’t get the surgery type with the longer-term survival chances), there can be other factors involved, that may make surgeons more interested in your short-term survival chances.
Or you might just not have enough donor artery tissue available to pick and choose; after all, a person having a coronary artery bypass quite possibly won’t have great arteries in their arm or leg, either.
Or a person could be missing limbs (a common complication, given the comorbidities of both peripheral artery disease, and diabetes).
See also: How To Stay A Step Ahead Of Peripheral Artery Disease
Why it might be ok that things are like this
When factoring in surgeon preference for MAG or SAG as an instrumental variable, no significant difference in long-term survival was observed. This may explain inconsistencies with randomized controlled trials like the Arterial Revascularization Trial (ART), which also found no survival benefit of MAG over SAG.
Also, MAG recipients were generally younger, healthier, and from more resourceful areas, which likely had a further impact on MAG-giving decisions, and/but at the same time, may also have increased survival chances for reasons other than that they got MAG rather than SAG.
Here’s a pop-science article that goes into more detail about this:
Surgeon preferences may explain differences in CABG survival rates
How to look out for yourself, and advocate for yourself
…or your loved one, of course. Now, having a coronary artery bypass surgery of any kind is not a fun activity; it will be dangerous, it’ll be stressful before and after, and the recovery will often not be an easy time either. However, it is possible to learn more about what is going on / what will happen, ask the right questions, and get the best options for you (which may not always be the same as the best options for someone else).
We wrote about that in more detail here:
Nobody Likes Surgery, But Here’s How To Make It Much Less Bad
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Cannabis Myths vs Reality

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cannabis Myths vs Reality

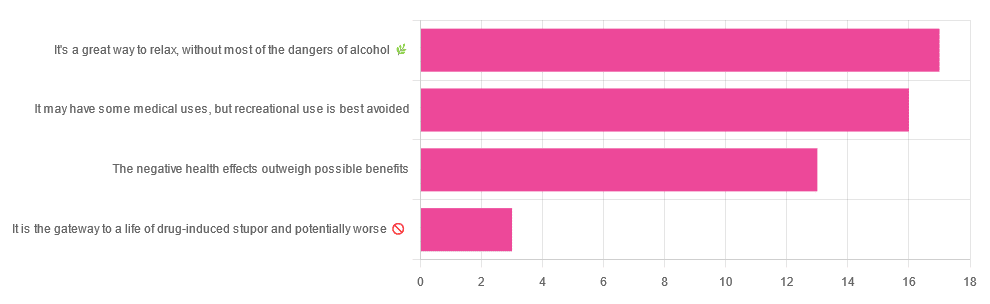
We asked you for your (health-related) opinion on cannabis use—specifically, the kind with psychoactive THC, not just CBD. We got the above-pictured, below-described, spread of responses:
- A little over a third of you voted for “It’s a great way to relax, without most of the dangers of alcohol”.
- A little under a third of you voted for “It may have some medical uses, but recreational use is best avoided”.
- About a quarter of you voted for “The negative health effects outweigh the possible benefits”
- Three of you voted for “It is the gateway to a life of drug-induced stupor and potentially worse”
So, what does the science say?
A quick legal note first: we’re a health science publication, and are writing from that perspective. We do not know your location, much less your local laws and regulations, and so cannot comment on such. Please check your own local laws and regulations in that regard.
Cannabis use can cause serious health problems: True or False?
True. Whether the risks outweigh the benefits is a personal and subjective matter (for example, a person using it to mitigate the pain of late stage cancer is probably unconcerned with many other potential risks), but what’s objectively true is that it can cause serious health problems.
One subscriber who voted for “The negative health effects outweigh the possible benefits” wrote:
❝At a bare minimum, you are ingesting SMOKE into your lungs!! Everyone SEEMS TO BE against smoking cigarettes, but cannabis smoking is OK?? Lung cancer comes in many forms.❞
Of course, that is assuming smoking cannabis, and not consuming it as an edible. But, what does the science say on smoking it, and lung cancer?
There’s a lot less research about this when it comes to cannabis, compared to tobacco. But, there is some:
❝Results from our pooled analyses provide little evidence for an increased risk of lung cancer among habitual or long-term cannabis smokers, although the possibility of potential adverse effect for heavy consumption cannot be excluded.❞
Read: Cannabis smoking and lung cancer risk: Pooled analysis in the International Lung Cancer Consortium
Another study agreed there appears to be no association with lung cancer, but that there are other lung diseases to consider, such as bronchitis and COPD:
❝Smoking cannabis is associated with symptoms of chronic bronchitis, and there may be a modest association with the development of chronic obstructive pulmonary disease. Current evidence does not suggest an association with lung cancer.❞
Read: Cannabis Use, Lung Cancer, and Related Issues
Cannabis edibles are much safer than smoking cannabis: True or False?
Broadly True, with an important caveat.
One subscriber who selected “It may have some medical uses, but recreational use is best avoided”, wrote:
❝I’ve been taking cannabis gummies for fibromyalgia. I don’t know if they’re helping but they’re not doing any harm. You cannot overdose you don’t become addicted.❞
Firstly, of course consuming edibles (rather than inhaling cannabis) eliminates the smoke-related risk factors we discussed above. However, other risks remain, including the much greater ease of accidentally overdosing.
❝Visits attributable to inhaled cannabis are more frequent than those attributable to edible cannabis, although the latter is associated with more acute psychiatric visits and more ED visits than expected.❞
Note: that “more frequent” for inhaled cannabis, is because more people inhale it than eat it. If we adjust the numbers to control for how much less often people eat it, suddenly we see that the numbers of hospital admissions are disproportionately high for edibles, compared to inhaled cannabis.
Or, as the study author put it:
❝There are more adverse drug events associated on a milligram per milligram basis of THC when it comes in form of edibles versus an inhaled cannabis. If 1,000 people smoked pot and 1,000 people at the same dose in an edible, then more people would have more adverse drug events from edible cannabis.❞
See the numbers: Acute Illness Associated With Cannabis Use, by Route of Exposure
Why does this happen?
- It’s often because edibles take longer to take effect, so someone thinks “this isn’t very strong” and has more.
- It’s also sometimes because someone errantly eats someone else’s edibles, not realising what they are.
- It’s sometimes a combination of the above problems: a person who is now high, may simply forget and/or make a bad decision when it comes to eating more.
On the other hand, that doesn’t mean inhaling it is necessarily safer. As well as the pulmonary issues we discussed previously, inhaling cannabis has a higher risk of cannabinoid hyperemesis syndrome (and the resultant cyclic vomiting that’s difficult to treat).
You can read about this fascinating condition that’s sometimes informally called “scromiting”, a portmanteau of screaming and vomiting:
Cannabinoid Hyperemesis Syndrome
You can’t get addicted to cannabis: True or False?
False. However, it is fair to say that the likelihood of developing a substance abuse disorder is lower than for alcohol, and much lower than for nicotine.
See: Prevalence of Marijuana Use Disorders in the United States Between 2001–2002 and 2012–2013
If you prefer just the stats without the science, here’s the CDC’s rendering of that:
Addiction (Marijuana or Cannabis Use Disorder)
However, there is an interesting complicating factor, which is age. One is 4–7 times more likely to develop a substance abuse disorder, if one starts use as an adolescent, rather than later as an adult:
Cannabis is the gateway to use of more dangerous drugs: True or False?
False, generally speaking. Of course, for any population there will be some outliers, but there appears to be no meaningful causal relation between cannabis use and other substance use:
Interestingly, the strongest association (where any existed at all) was between cannabis use and opioid use. However, rather than this being a matter of cannabis use being a gateway to opioid use, it seems more likely that this is a matter of people looking to both for the same purpose: pain relief.
As a result, growing accessibility of cannabis may actually reduce opioid problems:
- Cannabis as a Gateway Drug for Opioid Use Disorder
- Association between medical cannabis laws and opioid overdose mortality has reversed over time
Some final words…
Cannabis is a complex drug with complex mechanisms and complex health considerations, and research is mostly quite young, due to its historic illegality seriously cramping science by reducing sample sizes to negligible. Simply put, there’s a lot we still don’t know.
Also, we covered some important topics today, but there were others we didn’t have time to cover, such as the other potential psychological benefits—and risks. Likely we’ll revisit those another day.
Lastly, while we’ve covered a bunch of risks today, those of you who said it has fewer and lesser risks than alcohol are quite right—the only reason we couldn’t focus on that more, is because to talk about all the risks of alcohol would make this feature many times longer!
Meanwhile, whether you partake or not, stay safe and stay well.
Share This Post
-

Anti-Inflammatory Cookbook for Beginners – by Melissa Jefferson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For some of us, avoiding inflammatory food is a particularly important consideration. For all of us, it should be anyway.
Sometimes, we know what’s good against inflammation, and we know what’s bad for inflammation… but we might struggle to come up with full meals of just-the-good, especially if we want to not repeat meals every day!
The subtitle is slightly misleading! It says “Countless Easy and Delicious Recipes”, but this depends on your counting ability. Melissa Jefferson gives us 150 anti-inflammatory recipes, which can be combined for a 12-week meal plan. We think that’s enough to at least call it “many”, though.
First comes an introduction to inflammation, inflammatory diseases, and a general overview of what to eat / what to avoid. After that, the main part of the book is divided into sections:
- Breakfasts (20)
- Soups (15)
- Beans & Grains (20)
- Meat (20)
- Fish (20)
- Vegetables (20)
- Sides (15)
- Snacks (10)
- Desserts (10)
If you’ve a knowledge of anti-inflammation diet already, you may be wondering how “Meat” and “Desserts” works.
- The meat section is a matter of going light on the meat and generally favoring white meats, and certainly unprocessed.
- Of course, if you are vegetarian or vegan, substitutions may be in order anyway.
As for the dessert section? A key factor is that fruits and chocolate are anti-inflammatory foods! Just a matter of not having desserts full of sugar, flour, etc.
The recipes themselves are simple and to-the-point, with ingredients, method, and nutritional values. Just the way we like it.
All in all, a fine addition to absolutely anyone’s kitchen library… And doubly so if you have a particular reason to focus on avoiding/reducing inflammation!
Get your copy of “Anti-Inflammatory Cookbook for Beginners” from Amazon today!
Share This Post
-

Should Men Over 50 Get PSA?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Loved the information on prostate cancer. Do recommend your readers get a PSA or equivalent test annually for over 50 yr old men.❞
(This is about: Prostate Health: What You Should Know)
Yep, or best yet, the much more accurate PSE test! But if PSA test is what’s available, it’s a lot better than nothing. And, much as it’s rarely the highlight of anyone’s day, a prostate exam by a suitably qualified professional is also a good idea.
Share This Post

-

Open Your Hips With Better Joint Mechanics (Here’s How)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Most people stretch hips incorrectly, and pushing through painful stretches often leads to little or no progress, which can be discouraging to say the least.
Here’s how to cut through all that and get the results you need:
More than just stretching
Effective hip mobility also requires joint capsule activation, muscle tension release, and nervous system safety. These four exercises meet those needs:
- Banded lunge hip mobilization: in a lunge, loop a resistance band across the hip of your lead leg, extend your back leg, and push your front knee outwards without hip rotation or spinal arching. Hold 15–20 seconds, repeat.
- Weighted butterfly stretch: sit with your feet together, knees out, and rest light/moderate dumbbells on each knee to gently press them down; relax fully, hold 2–3 seconds, repeat 8–10 times.
- Seated hinge with barbell: sit on a bench with your knees bent and your hips open; hold a barbell at your shoulders, brace your core, and hinge forward at hips while keeping your spine neutral; you should feel the stretch in your hips, glutes, and groin. Pause 2–3 seconds, repeat 8–12 times.
- Frog stretch with sliders and weight: hold the “frog” position (knees wide, feet out), for 30–60 seconds; add sliders to move your hips up/down, then rest a plate on your hips and hold another 30–60 seconds.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
The Most Underrated Hip Mobility Exercise (Not Stretching)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Online Eye Exams vs In-Office Eye Exams (Do We Really Need Them?)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Neal Guymon puts things into perspective:
Eye to eye
This eye doctor is, of course, not coming into this completely unbiased. He is not about to say “you don’t need to see an eye doctor”. However, the perspective he shares is useful:
In the category of online eye exams, options include in-office tests with a remote doctor reviewing results, at-home vision tests using a phone or computer, and simple online renewals based on self-reported vision and basic checks.
- A main benefit, of course, is convenience: online exams are quick and flexible, making them ideal if you’re busy, can’t take time off work, or just want to renew a prescription from home.
- There’s obviously a cost advantage too; online exams are usually much cheaper (around $15–$30), especially relevant if you don’t have insurance, but they only cover a small part of what a full exam includes.
- They best suit someone young, healthy, and stable, whose prescription hasn’t changed for years and who has no symptoms or eye issues, because most only assess whether you can see clearly (e.g. 20/20), which is a small fraction of eye health and can miss underlying problems.
In contrast, an in-person eye exam evaluates far more than vision, including your eyelids, tear glands, cornea, retina, eye pressure, blood vessels, eye muscles, and early signs of conditions like cataracts, glaucoma, or macular degeneration
- Without this, serious issues like retinal tears, early glaucoma, inflammation, or contact lens damage can develop without symptoms and would likely be missed online.
- There is also the fact that proper prescribing requires checking lens fit, movement, and effects on your eye, which online renewals don’t reliably assess.
In other words, online exams are convenient and cheap for simple prescription renewals, but they don’t replace a comprehensive in-person exam, which is still the best way to detect and prevent eye disease early.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
5 Follow-Along Exercises To Rapidly Improve Your Eyesight
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Celeriac vs Red Cabbage – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing celeriac to red cabbage, we picked the celeriac.
Why?
In terms of macros, there’s really nothing between them; they have almost identical numbers for fiber, carbs, and protein, so this first round’s a tie.
In the category of vitamins, celeriac has more of vitamins B3, B5, E, and K, while red cabbage has more of vitamins A, B9, and C, yielding a modest win to celeriac here.
Looking at minerals, celeriac has more copper, magnesium, phosphorus, potassium, selenium, and zinc, while red cabbage has more iron and manganese, for a 6:2 win to celeriac in this round.
In other considerations, celeriac has more polyphenols, with, for example, 24x more apigenin than red cabbage. So, that’s another point in celeriac’s favor.
Adding up the sections makes for an overall win for celeriac, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
21 Most Beneficial Polyphenols & What Foods Have Them
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:


