Women are less likely to receive CPR than men. Training on manikins with breasts could help
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If someone’s heart suddenly stops beating, they may only have minutes to live. Doing CPR (cardiopulmonary resusciation) can increase their chances of survival. CPR makes sure blood keeps pumping, providing oxygen to the brain and vital organs until specialist treatment arrives.
But research shows bystanders are less likely to intervene to perform CPR when that person is a woman. A recent Australian study analysed 4,491 cardiac arrests between 2017–19 and found bystanders were more likely to give CPR to men (74%) than women (65%).
Could this partly be because CPR training dummies (known as manikins) don’t have breasts? Our new research looked at manikins available worldwide to train people in performing CPR and found 95% are flat-chested.
Anatomically, breasts don’t change CPR technique. But they may influence whether people attempt it – and hesitation in these crucial moments could mean the difference between life and death.

Heart health disparities
Cardiovascular diseases – including heart disease, stroke and cardiac arrest – are the leading cause of death for women across the world.
But if a woman has a cardiac arrest outside hospital (meaning her heart stops pumping properly), she is 10% less likely to receive CPR than a man. Women are also less likely to survive CPR and more likely to have brain damage following cardiac arrests.

These are just some of many unequal health outcomes women experience, along with transgender and non-binary people. Compared to men, their symptoms are more likely to be dismissed or misdiagnosed, or it may take longer for them to receive a diagnosis.
Bystander reluctance
There is also increasing evidence women are less likely to receive CPR compared to men.
This may be partly due to bystander concerns they’ll be accused of sexual harassment, worry they might cause damage (in some cases based on a perception women are more “frail”) and discomfort about touching a woman’s breast.
Bystanders may also have trouble recognising a woman is experiencing a cardiac arrest.
Even in simulations of scenarios, researchers have found those who intervened were less likely to remove a woman’s clothing to prepare for resuscitation, compared to men. And women were less likely to receive CPR or defibrillation (an electric charge to restart the heart) – even when the training was an online game that didn’t involve touching anyone.
There is evidence that how people act in resuscitation training scenarios mirrors what they do in real emergencies. This means it’s vital to train people to recognise a cardiac arrest and be prepared to intervene, across genders and body types.
Skewed to male bodies
Most CPR training resources feature male bodies, or don’t specify a sex. If the bodies don’t have breasts, it implies a male default.
For example, a 2022 study looking at CPR training across North, Central and South America, found most manikins available were white (88%), male (94%) and lean (99%).

These studies reflect what we see in our own work, training other health practitioners to do CPR. We have noticed all the manikins available to for training are flat-chested. One of us (Rebecca) found it difficult to find any training manikins with breasts.
A single manikin with breasts
Our new research investigated what CPR manikins are available and how diverse they are. We identified 20 CPR manikins on the global market in 2023. Manikins are usually a torso with a head and no arms.
Of the 20 available, five (25%) were sold as “female” – but only one of these had breasts. That means 95% of available CPR training manikins were flat-chested.
We also looked at other features of diversity, including skin tone and larger bodies. We found 65% had more than one skin tone available, but just one was a larger size body. More research is needed on how these aspects affect bystanders in giving CPR.
Breasts don’t change CPR technique
CPR technique doesn’t change when someone has breasts. The barriers are cultural. And while you might feel uncomfortable, starting CPR as soon as possible could save a life.
Signs someone might need CPR include not breathing properly or at all, or not responding to you.
To perform effective CPR, you should:
- put the heel of your hand on the middle of their chest
- put your other hand on the top of the first hand, and interlock fingers (keep your arms straight)
- press down hard, to a depth of about 5cm before releasing
- push the chest at a rate of 100-120 beats per minute (you can sing a song) in your head to help keep time!)
https://www.youtube.com/embed/Plse2FOkV4Q?wmode=transparent&start=94 An example of how to do CPR – with a flat-chested manikin.
What about a defibrillator?
You don’t need to remove someone’s bra to perform CPR. But you may need to if a defibrillator is required.
A defibrillator is a device that applies an electric charge to restore the heartbeat. A bra with an underwire could cause a slight burn to the skin when the debrillator’s pads apply the electric charge. But if you can’t remove the bra, don’t let it delay care.
What should change?
Our research highlights the need for a range of CPR training manikins with breasts, as well as different body sizes.
Training resources need to better prepare people to intervene and perform CPR on people with breasts. We also need greater education about women’s risk of getting and dying from heart-related diseases.
Jessica Stokes-Parish, Assistant Professor in Medicine, Bond University and Rebecca A. Szabo, Honorary Senior Lecturer in Critical Care and Obstetrics, Gynaecology and Newborn Health, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Sweet Cinnamon vs Regular Cinnamon – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing sweet cinnamon to regular cinnamon, we picked the sweet.
Why?
In this case, it’s not close. One of them is health-giving and the other is poisonous (but still widely sold in supermarkets, especially in the US and Canada, because it is cheaper).
It’s worth noting that “regular cinnamon” is a bit of a misnomer, since sweet cinnamon is also called “true cinnamon”. The other cinnamon’s name is formally “cassia cinnamon”, but marketers don’t tend to call it that, preferring to calling it simply “cinnamon” and hope consumers won’t ask questions about what kind, because it’s cheaper.
Note: this too is especially true in the US and Canada, where for whatever reason sweet cinnamon seems to be more difficult to obtain than in the rest of the world.
In short, both cinnamons contain cinnamaldehyde and coumarin, but:
- Sweet/True cinnamon contains only trace amounts of coumarin
- Regular/Cassia cinnamon contains about 250x more coumarin
Coumarin is heptatotoxic, meaning it poisons the liver, and the recommended safe amount is 0.1mg/kg, so it’s easy to go over that with just a couple of teaspoons of cassia cinnamon.
You might be wondering: how can they get away with selling something that poisons the liver? In which case, see also: the alcohol aisle. Selling toxic things is very common; it just gets normalized a lot.
Cinnamaldehyde is responsible for cinnamon’s healthier properties, and is found in reasonable amounts in both cinnamons. There is about 50% more of it in the regular/cassia than in the sweet/true, but that doesn’t come close to offsetting the potential harm of its higher coumarin content.
Want to learn more?
You may like to read:
- A Tale Of Two Cinnamons ← this one has more of the science of coumarin toxicity, as well as discussing (and evidencing) cinnamaldehyde’s many healthful properties against inflammation, cancer, heart disease, neurodegeneration, etc
Enjoy!
Share This Post
-

I have a stuffy nose, how can I tell if it’s hay fever, COVID or something else?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hay fever (also called allergic rhinitis) affects 24% of Australians. Symptoms include sneezing, a runny nose (which may feel blocked or stuffy) and itchy eyes. People can also experience an itchy nose, throat or ears.
But COVID is still spreading, and other viruses can cause cold-like symptoms. So how do you know which one you’ve got?

Lysenko Andrii/Shutterstock Remind me, how does hay fever cause symptoms?
Hay fever happens when a person has become “sensitised” to an allergen trigger. This means a person’s body is always primed to react to this trigger.
Triggers can include allergens in the air (such as pollen from trees, grasses and flowers), mould spores, animals or house dust mites which mostly live in people’s mattresses and bedding, and feed on shed skin.
When the body is exposed to the trigger, it produces IgE (immunoglobulin E) antibodies. These cause the release of many of the body’s own chemicals, including histamine, which result in hay fever symptoms.
People who have asthma may find their asthma symptoms (cough, wheeze, tight chest or trouble breathing) worsen when exposed to airborne allergens. Spring and sometimes into summer can be the worst time for people with grass, tree or flower allergies.
However, animal and house dust mite symptoms usually happen year-round.
Ryegrass pollen is a common culprit. bangku ceria/Shutterstock What else might be causing my symptoms?
Hay fever does not cause a fever, sore throat, muscle aches and pains, weakness, loss of taste or smell, nor does it cause you to cough up mucus.
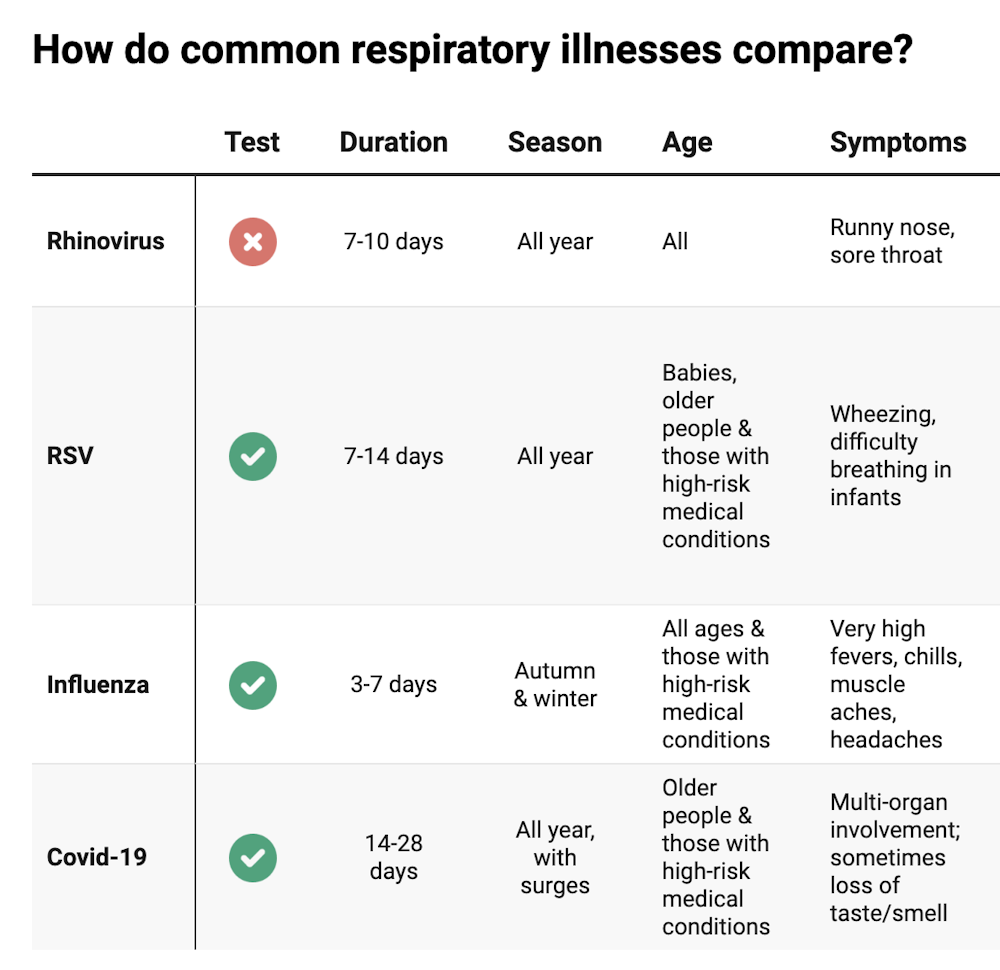
These symptoms are likely to be caused by a virus, such as COVID, influenza, respiratory syncytial virus (RSV) or a “cold” (often caused by rhinoviruses). These conditions can occur all year round, with some overlap of symptoms:
Natasha Yates/The Conversation COVID still surrounds us. RSV and influenza rates appear higher than before the COVID pandemic, but it may be due to more testing.
So if you have a fever, sore throat, muscle aches/pains, weakness, fatigue, or are coughing up mucus, stay home and avoid mixing with others to limit transmission.
People with COVID symptoms can take a rapid antigen test (RAT), ideally when symptoms start, then isolate until symptoms disappear. One negative RAT alone can’t rule out COVID if symptoms are still present, so test again 24–48 hours after your initial test if symptoms persist.
You can now test yourself for COVID, RSV and influenza in a combined RAT. But again, a negative test doesn’t rule out the virus. If your symptoms continue, test again 24–48 hours after the previous test.
If it’s hay fever, how do I treat it?
Treatment involves blocking the body’s histamine release, by taking antihistamine medication which helps reduce the symptoms.
Doctors, nurse practitioners and pharmacists can develop a hay fever care plan. This may include using a nasal spray containing a topical corticosteroid to help reduce the swelling inside the nose, which causes stuffiness or blockage.
Nasal sprays need to delivered using correct technique and used over several weeks to work properly. Often these sprays can also help lessen the itchy eyes of hay fever.
Drying bed linen and pyjamas inside during spring can lessen symptoms, as can putting a smear of Vaseline in the nostrils when going outside. Pollen sticks to the Vaseline, and gently blowing your nose later removes it.
People with asthma should also have an asthma plan, created by their doctor or nurse practitioner, explaining how to adjust their asthma reliever and preventer medications in hay fever seasons or on allergen exposure.
People with asthma also need to be alert for thunderstorms, where pollens can burst into tinier particles, be inhaled deeper in the lungs and cause a severe asthma attack, and even death.
What if it’s COVID, RSV or the flu?
Australians aged 70 and over and others with underlying health conditions who test positive for COVID are eligible for antivirals to reduce their chance of severe illness.
Most other people with COVID, RSV and influenza will recover at home with rest, fluids and paracetamol to relieve symptoms. However some groups are at greater risk of serious illness and may require additional treatment or hospitalisation.
For RSV, this includes premature infants, babies 12 months and younger, children under two who have other medical conditions, adults over 75, people with heart and lung conditions, or health conditions that lessens the immune system response.
For influenza, people at higher risk of severe illness are pregnant women, Aboriginal people, people under five or over 65 years, or people with long-term medical conditions, such as kidney, heart, lung or liver disease, diabetes and decreased immunity.
If you’re concerned about severe symptoms of COVID, RSV or influenza, consult your doctor or call 000 in an emergency.
If your symptoms are mild but persist, and you’re not sure what’s causing them, book an appointment with your doctor or nurse practitioner. Although hay fever season is here, we need to avoid spreading other serious infectious.
For more information, you can call the healthdirect helpline on 1800 022 222 (known as NURSE-ON-CALL in Victoria); use the online Symptom Checker; or visit healthdirect.gov.au or the Australian Society of Clinical Immunology and Allergy.
Deryn Thompson, Eczema and Allergy Nurse; Lecturer, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

The voice in your head may help you recall and process words. But what if you don’t have one?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Can you imagine hearing yourself speak? A voice inside your head – perhaps reciting a shopping list or a phone number? What would life be like if you couldn’t?
Some people, including me, cannot have imagined visual experiences. We cannot close our eyes and conjure an experience of seeing a loved one’s face, or imagine our lounge room layout – to consider if a new piece of furniture might fit in it. This is called “aphantasia”, from a Greek phrase where the “a” means without, and “phantasia” refers to an image. Colloquially, people like myself are often referred to as having a “blind mind”.
While most attention has been given to the inability to have imagined visual sensations, aphantasics can lack other imagined experiences. We might be unable to experience imagined tastes or smells. Some people cannot imagine hearing themselves speak.
A recent study has advanced our understanding of people who cannot imagine hearing their own internal monologue. Importantly, the authors have identified some tasks that such people are more likely to find challenging.
fizkes/Shutterstock What the study found
Researchers at the University of Copenhagen in Denmark and at the University of Wisconsin-Madison in the United States recruited 93 volunteers. They included 46 adults who reported low levels of inner speech and 47 who reported high levels.
Both groups were given challenging tasks: judging if the names of objects they had seen would rhyme and recalling words. The group without an inner monologue performed worse. But differences disappeared when everyone could say words aloud.
Importantly, people who reported less inner speech were not worse at all tasks. They could recall similar numbers of words when the words had a different appearance to one another. This negates any suggestion that aphants (people with aphantasia) simply weren’t trying or were less capable.
Hearing our own imagined voice may play an important role in word processing. sutadimages/Shutterstock A welcome validation
The study provides some welcome evidence for the lived experiences of some aphants, who are still often told their experiences are not different, but rather that they cannot describe their imagined experiences. Some people feel anxiety when they realise other people can have imagined experiences that they cannot. These feelings may be deepened when others assert they are merely confused or inarticulate.
In my own aphantasia research I have often quizzed crowds of people on their capacity to have imagined experiences.
Questions about the capacity to have imagined visual or audio sensations tend to be excitedly endorsed by a vast majority, but questions about imagined experiences of taste or smell seem to cause more confusion. Some people are adamant they can do this, including a colleague who says he can imagine what combinations of ingredients will taste like when cooked together. But other responses suggest subtypes of aphantasia may prove to be more common than we realise.
The authors of the recent study suggest the inability to imagine hearing yourself speak should be referred to as “anendophasia”, meaning without inner speech. Other authors had suggested anauralia (meaning without auditory imagery). Still other researchers have referred to all types of imagined sensation as being different types of “imagery”.
Having consistent names is important. It can help scientists “talk” to one another to compare findings. If different authors use different names, important evidence can be missed.
We’re starting to broaden our understanding of the senses and how we imagine them. Napat Chaichanasiri/Shutterstock We have more than 5 senses
Debate continues about how many senses humans have, but some scientists reasonably argue for a number greater than 20.
In addition to the five senses of sight, smell, taste, touch and hearing, lesser known senses include thermoception (our sense of heat) and proprioception (awareness of the positions of our body parts). Thanks to proprioception, most of us can close our eyes and touch the tip of our index finger to our nose. Thanks to our vestibular sense, we typically have a good idea of which way is up and can maintain balance.
It may be tempting to give a new name to each inability to have a given type of imagined sensation. But this could lead to confusion. Another approach would be to adapt phrases that are already widely used. People who are unable to have imagined sensations commonly refer to ourselves as “aphants”. This could be adapted with a prefix, such as “audio aphant”. Time will tell which approach is adopted by most researchers.
Why we should keep investigating
Regardless of the names we use, the study of multiple types of inability to have an imagined sensation is important. These investigations could reveal the essential processes in human brains that bring about a conscious experience of an imagined sensation.
In time, this will not only lead to a better understanding of the diversity of humans, but may help uncover how human brains can create any conscious sensation. This question – how and where our conscious feelings are generated – remains one of the great mysteries of science.
Derek Arnold, Professor, School of Psychology, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post





-

End the Insomnia Struggle – by Dr. Colleen Ehrnstrom and Dr. Alisha Brosse
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve reviewed sleep books before, and we always try to recommend books that have something a little different than the rest, so what makes this one stand out?
While there is the usual quick overview of the basics that we’re sure you already know (sleep hygiene etc), most of the attention here is given to cold, hard clinical psychology… in a highly personalized way.
How, you may ask, can they personalize a book, that is the same for everyone?
The answer is, by guiding the reader through examining our own situation. With template logbooks, worksheets, and the like—for this reason we recommend getting a paper copy of the book, rather than the Kindle version, in case you’d like to use/photocopy those.
Essentially, reading this book is much like having your own psychologist (or two) to guide you through finding a path to better sleep.
The therapeutic approach, by the way, is a combination of Cognitive Behavioral Therapy (CBT) and Acceptance-Commitment Therapy (ACT), which work very well together here.
Bottom line: if you’ve changed your bedsheets and turned off your electronic devices and need something a little more, this book is the psychological “big guns” for removing the barriers between you and good sleep.
Click here to check out End the Insomnia Struggle, and end yours once and for all!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Toothpastes & Mouthwashes: Which Help And Which Harm?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Toothpastes and mouthwashes: which kinds help, and which kinds harm?
You almost certainly brush your teeth. You might use mouthwash. A lot of people floss for three weeks at a time, often in January.
There are a lot of options for oral hygiene; variations of the above, and many alternatives too. This is a big topic, so rather than try to squeeze it all in one, this will be a several-part series.
For today, let’s look at toothpastes and mouthwashes, to start!
Toothpaste options
Toothpastes may contain one, some, or all of the following, so here are some notes on those:
Fluoride
Most toothpastes contain fluoride; this is generally recognized as safe though is not without its controversies. The fluoride content is the reason it’s recommended not to swallow toothpaste, though.
The fluoride in toothpaste can cause some small problems if overused; if you see unusually white patches on your teeth (your teeth are supposed to be ivory-colored, not truly white), that is probably a case of localized overcalcification because of the fluoride, and yes, you can have too much of a good thing.
Overall, the benefits are considered to far outweigh the risks, though.
Baking soda
Whether by itself or as part of a toothpaste, baking soda is a safe and effective choice, not just for cosmetic purposes, but for boosting genuine oral hygiene too:
- Enhanced plaque removal to improve gingival health: 3-month randomized clinical study of the effects of baking soda toothpaste on plaque and gingivitis
- The effects of two baking-soda toothpastes in enhancing mechanical plaque removal and improving gingival health: A 6-month randomized clinical study
- The efficacy of baking soda dentifrice in controlling plaque and gingivitis: A systematic review
Activated charcoal
Activated charcoal is great at removing many chemicals from things it touches. That includes the kind you might see on your teeth in the form of stains.
A topical aside on safety: activated charcoal is a common ingredient in a lot of black-colored Halloween-themed foods and drinks around this time of year. Beware, if you ingest these, there’s a good chance of it also cleaning out any meds you are taking. Ask your pharmacist about your own personal meds, but meds that (ingested) activated charcoal will usually remove include:
- Oral HRT / contraceptives
- Antidepressants (many kinds)
- Heart medications (at least several major kinds)
Toothpaste, assuming you are spitting-not-swallowing, won’t remove your medications though. Nor, in case you were worrying, will it strip tooth enamel, even if you have extant tooth enamel erosion:
Source: Activated charcoal toothpastes do not increase erosive tooth wear
However, it’s of no special extra help when it comes to oral hygiene itself, just removing stains.
So, if you’d like to use it for cosmetic reasons, go right ahead. If not, no need.
Hydrogen peroxide
This is generally not a good idea, speaking for the health. For whitening, yes, it works. But for health, not so much:
To be clear, when they say “alter”, they mean “in a bad way”. It increases inflammation and tissue damage.
If buying commercially-available whitening toothpaste made with hydrogen peroxide, the academic answer is that it’s a lottery, because brands’ proprietorial compounding processes vary widely and constantly with little oversight and even less transparency:
Is whitening toothpaste safe for dental health?: RDA-PE method
Mouthwash options
In the case of fluoride and hydrogen peroxide, the same advice (for and against) goes as per toothpaste.
Alcohol
There has been some concern about the potential carcinogenic effect of alcohol-based mouthwashes. According to the best current science, this one’s not an easy yes-or-no, but rather:
- If there are no other cancer risk factors, it does not seem to increase cancer risk
- If there are other cancer risk factors, it does make the risk worse
Read more:
- Does the use of alcohol mouthwash increase the risk of developing oral cancer?
- Alcohol-based mouthwash as a risk factor of oral cancer: A systematic review
Non-Alcohol
Non-alcoholic mouthwashes are not without their concerns either. In this case, the potential problem is changing the oral microbiome (we are supposed to have one!), and specifically, that the spread of what it kills and what it doesn’t may result in an imbalance that causes a lowering of the pH of the mouth.
Put differently: it makes your saliva more acidic.
Needless to say, that can cause its own problems for teeth. The research on this is still emerging, with regard to whether the benefits outweigh the problems, but the fact that it has this effect seems to be a consensus. Here’s an example paper; there are others:
Effects of Chlorhexidine mouthwash on the oral microbiome
Flossing, scraping, and alternatives
These are important (and varied, and interesting) enough to merit their own main feature, rather than squeezing them in at the end.
So, watch this space for a main feature on these soon!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The Most Underrated Hip Mobility Exercise (Not Stretching)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cori Lefkowith, of “Redefining Strength” and “Strong At Every Age” fame, is back to help us keep our hips in good order:
These tips don’t lie
It’s less about stretching, and more about range of motion and “use it or lose it”:
- Full range of motion in lifting exercises enhances joint mobility and stability, whereas strengthening muscles through a limited range of motion (e.g., half squats) can cause tightness.
- Lifting through a larger range of motion may result in faster strength gains too, so that’s a bonus.
- Customize your range of motion based on your body type and capability, but do try for what you reasonably can—don’t give up!
- Lower weights and focus on deeper movements like split squats or single-leg squats, but work up slowly if you have any difficulties to start with.
- Using exercises like the Bulgarian split squat and deficit split squat can improve hip mobility and strength (you’ll really need to see the video for this one)
- Fully controlling the range of motion is key to progress, even if it means going lighter; prioritize mobility over brute strength. Strength is good, but mobility is even more critical.
- Adding instability, such as raising the front foot in lunges, challenges muscles and increases mobility. Obviously, please be safe while doing so, and slowly increase the range of motion while maintaining control, avoiding reliance on momentum.
- Final tip that most don’t consider: try starting exercises from the bottom position to ensure proper form and muscle engagement!
For more on each of these plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: