Why Is Pneumonia So Dangerous?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Pneumonia is a significant killer of people over the age of 65, with the risk increasing with age after that, rising very sharply around the age of 85.
Here’s why;
Take a deep breath…
Pneumonia is an infection of the alveoli (air sacs of the lungs that increase the surface area and allow the gas exchange that’s necessary for our respiration) that causes them to fill with fluid, disrupting the normal exchange of oxygen and carbon dioxide.
Now, pneumonia is most commonly caused by viruses or bacteria that enter your body through respiratory droplets or by touching your eyes, nose, or mouth after contacting a contaminated surface.
Fortunately, we (usually) have a functioning immune system, and if pathogens reach your alveoli, macrophages engulf them, and additional white blood cells trigger inflammation that helps fight the infection but also produces fluid.
Unfortunately, as we mentioned up top, fluid-filled alveoli make gas exchange difficult to say the least, causing carbon dioxide to build up, leading to rapid breathing, poor oxygenation (in turn causing most of the rest of the body’s processes to become impaired), and in some cases, an excessive, prolonged inflammatory response spreads beyond your lungs, leading to organ failure, shock, and death.
For this reason, once identified, it’s usually treated with antibiotics (which also carry big risks, but the numbers favor taking one’s chances with antibiotics rather than with untreated pneumonia).
- Things that worsen your risk: smoking impairs your cilia, while genetic disorders, autoimmune disorders, young age, older age, and viral pneumonia can all increase the risk of developing severe pneumonia or secondary bacterial infections.
- Things that reduce your risk: eating a nutritious diet, getting adequate sleep, exercising regularly, receiving recommended vaccinations, and washing your hands frequently all help reduce the risk of pneumonia and protect vulnerable people.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Pneumonia: Prevention Is Better Than Cure
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Guava vs Watermelon – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing guava to watermelon, we picked the guava.
Why?
There’s a big difference in nutritional density:
In terms of macros, guava has 11x the fiber for 2x the carbs and 5x the protein, winning this category easily.
In the category of vitamins, guava has more of vitamins A, B1, B2, B3, B5, B6, B7, B9, C, E and K, while watermelon is not higher in any vitamins, making this one a complete win for guava.
Looking at minerals next, guava has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while watermelon is not higher in any minerals; a total win for guava once again.
In other considerations, guava is higher in polyphenols, but watermelon is an excellent source of lycopene (better than tomatoes, even), so this round’s a respectable tie.
Adding up the sections makes for a clear overall win for guava, but by all means enjoy either or both, as diversity is great, and also, while watermelon is indeed mostly water, that water is absorbed a lot better than just drinking it, so there’s a benefit there, too!
Want to learn more?
You might like:
Lycopene’s Benefits For The Gut, Heart, Brain, & More
Enjoy!
Share This Post
-

Gravitas – by Caroline Goyder
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A no-nonsense guide to (more than!) public speaking that isn’t just “tell jokes in your speech and imagine the audience naked”.
Because this isn’t just about speech-writing or speech delivery, so much as giving you important life skills. The kind that weren’t taught in school, but that nevertheless make a huge impact on success… whether you’re giving a presentation or hosting a party or negotiating a deal or just attending a social event. Or making a phonecall, even.
Whereas a lot of books of this kind treat “the audience” as a nebulous and purely responsive passive crowd of extras, Goyder does better. People are individuals, even if they’re all facing the same way for a moment. She works with that! She also teaches how to deal with not just hecklers, but also simply those people who sap your confidence and find fault with you and anything you do or say.b
Bottom line is: if you for whatever reason communicate with people, and would like them to think better of you, this is the book for you.
Share This Post
-
3 drugs that went from legal, to illegal, then back again
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cannabis, cocaine and heroin have interesting life stories and long rap sheets. We might know them today as illicit drugs, but each was once legal.
Then things changed. Racism and politics played a part in how we viewed them. We also learned more about their impact on health. Over time, they were declared illegal.
But decades later, these drugs and their derivatives are being used legally, for medical purposes.
Here’s how we ended up outlawing cannabis, cocaine and heroin, and what happened next.

Peruvian Syrup, containing cocaine, was used to ‘cure’ a range of diseases. Smithsonian Museum of American History/Flickr Cannabis, religion and racism
Cannabis plants originated in central Asia, spread to North Africa, and then to the Americas. People grew cannabis for its hemp fibre, used to make ropes and sacks. But it also had other properties. Like many other ancient medical discoveries, it all started with religion.
Cannabis is mentioned in the Hindu texts known as the Vedas (1700-1100 BCE) as a sacred, feel-good plant. Cannabis or bhang is still used ritually in India today during festivals such as Shivratri and Holi.
From the late 1700s, the British in India started taxing cannabis products. They also noticed a high rate of “Indian hemp insanity” – including what we’d now recognise as psychosis – in the colony. By the late 1800s, a British government investigation found only heavy cannabis use seemed to affect people’s mental health.
This drug bottle from the United States contains cannabis tincture. Wikimedia In the 1880s, cannabis was used therapeutically in the United States to treat tetanus, migraine and “insane delirium”. But not everyone agreed on (or even knew) the best dose. Local producers simply mixed up what they had into a tincture – soaking cannabis leaves and buds in alcohol to extract essential oils – and hoped for the best.
So how did cannabis go from a slightly useless legal drug to a social menace?
Some of it was from genuine health concerns about what was added to people’s food, drink and medicine.
In 1908 in Australia, New South Wales listed cannabis as an ingredient that could “adulterate” food and drink (along with opium, cocaine and chloroform). To sell the product legally, you had to tell the customers it contained cannabis.
Some of it was international politics. Moves to control cannabis use began in 1912 with the world’s first treaty against drug trafficking. The US and Italy both wanted cannabis included, but this didn’t happen until until 1925.
Some of it was racism. The word marihuana is Spanish for cannabis (later Anglicised to marijuana) and the drug became associated with poor migrants. In 1915, El Paso, Texas, on the Mexican border, was the first US municipality to ban the non-medical cannabis trade.
By the late 1930s, cannabis was firmly entrenched as a public menace and drug laws had been introduced across much of the US, Europe and (less quickly) Australia to prohibit its use. Cannabis was now a “poison” regulated alongside cocaine and opiates.
The 1936 movie Reefer Madness fuelled cannabis paranoia. Motion Picture Ventures/Wikimedia Commons The 1936 movie Reefer Madness was a high point of cannabis paranoia. Cannabis smoking was also part of other “suspect” new subcultures such as Black jazz, the 1950s Beatnik movement and US service personnel returning from Vietnam.
Today recreational cannabis use is associated with physical and mental harm. In the short term, it impairs your functioning, including your ability to learn, drive and pay attention. In the long term, harms include increasing the risk of psychosis.
But what about cannabis as a medicine? Since the 1980s there has been a change in mood towards experimenting with cannabis as a therapeutic drug. Medicinal cannabis products are those that contain cannabidiol (CBD) or tetrahydrocannabinol (THC). Today in Australia and some other countries, these can be prescribed by certain doctors to treat conditions when other medicines do not work.
Medicinal cannabis has been touted as a treatment for some chronic conditions such as cancer pain and multiple sclerosis. But it’s not clear yet whether it’s effective for the range of chronic diseases it’s prescribed for. However, it does seem to improve the quality of life for people with some serious or terminal illnesses who are using other prescription drugs.
Cocaine, tonics and addiction
Several different species of the coca plant grow across Bolivia, Peru and Colombia. For centuries, local people chewed coca leaves or made them into a mildly stimulant tea. Coca and ayahuasca (a plant-based psychedelic) were also possibly used to sedate people before Inca human sacrifice.
In 1860, German scientist Albert Niemann (1834-1861) isolated the alkaloid we now call “cocaine” from coca leaves. Niemann noticed that applying it to the tongue made it feel numb.
But because effective anaesthetics such as ether and nitrous oxide had already been discovered, cocaine was mostly used instead in tonics and patent medicines.
Hall’s Coca Wine was made from the leaves of the coca plant. Stephen Smith & Co/Wellcome Collection, CC BY Perhaps the most famous example was Coca-Cola, which contained cocaine when it was launched in 1886. But cocaine was used earlier, in 1860s Italy, in a drink called Vin Mariani – Pope Leo XIII was a fan.
With cocaine-based products easily available, it quickly became a drug of addiction.
Cocaine remained popular in the entertainment industry. Fictional detective Sherlock Holmes injected it, American actor Tallulah Bankhead swore by it, and novelist Agatha Christie used cocaine to kill off some of her characters.
In 1914, cocaine possession was made illegal in the US. After the hippy era of the 1960s and 1970s, cocaine became the “it” drug of the yuppie 1980s. “Crack” cocaine also destroyed mostly Black American urban communities.
Cocaine use is now associated with physical and mental harms. In the short and long term, it can cause problems with your heart and blood pressure and cause organ damage. At its worst, it can kill you. Right now, illegal cocaine production and use is also surging across the globe.
But cocaine was always legal for medical and surgical use, most commonly in the form of cocaine hydrochloride. As well as acting as a painkiller, it’s a vasoconstrictor – it tightens blood vessels and reduces bleeding. So it’s still used in some types of surgery.
Heroin, coughing and overdoses
Opium has been used for pain relief ever since people worked out how to harvest the sap of the opium poppy. By the 19th century, addictive and potentially lethal opium-based products such as laudanum were widely available across the United Kingdom, Europe and the US. Opium addiction was also a real problem.
Because of this, scientists were looking for safe and effective alternatives for pain relief and to help people cure their addictions.
In 1874, English chemist Charles Romley Alder Wright (1844-1894) created diacetylmorphine (also known as diamorphine). Drug firm Bayer thought it might be useful in cough medicines, gave it the brand name Heroin and put it on the market in 1898. It made chest infections worse.
Allenburys Throat Pastilles contained heroin and cocaine. Seth Anderson/Flickr, CC BY-NC Although diamorphine was created with good intentions, this opiate was highly addictive. Shortly after it came on the market, it became clear that it was every bit as addictive as other opiates. This coincided with international moves to shut down the trade in non-medical opiates due to their devastating effect on China and other Asian countries.
Like cannabis, heroin quickly developed radical chic. The mafia trafficked into the US and it became popular in the Harlem jazz scene, beatniks embraced it and US servicemen came back from Vietnam addicted to it. Heroin also helped kill US singers Janis Joplin and Jim Morrison.
Today, we know heroin use and addiction contributes to a range of physical and mental health problems, as well as death from overdose.
However, heroin-related harm is now being outpaced by powerful synthetic opioids such as oxycodone, fentanyl, and the nitazene group of drugs. In Australia, there were more deaths and hospital admissions from prescription opiate overdoses than from heroin overdoses.
In a nutshell
Not all medicines have a squeaky-clean history. And not all illicit drugs have always been illegal.
Drugs’ legal status and how they’re used are shaped by factors such as politics, racism and social norms of the day, as well as their impact on health.
Philippa Martyr, Lecturer, Pharmacology, Women’s Health, School of Biomedical Sciences, The University of Western Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post






Related Posts
-
A Surprisingly Accessible Treatment For Migraines
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
…and other items from this week’s health news:
Cannabis’s very good stats for migraine relief
Migraine attacks are thought by many people to be “just a bad headache”, but in fact, there’s a lot more to it than that, and they’re also famously resistant to a lot of usual headache-relief medications and other remedies.
So, what’s new? Researchers (Dr. Dawn Buse et al.) tested cannabis vs placebo for the treatment of migraine, and got great results:
How it worked: 92 participants used vaporized cannabis containing 6% tetrahydrocannabinol (THC) and 11% cannabidiol (CBD), which are considdered relatively low potencies.
And the results?
- 67% of participants experienced a reduction in migraine pain within two hours of treatment
- 35% of participants became completely pain-free after treatment
These benefits lasted for up to 48 hours across 247 treated migraine attacks, and in terms of safety, no serious adverse events were reported during the study.
Read in full: Cannabis shows anti-migraine benefits
Related: Migraine: When Headaches Are The Tip Of The Neurological Iceberg
Alcohol use disorder: what are the key factors affecting relapse?
Long-term relapse in alcohol use disorder was most strongly linked to a gradual reduction in recovery focus or vigilance, making it the most prevalent and potent risk factor. As for what this looked like, it often involved deprioritizing recovery-related attitudes and routines, alongside disengagement from mutual-help groups and other recovery supports.
In other words, rather than a sudden failure as such relapses are generally assumed to be, it was usually more of a slow erosion of commitment to ongoing recovery maintenance.
That, perhaps, explains why psychological and social factors also play a major role, particularly worsening mental health symptoms, loneliness, social isolation, and increased exposure to alcohol-related environments, generally increasing in the year leading up to relapse:
Read in full: Key risk factors identified for long-term relapse in alcohol use disorder
Related: Which Addiction-Quitting Methods Work Best?
Not “basically just steam” after all
Vapes have enjoyed a (so far, it seems, well-earned) reputation of being less harmful than cigarettes. One of the ways in which they are considered less bad healthwise is when it comes to passive consumption, i.e., second-hand smoke/vapour. In the case of smoke, it’s smoke, and whatever else is in it, everyone knows smoke is bad to inhale, right? Whereas vapour… Steam inhalation is good for the health, no?
And in this case: no
As it turns out, secondhand vape plumes can contain ultrafine particles loaded with metals and reactive peroxides that interact to form lung-damaging free radicals. Additionally, volatile organic compounds in vape vapor can react with indoor ozone to form peroxides, which then interact with metals to generate reactive radicals.
It gets worse: because ultrafine particles can penetrate deep into your lungs and reach fluid-lined alveoli, they may damage lung tissue and impair lower respiratory function. And, paradoxically, ultrafine particles carry higher proportions of metals and peroxides than larger particles.
Read in full: Secondhand vape plumes could form lung-damaging radicals
Related: Vaping: A Lot Of Hot Air?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

A person in Texas caught bird flu after mixing with dairy cattle. Should we be worried?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The United States’ Centers for Disease Control and Prevention (CDC) has issued a health alert after the first case of H5N1 avian influenza, or bird flu, seemingly spread from a cow to a human.
A farm worker in Texas contracted the virus amid an outbreak in dairy cattle. This is the second human case in the US; a poultry worker tested positive in Colorado in 2022.
The virus strain identified in the Texan farm worker is not readily transmissible between humans and therefore not a pandemic threat. But it’s a significant development nonetheless.
Some background on bird flu
There are two types of avian influenza: highly pathogenic or low pathogenic, based on the level of disease the strain causes in birds. H5N1 is a highly pathogenic avian influenza.
H5N1 first emerged in 1997 in Hong Kong and then China in 2003, spreading through wild bird migration and poultry trading. It has caused periodic epidemics in poultry farms, with occasional human cases.
Influenza A viruses such as H5N1 are further divided into variants, called clades. The unique variant causing the current epidemic is H5N1 clade 2.3.4.4b, which emerged in late 2020 and is now widespread globally, especially in the Americas.
In the past, outbreaks could be controlled by culling of infected birds, and H5N1 would die down for a while. But this has become increasingly difficult due to escalating outbreaks since 2021.
Wild animals are now in the mix
Waterfowl (ducks, swans and geese) are the main global spreaders of avian flu, as they migrate across the world via specific routes that bypass Australia. The main hub for waterfowl to migrate around the world is Quinghai lake in China.
But there’s been an increasing number of infected non-waterfowl birds, such as true thrushes and raptors, which use different flyways. Worryingly, the infection has spread to Antarctica too, which means Australia is now at risk from different bird species which fly here.
H5N1 has escalated in an unprecedented fashion since 2021, and an increasing number of mammals including sea lions, goats, red foxes, coyotes, even domestic dogs and cats have become infected around the world.
Wild animals like red foxes which live in peri-urban areas are a possible new route of spread to farms, domestic pets and humans.
Dairy cows and goats have now become infected with H5N1 in at least 17 farms across seven US states.
What are the symptoms?
Globally, there have been 14 cases of H5N1 clade 2.3.4.4b virus in humans, and 889 H5N1 human cases overall since 2003.
Previous human cases have presented with a severe respiratory illness, but H5N1 2.3.4.4b is causing illness affecting other organs too, like the brain, eyes and liver.
For example, more recent cases have developed neurological complications including seizures, organ failure and stroke. It’s been estimated that around half of people infected with H5N1 will die.
The case in the Texan farm worker appears to be mild. This person presented with conjunctivitis, which is unusual.
Food safety
Contact with sick poultry is a key risk factor for human infection. Likewise, the farm worker in Texas was likely in close contact with the infected cattle.
The CDC advises pasteurised milk and well cooked eggs are safe. However, handling of infected meat or eggs in the process of cooking, or drinking unpasteurised milk, may pose a risk.
Although there’s no H5N1 in Australian poultry or cattle, hygienic food practices are always a good idea, as raw milk or poorly cooked meat, eggs or poultry can be contaminated with microbes such as salmonella and E Coli.
If it’s not a pandemic, why are we worried?
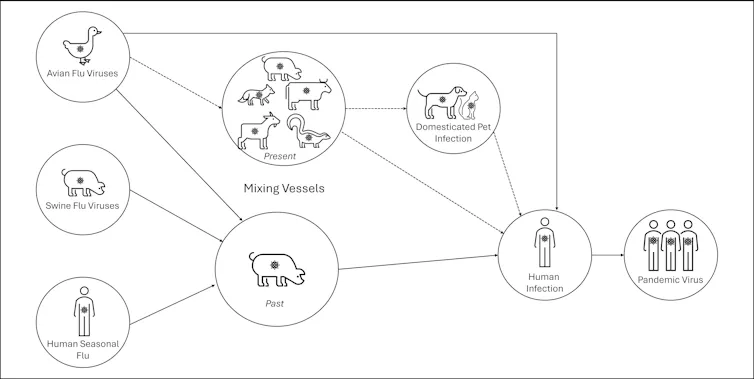
Scientists have feared avian influenza may cause a pandemic since about 2005. Avian flu viruses don’t easily spread in humans. But if an avian virus mutates to spread in humans, it can cause a pandemic.
One concern is if birds were to infect an animal like a pig, this acts as a genetic mixing vessel. In areas where humans and livestock exist in close proximity, for example farms, markets or even in homes with backyard poultry, the probability of bird and human flu strains mixing and mutating to cause a new pandemic strain is higher.
There are a number of potential pathways to a pandemic caused by influenza. Author provided The cows infected in Texas were tested because farmers noticed they were producing less milk. If beef cattle are similarly affected, it may not be as easily identified, and the economic loss to farmers may be a disincentive to test or report infections.
How can we prevent a pandemic?
For now there is no spread of H5N1 between humans, so there’s no immediate risk of a pandemic.
However, we now have unprecedented and persistent infection with H5N1 clade 2.3.4.4b in farms, wild animals and a wider range of wild birds than ever before, creating more chances for H5N1 to mutate and cause a pandemic.
Unlike the previous epidemiology of avian flu, where hot spots were in Asia, the new hot spots (and likely sites of emergence of a pandemic) are in the Americas, Europe or in Africa.
Pandemics grow exponentially, so early warnings for animal and human outbreaks are crucial. We can monitor infections using surveillance tools such as our EPIWATCH platform.
The earlier epidemics can be detected, the better the chance of stamping them out and rapidly developing vaccines.
Although there is a vaccine for birds, it has been largely avoided until recently because it’s only partially effective and can mask outbreaks. But it’s no longer feasible to control an outbreak by culling infected birds, so some countries like France began vaccinating poultry in 2023.
For humans, seasonal flu vaccines may provide a small amount of cross-protection, but for the best protection, vaccines need to be matched exactly to the pandemic strain, and this takes time. The 2009 flu pandemic started in May in Australia, but the vaccines were available in September, after the pandemic peak.
To reduce the risk of a pandemic, we must identify how H5N1 is spreading to so many mammalian species, what new wild bird pathways pose a risk, and monitor for early signs of outbreaks and illness in animals, birds and humans. Economic compensation for farmers is also crucial to ensure we detect all outbreaks and avoid compromising the food supply.
C Raina MacIntyre, Professor of Global Biosecurity, NHMRC L3 Research Fellow, Head, Biosecurity Program, Kirby Institute, UNSW Sydney; Ashley Quigley, Senior Research Associate, Global Biosecurity, UNSW Sydney; Haley Stone, PhD Candidate, Biosecurity Program, Kirby Institute, UNSW Sydney; Matthew Scotch, Associate Dean of Research and Professor of Biomedical Informatics, College of Health Solutions, Arizona State University, and Rebecca Dawson, Research Associate, The Kirby Institute, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
5 Things You Can Change About Your Personality (But: Should You?)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are many personality-typing systems that, with varying degrees of validity*, aim to describe a person’s personality.
*and often pseudoscience:
- sometimes obviously so like astrology
- sometimes dressed up in clinical words like the Meyers-Briggs
- sometimes openly, per “this is not science but you may find it useful to frame things this way”, like the Enneagram
There is currently one kind of personality-typing system (with some minor variations) that is used in the actual field of clinical psychology, specifically under the umbrella of “trait theory”, and that is…
The “Big Five” personality traits
Also called the OCEAN or CANOE model, based on its 5 components:
- openness to experience: inventive/curious rather than consistent/cautious
- conscientiousness: efficient/organized rather than extravagant/careless
- extroversion: outgoing/energetic rather than solitary/reserved
- agreeableness: friendly/compassionate rather than critical/judgmental
- neuroticism: sensitive/nervous rather than resilient/confident
The latter (neuroticism) is not to be confused with neurosis, which is very different and beyond the scope of today’s article.
Note that some of these seem more positive/negative than others at a glance, but really, any of these could be a virtue or a vice depending on specifics or extremity.
For scientific reference, here’s an example paper:
The Big Five Personality Factors and Personal Values
Quick self-assessment
There are of course many lengthy questionnaires for this, but in the interests of expediency:
Take a moment to rate yourself as honestly as you can, on a scale of 1–10, for each of those components, with 10 being highest for the named trait.
For example, this writer gives herself: O7, C6, E3, A8, N2 (in other words I’d say I’m fairly open, moderately conscientious, on the reserved side, quite agreeable, and quite resilient)
Now, put your rating aside (in your phone’s notes app is fine, if you hadn’t written it down already) and forget about it for the moment, because we want you to do the next exercise from scratch.
Who would you be, at your best?
Now imagine your perfect idealized self, the best you could ever be, with no constraints.
Take a moment to rate your idealized self’s personality, on a scale of 1–10, for each of those components, with 10 being highest for the named trait.
For example, this writer picks: O9, C10, E5, A8, N1.
Maybe this, or maybe your own idealized self’s personality, will surprise you. That some traits might already be perfect for you already; others might just be nudged a little here or there; maybe there’s some big change you’d like. Chances are you didn’t go for a string of 10s or 1s (though if you did, you do you; there are no wrong answers here as this one is about your preferences).
We become who we practice being
There are some aspects of personality that can naturally change with age. For example:
- confidence/resilience will usually gradually increase with age due to life experience (politely overlook teenagers’ bravado; they are usually a bundle of nerves inside, resulting in the overcompensatory displays of confidence)
- openness to experience may decrease with age, as we can get into a rut of thinking/acting a certain way, and/or simply consciously decide that our position on something is already complete and does not need revision.
But, we can decide for ourselves how to nudge our “Big Five” traits, for example:
- We can make a point of seeking out new experiences, and considering new ideas, or develop strategies for reining ourselves in
- We can use systems to improve our organization, or go out of our way to introduce a little well-placed chaos
- We can “put ourselves out there” socially, or make the decision to decline more social invitations because we simply don’t want to
- We can make a habit of thinking kindly of others and ourselves, or we can consciously detach ourselves and look on the cynical side more
- We can build on our strengths and eliminate our weaknesses, or lean into uncomfortable emotions
Some of those may provoke a “why would anyone want to…?” response, but the truth is we are all different. An artist and a police officer may have very different goals for who they want to be as a person, for example.
Interventions to change personality can and do work:
A systematic review of personality trait change through intervention
There are many ways to go about “being the change we want to see” in ourselves, and yes there can be a degree of “fake it until you make it” if that works for you, but it doesn’t have to be so. It can also simply be a matter of setting yourself reminders about the things that are most important to you.
Writer’s example: pinned above my digital workspace I have a note from my late beloved, written just under a week before death. The final line reads, “keep being the good person that you are” (on a human level, the whole note is uplifting and soothing to me and makes me smile and remember the love we shared; or to put it in clinical terms, it promotes high agreeableness, low neuroticism).
Other examples could be a daily practice of gratitude (promotes lower neuroticism), or going out of your way to speak to your neighbors (promotes higher extraversion), signing up for a new educational course (promotes higher openness) or downloading a budgeting app (promotes higher conscientiousness).
In short: be the person you want to be, and be that person deliberately, because you can.
Some resources that may help for each of the 5 traits:
- Curiosity Kills The Neurodegeneration
- How (And Why) To Train Your Pre-Frontal Cortex
- How To Beat Loneliness & Isolation
- Optimism Seriously Increases Longevity!
- Building Psychological Resilience (Without Undue Hardship)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: