Migraine Mythbusting
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Migraine: When Headaches Are The Tip Of The Neurological Iceberg
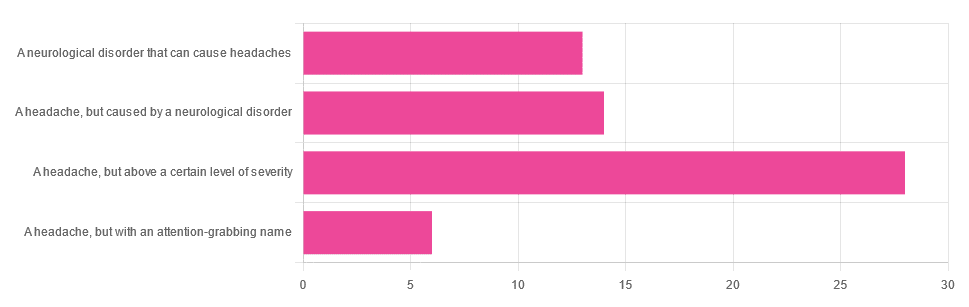
Yesterday, we asked you “What is a migraine?” and got the above-depicted, below-described spread of responses:
- Just under 46% said “a headache, but above a certain level of severity”
- Just under 23% said “a headache, but caused by a neurological disorder”
- Just over 21% said “a neurological disorder that can cause headaches”
- Just under 10% said “a headache, but with an attention-grabbing name”
So… What does the science say?
A migraine is a headache, but above a certain level of severity: True or False?
While that’s usually a very noticeable part of it… That’s only one part of it, and not a required diagnostic criterion. So, in terms of defining what a migraine is, False.
Indeed, migraine may occur without any headache, let alone a severe one, for example: Abdominal Migraine—though this is much less well-researched than the more common with-headache varieties.
Here are the defining characteristics of a migraine, with the handy mnemonic 5-4-3-2-1:
- 5 or more attacks
- 4 hours to 3 days in duration
- 2 or more of the following:
- Unilateral (affects only one side of the head)
- Pulsating
- Moderate or severe pain intensity
- Worsened by or causing avoidance of routine physical activity
- 1 or more of the following:
- Nausea and/or vomiting
- Sensitivity to both light and sound
Source: Cephalalgia | ICHD-II Classification: Parts 1–3: Primary, Secondary and Other
As one of our subscribers wrote:
❝I have chronic migraine, and it is NOT fun. It takes away from my enjoyment of family activities, time with friends, and even enjoying alone time. Anyone who says a migraine is just a bad headache has not had to deal with vertigo, nausea, loss of balance, photophobia, light sensitivity, or a host of other symptoms.❞
Migraine is a neurological disorder: True or False?
True! While the underlying causes aren’t known, what is known is that there are genetic and neurological factors at play.
❝Migraine is a recurrent, disabling neurological disorder. The World Health Organization ranks migraine as the most prevalent, disabling, long-term neurological condition when taking into account years lost due to disability.
Considerable progress has been made in elucidating the pathophysiological mechanisms of migraine, associated genetic factors that may influence susceptibility to the disease❞
Source: JHP | Mechanisms of migraine as a chronic evolutive condition
Migraine is just a headache with a more attention-grabbing name: True or False?
Clearly, False.
As we’ve already covered why above, we’ll just close today with a nod to an old joke amongst people with chronic illnesses in general:
“Are you just saying that because you want attention?”
“Yes… Medical attention!”
Want to learn more?
You can find a lot of resources at…
NIH | National Institute of Neurological Disorders & Stroke | Migraine
and…
The Migraine Trust ← helpfully, this one has a “Calm mode” to tone down the colorscheme of the website!
Particularly useful from the above site are its pages:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:

How to Do the Work – by Dr. Nicole LaPera

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We have reviewed some self-therapy books before, and they chiefly have focused on CBT and mindfulness, which are great. This one’s different.
Dr. Nicole LaPera has a bolder vision for what we can do for ourselves. Rather than giving us some worksheets for unraveling cognitive distortions or clearing up automatic negative thoughts, she bids us treat the cause, rather than the symptom.
For most of us, this will be the life we have led. Now, we cannot change the parenting style(s) we received (or didn’t), get a redo on childhood, avoid mistakes we made in our adolescence, or face adult life with the benefit of experience we gained right after we needed it most. But we can still work on those things if we just know how.
The subtitle of this book promsies that the reader can/will “recognise your patterns, heal from your past, and create your self”.
That’s accurate, for the content of the book and the advice it gives.
Dr. LaPera’s focus is on being our own best healer, and reparenting our own inner child. Giving each of us the confidence in ourself; the love and care and/but also firm-if-necessary direction that a (good) parent gives a child, and the trust that a secure child will have in the parent looking after them. Doing this for ourselves, Dr. LaPera holds, allows us to heal from traumas we went through when we perhaps didn’t quite have that, and show up for ourselves in a way that we might not have thought about before.
If the book has a weak point, it’s that many of the examples given are from Dr. LaPera’s own life and experience, so how relatable the specific examples will be to any given reader may vary. But, the principles and advices stand the same regardless.
Bottom line: if you’d like to try self-therapy on a deeper level than CBT worksheets, this book is an excellent primer.
Click here to check out How To Do The Work, and empower yourself to indeed do the work!
Share This Post

Eat Well With Arthritis – by Emily Johnson, with Dr. Deepak Ravindran
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Author Emily Johnson was diagnosed with arthritis in her early 20s, but it had been affecting her life since the age of 4. Suffice it to say, managing the condition has been integral to her life.
She’s written this book with not only her own accumulated knowledge, but also the input of professional experts; the book contains insights from chronic pain specialist Dr. Deepak Ravindran, and gets an additional medical thumbs-up in a foreword by rheumatologist Dr. Lauren Freid.
The recipes themselves are clear and easy, and the ingredients are not obscure. There’s information on what makes each dish anti-inflammatory, per ingredient, so if you have cause to make any substitutions, that’s useful to know.
Speaking of ingredients, the recipes are mostly plant-based (though there are some chicken/fish ones) and free from common allergens—but not all of them are, so each of those is marked appropriately.
Beyond the recipes, there are also sections on managing arthritis more generally, and information on things to get for your kitchen that can make your life with arthritis a lot easier!
Bottom line: if you have arthritis, cook for somebody with arthritis, or would just like a low-inflammation diet, then this is an excellent book for you.
Share This Post

Laziness Does Not Exist – by Dr. Devon Price
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Some cultures prize productivity as an ideal above most other things, and it’s certainly so in the US. Not only is this not great for mental health in general, but also—as Dr. Price explains—it’s based on a lie.
Generally speaking, when a person appears lazy there is something stopping them/you from doing better, and it’s not some mystical unseen force of laziness, not a set character trait, not a moral failing. Rather, the root cause may be physical, psychological, socioeconomic, or something else entirely.
Those causes can in some cases be overcome (for example, a little CBT can often set aside perfectionist anxiety that results in procrastination), and in some cases they can’t, at least on an individual level (disabilities often stubbornly remain disabling, and societal problems require societal solutions).
This matters for our mental health in areas well beyond the labor marketplace, of course, and these ideas extend to personal projects and even personal relationships. Whatever it is, if it’s leaving you exhausted, then probably something needs to be changed (even if the something is just “expectations”).
The book does offer practical solutions to all manner of such situations, improving what can be improved, making easier what can be made easier, and accepting what just needs to be accepted.
The style of this book is casual yet insightful and deep, easy-reading yet with all the acumen of an accomplished social psychologist.
Bottom line: if life leaves you exhausted, this book can be the antidote and cure
Click here to check out Laziness Does Not Exist, and break free!
Share This Post
Related Posts

What’s Your Personal Life Expectancy?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Tick Tock… Goes the Death Clock?
This fun little test will ask a few questions about you and your lifestyle, and then make a prediction of your personal life expectancy, based on global statistics from the World Health Organisation.
And then the countdown starts… Literally, it generates a clock for you to see your life-seconds ticking away—this may or may not delight you, but it sure is a curiosity.
Their “Letters” page has a lot of reactions from people who just got their results (spoiler: people’s perspectives on life vary a lot)
Who mostly uses this service? According to their stats page, it’s mostly curious under-45s, with gradually less interest in knowing about it from 45 onwards… until the age of 70, when suddenly everyone wants to know about it again!
So Is It Possible To Pause The Clock On Aging? – Q&A Spotlight Interview
Life extension is sometimes viewed as the domain of the super-rich, and with less than half of Millennials (and almost none of Gen-Z) having retirement plans, often those of us who aren’t super-rich have more mundane (and immediate!) goals than living to 120.
And yet…
Middle class and working class life-extensionists do exist, even if not garnering the same media attention. We think that’s strange—after all, while the whimsies of the super-rich may be entertaining to read about, it’s not nearly as applicable to most people as more relatable stories:
- The twenty-something who gives up smoking and adds (healthier!) years to their life
- The thirty-something who adopts a plant-based diet and is less likely to die of heart disease
- The forty-something who stops drinking, and avoids health conditions and mishaps alike
- The fifty-something who reconsiders their health plan in light of their changing body
- The sixty-something who takes up yoga, or chess, or salsa dancing
- The seventy-something who gets asked what their secret is
- …and so on
But these are ideas, textbook examples. What if we make it more personal?
We interviewed 10 Almonds subscriber and longevity enthusiast Anastasia S., and here’s what she had to say:
Q: What does life extension mean to you, in your life?
A: To me, the key is healthy life extension. People often joke “I don’t want to live longer; the last years are the worst!” but they’re missing the point that after a certain age, those difficulties are coming whether they come at 50 or 70 or 90. Personally, I’d rather keep them at bay if I can.
Q: How do you do that?
A: Firstly, which won’t be a shock: good diet and exercise. Those two things are possibly the biggest active influences on my longevity. I’m vegan, which I don’t think is outright necessary for good health but done right, it can certainly be good. In this house we eat a lot of whole grains, beans, lentils, vegetables in general, nuts too. As for exercise, I do 30–60 minutes of Pilates daily; it’s nothing fancy and it’s just me in my pajamas at home, but it keeps me strong and fit and supple. I also walk everywhere; I don’t even own a car. Beyond that… I don’t drink or smoke (probably the biggest passive influences on my longevity, i.e., things that aren’t there to make it shorter), and I try to take my sleep seriously, making sure to schedule enough time and prepare properly for it.
Q: Take your sleep seriously? How so?
A: Good “sleep hygiene” as some call it—I schedule a little wind-down time before sleep, with no glaring screens or main lights, making a space between my busy day and restful sleep, kicking anything requiring brainpower to the morning, and making a conscious choice not to think more about those things in the meantime. I take care to make my sleeping environment as conducive as possible to good sleep too; I have a good mattress and pillows, I make sure the temperature is cool but cosy. I have a pot of herbal tea on my bedside table—I hydrate a lot.
Q: Do you take any supplements?
A: I do! They’re mostly quite general though, just “covering my bases”, so to speak. I take a daily nootropic stack (a collection of supplements specifically for brain health), too. I buy them in bulk, so they don’t cost so much.
Q: This seems quite a healthy lifestyle! Do you have any vices at all?
A: I definitely drink more coffee than I probably should! But hey, nobody’s perfect. I do love coffee, though, and as vices go, it’s probably not too bad.
Q: How’s it all working out for you? Do you feel younger?
A: I’m 38 and sometimes I feel like a teenager; sometimes I feel like an old lady. But the latter is usually for social reasons, not health-related reasons. I do have streaks of gray in my hair though, and I love that! If people don’t notice my grays, then they often think I’m in my 20s, rather than pushing 40. A little while back, I was stopped in the street by someone wanting to sell me a change of household utilities provider, then she stopped herself mid-sentence and said “Oh but wait, you look a bit too young, never mind”. Most general metrics of health would put me in my 20s.
Q: That’s interesting that you love your gray hairs, for someone who wants to stay young; is it an exception?
A: It’s more that I want to minimize the problems that come with age, and not everything’s a problem. Gray hairs are cool; joint pain, not so much. A long life rich with experiences is cool; memory loss, not so much. So, I try to keep healthy, and wear my years as best I can.
Q: Sounds good to us; good luck with it!
A: Thank you; I do my best!
Here at 10 Almonds, we love featuring what our readers are doing to improve their health; if you’re willing to be featured in our newsletter, let us know by replying to this email (where an actual human will read it, we promise!)
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:

Think you’re good at multi-tasking? Here’s how your brain compensates – and how this changes with age
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’re all time-poor, so multi-tasking is seen as a necessity of modern living. We answer work emails while watching TV, make shopping lists in meetings and listen to podcasts when doing the dishes. We attempt to split our attention countless times a day when juggling both mundane and important tasks.
But doing two things at the same time isn’t always as productive or safe as focusing on one thing at a time.
The dilemma with multi-tasking is that when tasks become complex or energy-demanding, like driving a car while talking on the phone, our performance often drops on one or both.
Here’s why – and how our ability to multi-task changes as we age.
Doing more things, but less effectively
The issue with multi-tasking at a brain level, is that two tasks performed at the same time often compete for common neural pathways – like two intersecting streams of traffic on a road.
In particular, the brain’s planning centres in the frontal cortex (and connections to parieto-cerebellar system, among others) are needed for both motor and cognitive tasks. The more tasks rely on the same sensory system, like vision, the greater the interference.
This is why multi-tasking, such as talking on the phone, while driving can be risky. It takes longer to react to critical events, such as a car braking suddenly, and you have a higher risk of missing critical signals, such as a red light.
The more involved the phone conversation, the higher the accident risk, even when talking “hands-free”.
Generally, the more skilled you are on a primary motor task, the better able you are to juggle another task at the same time. Skilled surgeons, for example, can multitask more effectively than residents, which is reassuring in a busy operating suite.
Highly automated skills and efficient brain processes mean greater flexibility when multi-tasking.
Adults are better at multi-tasking than kids
Both brain capacity and experience endow adults with a greater capacity for multi-tasking compared with children.
You may have noticed that when you start thinking about a problem, you walk more slowly, and sometimes to a standstill if deep in thought. The ability to walk and think at the same time gets better over childhood and adolescence, as do other types of multi-tasking.
When children do these two things at once, their walking speed and smoothness both wane, particularly when also doing a memory task (like recalling a sequence of numbers), verbal fluency task (like naming animals) or a fine-motor task (like buttoning up a shirt). Alternately, outside the lab, the cognitive task might fall by wayside as the motor goal takes precedence.
Brain maturation has a lot to do with these age differences. A larger prefrontal cortex helps share cognitive resources between tasks, thereby reducing the costs. This means better capacity to maintain performance at or near single-task levels.
The white matter tract that connects our two hemispheres (the corpus callosum) also takes a long time to fully mature, placing limits on how well children can walk around and do manual tasks (like texting on a phone) together.
For a child or adult with motor skill difficulties, or developmental coordination disorder, multi-tastking errors are more common. Simply standing still while solving a visual task (like judging which of two lines is longer) is hard. When walking, it takes much longer to complete a path if it also involves cognitive effort along the way. So you can imagine how difficult walking to school could be.
What about as we approach older age?
Older adults are more prone to multi-tasking errors. When walking, for example, adding another task generally means older adults walk much slower and with less fluid movement than younger adults.
These age differences are even more pronounced when obstacles must be avoided or the path is winding or uneven.
Older adults tend to enlist more of their prefrontal cortex when walking and, especially, when multi-tasking. This creates more interference when the same brain networks are also enlisted to perform a cognitive task.
These age differences in performance of multi-tasking might be more “compensatory” than anything else, allowing older adults more time and safety when negotiating events around them.
Older people can practise and improve
Testing multi-tasking capabilities can tell clinicians about an older patient’s risk of future falls better than an assessment of walking alone, even for healthy people living in the community.
Testing can be as simple as asking someone to walk a path while either mentally subtracting by sevens, carrying a cup and saucer, or balancing a ball on a tray.
Patients can then practise and improve these abilities by, for example, pedalling an exercise bike or walking on a treadmill while composing a poem, making a shopping list, or playing a word game.
The goal is for patients to be able to divide their attention more efficiently across two tasks and to ignore distractions, improving speed and balance.
There are times when we do think better when moving
Let’s not forget that a good walk can help unclutter our mind and promote creative thought. And, some research shows walking can improve our ability to search and respond to visual events in the environment.
But often, it’s better to focus on one thing at a time
We often overlook the emotional and energy costs of multi-tasking when time-pressured. In many areas of life – home, work and school – we think it will save us time and energy. But the reality can be different.
Multi-tasking can sometimes sap our reserves and create stress, raising our cortisol levels, especially when we’re time-pressured. If such performance is sustained over long periods, it can leave you feeling fatigued or just plain empty.
Deep thinking is energy demanding by itself and so caution is sometimes warranted when acting at the same time – such as being immersed in deep thought while crossing a busy road, descending steep stairs, using power tools, or climbing a ladder.
So, pick a good time to ask someone a vexed question – perhaps not while they’re cutting vegetables with a sharp knife. Sometimes, it’s better to focus on one thing at a time.

Peter Wilson, Professor of Developmental Psychology, Australian Catholic University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:

Blood-Brain Barrier Breach Blamed For Brain-Fog
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Move Over, Leaky Gut. Now It’s A Leaky Brain.
…which is not a headline that promises good news, and indeed, the only good news about this currently is “now we know another thing that’s happening, and thus can work towards a treatment for it”.
Back in February (most popular media outlets did not rush to publish this, as it rather goes against the narrative of “remember when COVID was a thing?” as though the numbers haven’t risen since the state of emergency was declared over), a team of Irish researchers made a discovery:
❝For the first time, we have been able to show that leaky blood vessels in the human brain, in tandem with a hyperactive immune system may be the key drivers of brain fog associated with long covid❞
~ Dr. Matthew Campbell (one of the researchers)
Let’s break that down a little, borrowing some context from the paper itself:
- the leaky blood vessels are breaching the blood-brain-barrier
- that’s a big deal, because that barrier is our only filter between our brain and Things That Definitely Should Not Go In The Brain™
- a hyperactive immune system can also be described as chronic inflammation
- in this case, that includes chronic neuroinflammation which, yes, is also a major driver of dementia
You may be wondering what COVID has to do with this, and well:
- these blood-brain-barrier breaches were very significantly associated (in lay terms: correlated, but correlated is only really used as an absolute in write-ups) with either acute COVID infection, or Long Covid.
- checking this in vitro, exposure of brain endothelial cells to serum from patients with Long Covid induced the same expression of inflammatory markers.
How important is this?
As another researcher (not to mention: professor of neurology and head of the school of medicine at Trinity) put it:
❝The findings will now likely change the landscape of how we understand and treat post-viral neurological conditions.
It also confirms that the neurological symptoms of long covid are measurable with real and demonstrable metabolic and vascular changes in the brain.❞
~ Dr. Colin Doherty (see mini-bio above)
You can read a pop-science article about this here:
Irish researchers discover underlying cause of “brain fog” linked with long covid
…and you can read the paper in full here:
Want to stay safe?
Beyond the obvious “get protected when offered boosters/updates” (see also: The Truth About Vaccines), other good practices include the same things most people were doing when the pandemic was big news, especially avoiding enclosed densely-populated places, washing hands frequently, and looking after your immune system. For that latter, see also:
Beyond Supplements: The Real Immune-Boosters!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- the leaky blood vessels are breaching the blood-brain-barrier