3 drugs that went from legal, to illegal, then back again
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cannabis, cocaine and heroin have interesting life stories and long rap sheets. We might know them today as illicit drugs, but each was once legal.
Then things changed. Racism and politics played a part in how we viewed them. We also learned more about their impact on health. Over time, they were declared illegal.
But decades later, these drugs and their derivatives are being used legally, for medical purposes.
Here’s how we ended up outlawing cannabis, cocaine and heroin, and what happened next.
Cannabis, religion and racism
Cannabis plants originated in central Asia, spread to North Africa, and then to the Americas. People grew cannabis for its hemp fibre, used to make ropes and sacks. But it also had other properties. Like many other ancient medical discoveries, it all started with religion.
Cannabis is mentioned in the Hindu texts known as the Vedas (1700-1100 BCE) as a sacred, feel-good plant. Cannabis or bhang is still used ritually in India today during festivals such as Shivratri and Holi.
From the late 1700s, the British in India started taxing cannabis products. They also noticed a high rate of “Indian hemp insanity” – including what we’d now recognise as psychosis – in the colony. By the late 1800s, a British government investigation found only heavy cannabis use seemed to affect people’s mental health.

In the 1880s, cannabis was used therapeutically in the United States to treat tetanus, migraine and “insane delirium”. But not everyone agreed on (or even knew) the best dose. Local producers simply mixed up what they had into a tincture – soaking cannabis leaves and buds in alcohol to extract essential oils – and hoped for the best.
So how did cannabis go from a slightly useless legal drug to a social menace?
Some of it was from genuine health concerns about what was added to people’s food, drink and medicine.
In 1908 in Australia, New South Wales listed cannabis as an ingredient that could “adulterate” food and drink (along with opium, cocaine and chloroform). To sell the product legally, you had to tell the customers it contained cannabis.
Some of it was international politics. Moves to control cannabis use began in 1912 with the world’s first treaty against drug trafficking. The US and Italy both wanted cannabis included, but this didn’t happen until until 1925.
Some of it was racism. The word marihuana is Spanish for cannabis (later Anglicised to marijuana) and the drug became associated with poor migrants. In 1915, El Paso, Texas, on the Mexican border, was the first US municipality to ban the non-medical cannabis trade.
By the late 1930s, cannabis was firmly entrenched as a public menace and drug laws had been introduced across much of the US, Europe and (less quickly) Australia to prohibit its use. Cannabis was now a “poison” regulated alongside cocaine and opiates.

The 1936 movie Reefer Madness was a high point of cannabis paranoia. Cannabis smoking was also part of other “suspect” new subcultures such as Black jazz, the 1950s Beatnik movement and US service personnel returning from Vietnam.
Today recreational cannabis use is associated with physical and mental harm. In the short term, it impairs your functioning, including your ability to learn, drive and pay attention. In the long term, harms include increasing the risk of psychosis.
But what about cannabis as a medicine? Since the 1980s there has been a change in mood towards experimenting with cannabis as a therapeutic drug. Medicinal cannabis products are those that contain cannabidiol (CBD) or tetrahydrocannabinol (THC). Today in Australia and some other countries, these can be prescribed by certain doctors to treat conditions when other medicines do not work.
Medicinal cannabis has been touted as a treatment for some chronic conditions such as cancer pain and multiple sclerosis. But it’s not clear yet whether it’s effective for the range of chronic diseases it’s prescribed for. However, it does seem to improve the quality of life for people with some serious or terminal illnesses who are using other prescription drugs.
Cocaine, tonics and addiction
Several different species of the coca plant grow across Bolivia, Peru and Colombia. For centuries, local people chewed coca leaves or made them into a mildly stimulant tea. Coca and ayahuasca (a plant-based psychedelic) were also possibly used to sedate people before Inca human sacrifice.
In 1860, German scientist Albert Niemann (1834-1861) isolated the alkaloid we now call “cocaine” from coca leaves. Niemann noticed that applying it to the tongue made it feel numb.
But because effective anaesthetics such as ether and nitrous oxide had already been discovered, cocaine was mostly used instead in tonics and patent medicines.

Perhaps the most famous example was Coca-Cola, which contained cocaine when it was launched in 1886. But cocaine was used earlier, in 1860s Italy, in a drink called Vin Mariani – Pope Leo XIII was a fan.
With cocaine-based products easily available, it quickly became a drug of addiction.
Cocaine remained popular in the entertainment industry. Fictional detective Sherlock Holmes injected it, American actor Tallulah Bankhead swore by it, and novelist Agatha Christie used cocaine to kill off some of her characters.
In 1914, cocaine possession was made illegal in the US. After the hippy era of the 1960s and 1970s, cocaine became the “it” drug of the yuppie 1980s. “Crack” cocaine also destroyed mostly Black American urban communities.
Cocaine use is now associated with physical and mental harms. In the short and long term, it can cause problems with your heart and blood pressure and cause organ damage. At its worst, it can kill you. Right now, illegal cocaine production and use is also surging across the globe.
But cocaine was always legal for medical and surgical use, most commonly in the form of cocaine hydrochloride. As well as acting as a painkiller, it’s a vasoconstrictor – it tightens blood vessels and reduces bleeding. So it’s still used in some types of surgery.
Heroin, coughing and overdoses
Opium has been used for pain relief ever since people worked out how to harvest the sap of the opium poppy. By the 19th century, addictive and potentially lethal opium-based products such as laudanum were widely available across the United Kingdom, Europe and the US. Opium addiction was also a real problem.
Because of this, scientists were looking for safe and effective alternatives for pain relief and to help people cure their addictions.
In 1874, English chemist Charles Romley Alder Wright (1844-1894) created diacetylmorphine (also known as diamorphine). Drug firm Bayer thought it might be useful in cough medicines, gave it the brand name Heroin and put it on the market in 1898. It made chest infections worse.

Although diamorphine was created with good intentions, this opiate was highly addictive. Shortly after it came on the market, it became clear that it was every bit as addictive as other opiates. This coincided with international moves to shut down the trade in non-medical opiates due to their devastating effect on China and other Asian countries.
Like cannabis, heroin quickly developed radical chic. The mafia trafficked into the US and it became popular in the Harlem jazz scene, beatniks embraced it and US servicemen came back from Vietnam addicted to it. Heroin also helped kill US singers Janis Joplin and Jim Morrison.
Today, we know heroin use and addiction contributes to a range of physical and mental health problems, as well as death from overdose.
However, heroin-related harm is now being outpaced by powerful synthetic opioids such as oxycodone, fentanyl, and the nitazene group of drugs. In Australia, there were more deaths and hospital admissions from prescription opiate overdoses than from heroin overdoses.
In a nutshell
Not all medicines have a squeaky-clean history. And not all illicit drugs have always been illegal.
Drugs’ legal status and how they’re used are shaped by factors such as politics, racism and social norms of the day, as well as their impact on health.
Philippa Martyr, Lecturer, Pharmacology, Women’s Health, School of Biomedical Sciences, The University of Western Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What is silicosis and what does research say about it?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Silicosis is a progressive, debilitating and sometimes fatal lung disease caused by breathing silica dust from cutting, drilling, chipping or grinding materials such as granite, sandstone, slate or artificial stone. The dust gets trapped in the lung tissue, causing inflammation, scarring and permanent damage.
Silicosis is a job-related lung disease and has no cure. The disease mostly affects workers in construction, stone countertop fabrication, mining, and even those who sandblast and stonewash denim jeans to create a ‘worn out’ look.
Silica is one of the most common minerals in nature. About 59% of the Earth’s crust is made of silica, found in quartz, granite, sandstone, slate and sand. Historically, people at the highest risk for the disease have worked in natural environments — mining, digging tunnels or doing quarry work. The disease was first documented by the Greek physician Hippocrates, who in 430 B.C. described breathing disorders in metal diggers.
But in recent decades there’s been renewed attention to the disease due to its more rapid progression and severity among younger workers. Research has shown that the culprit is artificial stone mostly used for countertops for kitchens and bathrooms, which has a very high silica content.
The new generation of coal miners is also at an increased risk of silicosis, in addition to black lung, because layers of coal have become thinner, forcing them to dig deeper into rock, as explained in a joint investigation by the Pittsburgh Post-Gazette and the Medill Investigative Lab at Northwestern University published on Dec. 4. CBS Sunday Morning also had a report on the same issue among West Virginia coal miners, aired as part of its Dec. 10 episode.
Silicosis in modern industries
Artificial, or engineered, stone used for countertops, also known as “quartz,” is formed from finely crushed rocks mixed with resin. Quartz is a natural mineral, but man-made products like many quartz countertops consist of not just quartz, but also resin, colors and other materials that are used to style and strengthen them.
The silica content of artificial stone is about 90%, compared with the 3% silica content of natural marble and 30% silica content in granite stones, according to the authors of a 2019 systematic review published in the International Journal of Environmental Research and Public Health.
The first reported case of silicosis associated with working with artificial stone was from Italy in 2010, according to a 2020 study published in Allergy. Since then, more studies have documented the growing number of cases among artificial stone workers, many of whom are from marginalized populations, such as immigrants.
A July 2023 study published in JAMA Internal Medicine found that in California, the disease mainly occurred among young Latino immigrant men. The disease was severe in most men by the time they sought care.
An August 2022 study, published in Occupational & Environmental Medicine, analyzing the Global Silicosis Registry, with workers in Israel, Spain, Australia and the U.S., found “a substantial emerging population of workers worldwide with severe and irreversible silica-associated diseases,” due to exposure from silica dust from engineered stone.
Other modern occupations such as denim sandblasting, work on dental prostheses, manufacturing of electrical cables and working on jewelry and semi-precious stones also put workers at risk of silicosis.
In the wake of modern-day silicosis cases, researchers have called for larger studies to better understand the disease and the discovery of effective treatments.
In the U.S. about 2.3 million workers are exposed to silica dust on the job, according to the American Lung Association. Other estimates show approximately 10 million workers in India, 3.2 million in the European Union and 2 million in Brazil work with material containing silica.
However, “the reporting system for occupational injuries and illnesses in the United States fails to capture many cases, leading to a poor understanding of silicosis incidence and prevalence,” writes Ryan F. Hoy, who has published extensively on the topic, in a June 2022 article in Respirology.
A 2015 study in the Morbidity & Mortality Weekly Report found the annual number of silicosis deaths declined from 185 people in 1999 to 111 in 2013, but the decline appeared to have leveled off between 2010 and 2013, the authors write. Another 2015 study in MMWR, examining silicosis deaths between 2001 and 2010, found the death rate from silicosis was significantly higher among Black people compared with whites and other races. Men also have a significantly higher death rate from silicosis than women.
The 2019 Global Burden of Disease Study estimates that more than 12,900 people worldwide die from silicosis each year.
Silicosis has no cure, but it’s preventable when workers have access to proper respiratory protection and are educated on safe practices set by regulatory bodies such as the U.S. National Institute for Occupational Safety and Health. The European Network on Silica also has guidelines on handling and using materials containing silica. A March 2023 study published in Environmental Science and Pollution Research International finds that “education, training, and marketing strategies improve respirator use, while training and education motivate workers to use dust control measures.”
Silicosis symptoms and treatment
Symptoms of silicosis include cough, fatigue, shortness of breath and chest pain. There’s no specific test for silicosis. The first signs may show in an abnormal chest X-ray and a slowly developing cough, according to the American Lung Association.
Silicosis symptoms don’t appear right away in most cases, usually taking several years to develop working with silica dust. However, studies indicate that symptoms of silicosis due to exposure to artificial stone appear quicker than exposure to natural silica sources, potentially due to the higher concentration of silica in artificial stone.
There are three types of silicosis: acute (most commonly caused by working with artificial stone), accelerated and chronic, depending on the level of exposure to silica dust, according to the Centers for Disease Control and Prevention, which explains the severity of each type on its website.
Complications from silicosis can include tuberculosis, lung cancer, chronic bronchitis, kidney disease and autoimmune disorders. In some cases, silicosis can cause severe scarring of the lung tissue, leading to a condition called progressive massive fibrosis, or PMF. Some patients may require a lung transplant.
Lung damage from silicosis is irreversible, so treatment of silicosis is aimed at slowing down the disease and relieving its symptoms.
In 1995, the World Health Organization called for the elimination of silicosis by 2030, but research studies and news stories show it remains a threat to many workers.
Below, we have gathered several studies on the topic to help journalists bolster their reporting with academic research.
Research roundup
Artificial Stone Associated Silicosis: A Systematic Review
Veruscka Leso, et al. International Journal of Environmental Research and Public Health, February 2019.This systematic review aims to verify the association between exposure to silica dust in artificial stone and the development of silicosis.
Researchers narrowed down their selection from 75 papers to seven studies that met their inclusion criteria. The seven studies were from Australia, Israel and Spain. Most of the studies are observational and impede a definite association between exposure to silica while working with artificial stone and developing silicosis, the authors note.
However, “the unusually high incidence of the disease that was reported over short periods of investigations, and the comparable occupational histories of affected workers, all being involved in the manufacture and manipulation of engineered stones, may indicate a cause-effect relationship of this type.”
The review of studies reveals a lack of basic preventive measures such as lack of access to disposable masks; lack of information and training on the dangers of silica dust; and lack of periodic medical examinations, including a chest X-ray, among workers. There was limited environmental monitoring of dust levels at the workplace. Also, there was no dust suppression system, such as the use of water when polishing the stones, or effective ventilation. Machinery and tools weren’t properly set up and didn’t undergo routine checks, the authors write.
The authors recommend environmental monitoring for assessing silica levels in the workplace and verifying the effectiveness of personal protections. They also recommend the health surveillance of workers exposed to silica dust.
“Stakeholders, manufacturers, occupational risk prevention services, insurance companies for occupational accidents and diseases, business owners, occupational health physicians, general practitioners, and also employees should be engaged, not only in designing/planning processes and operational working environments, but also in assessing the global applicability of proactive preventive and protective measures to identify and control crystalline silica exposure, especially in new and unexpected exposure scenarios, the full extent of which cannot yet be accurately predicted,” they write.
Silica-Related Diseases in the Modern World
Ryan F. Hoy and Daniel C. Chambers. Allergy, November 2020.The study is a review of the mineralogy of silica, epidemiology, clinical and radiological features of the various forms of silicosis and other diseases associated with exposure to silica.
The primary factor associated with the development of silicosis is the intensity and duration of cumulative exposure to silica dust. Most countries regulate silica dust occupational exposure limits, generally in the range of 0.05 mg/m3 to 0.1 mg/m3, although the risk of dust exposure to workers still remains high at those levels.
The study provides a list of activities that could expose workers to silica dust. They include abrasive blasting of sand and sandstone; cement and brick manufacturing; mixing, glazing or sculpting of china, ceramic and pottery; construction involving bricklaying, concrete cutting, paving and demolition; sandblasting denim jeans; working with and polishing dental materials; mining and related milling; handling raw material during paint manufacturing; road and highway construction and repair; soap and cosmetic production; blasting and drilling tunnels; and waste incineration.
“Despite the large number of workers in the construction sector, there have been few studies of [silica dust] exposure in this industry,” the authors note.
Other than silicosis, conditions associated with silica exposure include sarcoidosis, an inflammatory disease that commonly affects the lungs and lymph nodes, autoimmune disease, lung cancer and pulmonary infections.
“Recent outbreaks of silica-associated disease highlight the need for constant vigilance to identify and control new and well-established sources of silica exposure. While there are currently no effective treatments for silicosis, it is a completely preventable lung disease,” the authors write.
A Systematic Review of the Effectiveness of Dust Control Measures Adopted to Reduce Workplace Exposure
Frederick Anlimah, Vinod Gopaldasani, Catherine MacPhail and Brian Davies. Environmental Science and Pollution Research International, March 2023.This study provides an overview of various interventions and their effectiveness in preventing exposure to silica dust based on a review of 133 studies from 16 countries, including the U.S., Canada, China, India, Taiwan and Australia, and published between 2010 and 2020.
These dust control measures range from simple work practices such as the use of respirators to more sophisticated technologies, such as water and air curtains and foam technology, the authors note.
The review finds increasing research interest in dust reduction, mainly in China. But overall, regulatory influence remains inadequate in preventing miners’ exposure to silica dust.
“Results from the review suggest that adopted interventions increase knowledge, awareness, and attitudes about respirator usage and generate positive perceptions about respirator usage while reducing misconceptions,” the authors write. “Interventions can increase the use, proper use, and frequency of use of respirators and the adoption readiness for dust controls but may not provide sustained motivation in workers for the continual use of dust controls or [personal protective equipment.]”
Notes from the Field: Surveillance of Silicosis Using Electronic Case Reporting — California, December 2022–July 2023
Jennifer Flattery, et al. Morbidity and Mortality Weekly Report, November 2023.This study examines the use of electronic case reporting to identify silicosis cases in California. Electronic case reporting, or eCR, is the automated, real-time exchange of case report information between electronic health records at health facilities at state and local public health agencies in the U.S. It is a joint effort between the Association of Public Health Laboratories, the Council of State and Territorial Epidemiologists, and the CDC. Currently, 208 health conditions can be reported using eCR. All 50 states and other U.S.-affiliated jurisdictions are connected to eCR. Once a public health agency receives a case report, it reaches out to the patient for contact tracing or other actions.
From October 2022 to July 2023, the California Department of Public Health received initial silicosis case reports for 41 individuals. A review of medical records confirmed 19 cases and 16 probable cases. Six of the 41 cases were considered unlikely to be silicosis after a review of medical records.
Notably, engineered stone countertop fabrication was a significant source of exposure, especially among Hispanic and Latino workers.
At least seven of the 19 confirmed cases were associated with the fabrication of engineered stone — quartz — countertops. The 19 patients’ ages ranged from 33 to 51 and all were Hispanic or Latino. One patient died and two had both lungs replaced. One was evaluated for a lung transplant.
The median age of the 35 patients with probable or confirmed silicosis was 65, ranging from 33 to 89 years, and 91% were men.
“It is important that health care providers routinely ask patients about their work as an important determinant of health,” the authors write. “Being aware of the risks associated with work exposures, as well as the regulations, medical monitoring, and prevention strategies that address those risks can help guide patient care.”
Additional research
Understanding the Pathogenesis of Engineered Stone-Associated Silicosis: The Effect of Particle Chemistry on the Lung Cell Response
Chandnee Ramkissoon, et al. Respirology, December 2023.Silicosis, Tuberculosis and Silica Exposure Among Artisanal and Small-Scale Miners: A Systematic Review and Modelling Paper
Patrick Howlett, et al. PLOS Global Public Health, September 2023.Silicosis Among Immigrant Engineered Stone (Quartz) Countertop Fabrication Workers in California
Jane C. Fazio, et al. JAMA Internal Medicine, July 2023.Silicosis and Tuberculosis: A Systematic Review and Meta-Analysis
P. Jamshidi, et al. Pulmonology, June 2023.From Basic Research to Clinical Practice: Considerations for Treatment Drugs for Silicosis
Rou Li, Huimin Kang and Shi Chen. International Journal of Molecular Science, May 2023.Silicosis After Short-Term Exposure
J. Nowak-Pasternak, A. Lipińska-Ojrzanowska and B. Świątkowska. Occupational Medicine, January 2023.Occupational Silica Exposure and Dose-Response for Related Disorders—Silicosis, Pulmonary TB, AIDs and Renal Diseases: Results of a 15-Year Israeli Surveillance
Rachel Raanan, et al. International Journal of Environmental Research and Public Health, November 2022.Demographic, Exposure and Clinical Characteristics in a Multinational Registry of Engineered Stone Workers with Silicosis
Jeremy Tang Hua, et al. Occupational & Environmental Medicine, August 2022.Current Global Perspectives on Silicosis — Convergence of Old and Newly Emergent Hazards
Ryan F. Hoy, et al. Respirology, March 2022.The Association Between Silica Exposure, Silicosis and Tuberculosis: A systematic Review and Metal-Analysis
Rodney Ehrlich, Paula Akugizibwe, Nandi Siegfried and David Rees. BMC Public Health, May 2021.Silicosis, Progressive Massive Fibrosis and Silico-Tuberculosis Among Workers with Occupational Exposure to Silica Dusts in Sandstone Mines of Rajasthan State
Subroto Nandi, Sarang Dhatrak, Kamalesh Sarkar. Journal of Family Medicine and Primary Care, February 2021.Artificial Stone Silicosis: Rapid Progression Following Exposure Cessation
Antonio León-Jiménez, et al. Chest, September 2020.Silica-Associated Lung Disease: An Old-World Exposure in Modern Industries
Hayley Barnes, Nicole S.L. Goh, Tracy L. Leong and Ryan Hoy. Respirology, September 2019.Australia Reports on Audit of Silicosis for Stonecutters
Tony Kirby. The Lancet, March 2019.Artificial Stone-Associated Silicosis: A Rapidly Emerging Occupational Lung Disease
Ryan F. Hoy, et al. Occupational & Environmental Medicine, December 2017.This article first appeared on The Journalist’s Resource and is republished here under a Creative Commons license.

Share This Post
-

Our blood-brain barrier stops bugs and toxins getting to our brain. Here’s how it works
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our brain is an extremely complex and delicate organ. Our body fiercely protects it by holding onto things that help it and keeping harmful things out, such as bugs that can cause infection and toxins.
It does that though a protective layer called the blood-brain barrier. Here’s how it works, and what it means for drug design.
The Conversation, Rattiya Thongdumhyu/Shutterstock, Petr Ganaj/Pexels First, let’s look at the circulatory system
Adults have roughly 30 trillion cells in their body. Every cell needs a variety of nutrients and oxygen, and they produce waste, which needs to be taken away.
Our circulatory system provides this service, delivering nutrients and removing waste.
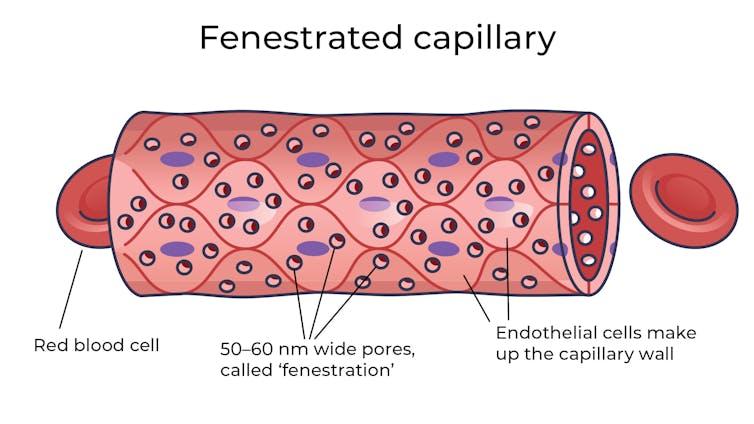
Fenestrated capillaries let nutrients and waste pass through. Vectormine/Shutterstock Where the circulatory system meets your cells, it branches down to tiny tubes called capillaries. These tiny tubes, about one-tenth the width of a human hair, are also made of cells.
But in most capillaries, there are some special features (known as fenestrations) that allow relatively free exchange of nutrients and waste between the blood and the cells of your tissues.
It’s kind of like pizza delivery
One way to think about the way the circulation works is like a pizza delivery person in a big city. On the really big roads (vessels) there are walls and you can’t walk up to the door of the house and pass someone the pizza.
But once you get down to the little suburban streets (capillaries), the design of the streets means you can stop, get off your scooter and walk up to the door to deliver the pizza (nutrients).
We often think of the brain as a spongy mass without much blood in it. In reality, the average brain has about 600 kilometres of blood vessels.
The difference between the capillaries in most of the brain and those elsewhere is that these capillaries are made of specialised cells that are very tightly joined together and limit the free exchange of anything dissolved in your blood. These are sometimes called continuous capillaries.
Continuous capillaries limit the free exchange of anything dissolved in your blood. Vectormine/Shutterstock This is the blood brain barrier. It’s not so much a bag around your brain stopping things from getting in and out but more like walls on all the streets, even the very small ones.
The only way pizza can get in is through special slots and these are just the right shape for the pizza box.
The blood brain barrier is set up so there are specialised transporters (like pizza box slots) for all the required nutrients. So mostly, the only things that can get in are things that there are transporters for or things that look very similar (on a molecular scale).
The analogy does fall down a little bit because the pizza box slot applies to nutrients that dissolve in water. Things that are highly soluble in fat can often bypass the slots in the wall.
Why do we have a blood-brain barrier?
The blood brain barrier is thought to exist for a few reasons.
First, it protects the brain from toxins you might eat (think chemicals that plants make) and viruses that often can infect the rest of your body but usually don’t make it to your brain.
It also provides protection by tightly regulating the movement of nutrients and waste in and out, providing a more stable environment than in the rest of the body.
Lastly, it serves to regulate passage of immune cells, preventing unnecessary inflammation which could damage cells in the brain.
What it means for medicines
One consequence of this tight regulation across the blood brain barrier is that if you want a medicine that gets to the brain, you need to consider how it will get in.
There are a few approaches. Highly fat-soluble molecules can often pass into the brain, so you might design your drug so it is a bit greasy.
The blood-brain barrier stops many medicines getting into the brain. Ron Lach/Pexels Another option is to link your medicine to another molecule that is normally taken up into the brain so it can hitch a ride, or a “pro-drug”, which looks like a molecule that is normally transported.
Using it to our advantage
You can also take advantage of the blood brain barrier.
Opioids used for pain relief often cause constipation. They do this because their target (opioid receptors) are also present in the nervous system of the intestines, where they act to slow movement of the intestinal contents.
Imodium (Loperamide), which is used to treat diarrhoea, is actually an opioid, but it has been specifically designed so it can’t cross the blood brain barrier.
This design means it can act on opioid receptors in the gastrointestinal tract, slowing down the movement of contents, but does not act on brain opioid receptors.
In contrast to Imodium, Ozempic and Victoza (originally designed for type 2 diabetes, but now popular for weight-loss) both have a long fat attached, to improve the length of time they stay in the body.
A consequence of having this long fat attached is that they can cross the blood-brain barrier, where they act to suppress appetite. This is part of the reason they are so effective as weight-loss drugs.
So while the blood brain barrier is important for protecting the brain it presents both a challenge and an opportunity for development of new medicines.
Sebastian Furness, ARC Future Fellow, School of Biomedical Sciences, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

The Forgotten Vitamin That Can Help vs Cancer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to eating vs cancer, usually the talk is about macros, for example: Eat To Beat Cancer
Indeed, whole books have been written on that, such as The Cancer Code − by Dr. William Fung
However, today we’re going to talk about an important (and vastly underrated) micronutrient:
Why niacin is extra nice
Niacin, also known as vitamin B3, is (like all vitamins) essential to health (part of the definition of “vitamin” is that we would literally die without it).
But most people have only a vague idea of what most vitamins do, with a common level of knowledge probably being something like:
- Vitamin A: good for the eyes
- Vitamin B1: is this for energy?
- Vitamin B2: who knows
- Vitamin B3: it is a mystery
- Vitamin B4: is this a real vitamin?
- Vitamin B5: energy?
- Vitamin B6: energy?
- Vitamin B7: good for skin, hair, & nails
- Vitamin B8: this isn’t a real vitamin
- Vitamin B9: something to do with pregnancy
- Vitamin B10: why so many B-vitamins?
- Vitamin B11: come on, this is too many
- Vitamin B12: energy!
- Vitamin C: skin!
- Vitamin D: bones!
- Vitamin E: skin!
- … (unlikely people think about the possibilities for vitamins F-J)
- Vitamin K: babies need this one, right?
And to quickly address those without getting too side-tracked: no, there are no vitamins B4, B8, B10, or B11, and all of the rest of them while the guesses were right, they had other important uses too.
You can learn a lot more here: Which B Vitamins? It Makes A Difference
In that article, we listed some of vitamin B3’s top things to know about:
- Function: aids metabolism, supports skin, nerves, and cholesterol levels
- Forms: niacin (nicotinic acid), niacinamide (nicotinamide), inositol hexanicotinate (flush-free niacin)
- Example foods: whole grains, peanuts (literally the best nut for this)
And now, researchers (Dr. Gloria Urgoiti et al.) tested high-dose controlled-release niacin (vitamin B3) alongside standard glioblastoma (a very common form of cancer) treatment and found very encouraging results!
In numbers:
- The participants: patients aged 18–75 with newly diagnosed glioblastoma received standard treatment plus controlled-release niacin
- The safety: the maximum tolerated dose was found to be 2,000mg/day. At 2,500mg/day, dose-limiting toxicities occurred, including severe thrombocytopenia and elevated bilirubin levels. The most common side effect was flushing, reported in 10 of 15 Phase I participants, with most cases being mild.
- The results: among the first wave of evaluable patients, 82.3% remained free of disease progression at 6 months (progression-free survival at six months, or “PFS-6M”).
- How that compares: historical studies of standard treatment report a six-month progression-free survival rate of about 53.9%.
So, that’s quite a difference!
As to how it works, the answer is, put very simply:
❝Niacin treatment rejuvenates immune cells so they can do what they are supposed to do, attack and kill the cancer cells❞
~ Dr. V. Wee Wong, co-author on the study
Want to learn more?
As for why you might want to favor getting this from food if you can, then while the title says “vitamins”, the following book discusses an assortment of vitamins, minerals, and other nutrients; the “other nutrients” category including amino acids (branched chain and essential), prebiotics and probiotics, and triglycerides of various kinds:
Eat Your Vitamins – by Mascha Davis, RDN ← see our review, here
Take care!
Share This Post




-
Supergreen Superfood Salad Slaw
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to “eating the rainbow”, in principle green should be the easiest color to get in, unless we live in a serious food desert (or serious food poverty). In practice, however, a lot of meals could do with a dash more green. This “supergreen superfood salad slaw” is remarkably versatile, and can be enjoyed as a very worthy accompaniment to almost any main.
You will need
For the bits:
- ½ small green cabbage, finely diced
- 7 oz tenderstem broccoli, finely chopped
- 2 stalks celery, finely chopped (if allergic, simply omit)
- ½ cucumber, diced into small cubes
- 2 oz kale, finely shredded
- 4 green (spring) onions, thinly sliced
For the dressing:
- 1 cup cashews (if allergic, substitute 1 cup roasted chickpeas)
- ½ cup extra virgin olive oil
- 2 oz baby spinach
- 1 oz basil leaves
- 1 oz chives
- ¼ bulb garlic
- 2 tbsp nutritional yeast
- 1 tbsp chia seeds
- Juice of two limes
Method
(we suggest you read everything at least once before doing anything)
1) Combine the ingredients from the “bits” category in a bowl large enough to accommodate them comfortably
2) Blend the ingredients from the “dressing” category in a blender until very smooth (the crux here is you do not want any stringy bits of spinach remaining)
3) Pour the dressing onto the bits, and mix well to combine. Refrigerate, ideally covered, until ready to serve.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Apple vs Cherries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apples to cherries, we picked the cherries.
Why?
In terms of macros, apples start out strong with a little more fiber, carbs, and protein, for a modest first-round win.
In the category of vitamins, however, apples boast only more vitamin E, while cherries have more of vitamins A, B1, B2, B3, B5, B7, B9, and C, winning this round easily.
Looking at minerals, apples are not higher any minerals, while cherries have more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, winning this round even more easily.
In other considerations, cherries have rather more polyphenols, especially anthocyanins and phenolic acids, and bring some extra health-giving phytochemical benefits that you can read about in the “learn more” section, below. Meanwhile, another round to cherries.
Adding up the sections makes for a clear overall win for cherries, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
Cherries’ Very Healthy Wealth Of Benefits!
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
“Skinny Fat” Explained (& How To Fix It)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Skinny fat” is a term you may have seen floating around social media. It describes people who have a low body weight but a high body fat percentage, often resulting in flabby appearance despite being within a weight range considered healthy. Many try dieting and exercising, only to find that neither work.
This video explains what’s going wrong, and how to fix it:
Diet & exercise won’t work if it’s not right
This problem occurs because common weight-loss approaches, such as restrictive dieting and excessive cardio, fail to improve body composition:
- Restrictive dieting reduces both fat and lean mass, keeping the body fat percentage unchanged
- Cardio burns some calories but the underlying metabolic issue hasn’t meaningfully changed, so any loss will be temporary (and most of any immediate loss will be water weight, anyway)
The key to overcoming skinny fat is resistance training. Lifting weights or doing bodyweight exercises helps build muscle, which not only lowers body fat percentage (by simple mathematics; add more muscle and the percentages of other things must go down even if the total amount is the same) and improves overall definition, which is something most people consider nice. However, the real value here is that it actually addresses the underlying metabolic issue—because muscle costs calories to maintain, one’s basal metabolic rate will now be faster, even when you’re sleeping.
This then becomes… Not quite a self-sustaining system, because you do have to still eat well and continue to do resistance training, but your body will be doing most of the work for you, and you’ll find it’s a lot easier to maintain a healthy body composition than to get one in the first place, for exactly the metabolic reason we described.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Visceral Belly Fat & How To Lose It ← this is a different, but adjacent issue (and very important for avoiding metabolic disease risks)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: