What’s the best way to support autistic kids with mild to moderate delay?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Autistic children with mild to moderate developmental delay will no longer be eligible for the National Disability Insurance Scheme (NDIS) from mid-2027.
Instead, they will be directed to a new support system called Thriving Kids. This is yet to be fully designed, but it’s intended to prioritise children receiving support through mainstream community-based services.
Understandably, some parents and professionals are concerned, and many are asking whether the new program can match the support currently provided through the NDIS.
While time will reveal the impact of the policy, the more urgent task now is to define and deliver what best practice looks like for autistic children.
Start with terminology
With the announcement came some confusion about autism and developmental delay.
Disability and NDIS Minister Mark Butler referred to children with “mild to moderate autism” which is not actually a diagnosis, or a way we talk about autism in contemporary practice.
A clearer way would have been to refer to children with developmental delay as the target group for Thriving Kids, noting it will include many, but not all, autistic children.
The wording is important because, from a clinical perspective, autism is a lifelong neurodevelopmental condition that influences the way a person understands and interacts with other people and the world around them. Children don’t “grow out of autism”, but needs can fluctuate over time.
Developmental delay is a term used when a child is behind their peers in one or more aspects of development, such as motor skills, communication, or cognition.
Many autistic children have a developmental delay, but not all.
A three-year-old autistic child may have a mild developmental delay in motor skills that impacts their ability to climb at the playground. A five-year-old autistic child may have a moderate delay in language, which impacts their ability to understand and follow instructions in the classroom. But another autistic child may be at, or above, the age expected level for their developmental milestones.
Around 25% of autistic children have profound disability, meaning they require 24/7 supervision and support to be safe.
By seeing autism and developmental delay as separate, but related, we are better able to understand and meet the different needs of children “across the spectrum”.
So what does best practice look like for autistic children with mild to moderate developmental delay?
Best practice for autistic children
Australia’s national guideline sets out recommendations for supporting the learning, participation and wellbeing of autistic children and their families.
The guideline puts forward a principles-based approach that places children and families at the centre, and includes recommendations for goal-setting, selecting and delivering supports, monitoring outcomes and safeguarding.
The goals for supporting autistic children are no different from those for all children. They need love, opportunities to learn through everyday activities, and strong connections with family, culture and community.
The difference comes when children are struggling, and the question shifts to what additional supports will help. Keeping this broader understanding front of mind makes every other decision about extra support clearer and more consistent.
A stepped care approach
The guideline states support should be personalised for each child and family. There is no blanket approach to supporting autistic children that will be equally beneficial for each child and family.
At a system level, it means a stepped-care model of support in which the right type of support is delivered at the right time and in the right amount to match the child’s age, developmental level, strengths, needs and family circumstances. This is best practice internationally and something we should strive for.
Let’s say a parent takes their child to a routine visit with a maternal child health nurse or GP, and there are signs of developmental delay. Perhaps the child is behind in terms of motor skills and communication.
In a stepped-care model, the nurse or doctor can listen, ask questions, and understand any concerns the parents may have. If some additional support is needed, the “next step” depends on exactly what was learned.
For one parent, the “next step” might be some information and strategies to encourage their child’s development, for another it might be connection to a community playgroup, and for another a referral for some further assessment.
If difficulties emerge in childcare or school settings, the most effective approach is usually to strengthen the capability of educators to include and support children.
There may also be scope for targeted specialist input, such as speech pathology, physiotherapy, or psychology, when needed.
The point is that the “steps” match the needs, and will be different for each child and family.
As professionals, we can support parents to make decisions by encouraging them to ask: “is this the best next step for my child and family?” This approach helps prevent the over-servicing that can happen when families are directed straight to the highest level of support.
What should happen next?
The new Thriving Kids program represents a genuine opportunity to transform how Australia supports children with mild to moderate developmental delays, including many autistic children.
Done well, it could become the stepped-care model of support that families desperately need. Get it wrong, and it becomes another well-intentioned policy that fails the children it’s meant to help.
Stepped-care models require deliberate design, sustained investment and careful attention to implementation details.
The key to getting this right lies in genuine co-design with the people who matter most: children and families themselves. They understand what works and what doesn’t, and where the gaps are.
David Trembath, Head of Autism Research and Senior Principal Research Fellow, The Kids Research Institute Australia; Andrew Whitehouse, Deputy Director, the Kids Research Institute Australia, The University of Western Australia, and Kandice Varcin, Senior Research Fellow in autism research, The Kids Research Institute Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

“Recovery is possible when we replace judgment with compassion”: How this mother turned pain into service for others

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is the second installment in a series about Pennsylvanians in recovery from substance use disorder and how stigma affected their recovery. The series is a collaboration between Public Good News, Centro Integral de la Mujer Madre Tierra, and Life Unites Us. If you’d like to share your story, contact us at mailto:[email protected].
[Editor’s note: The contents of this interview have been edited for length and clarity. This interview was originally conducted in Spanish.]
Carmen Albrecht, 58
Outreach bilingual coordinator at Peace and Harmony House in Berks County
Reading, PennsylvaniaI am a mother of five children. I have 22 grandchildren, six great-grandchildren, and I have been married for 16 years. I came to the United States from Puerto Rico in 1979, when my parents separated. My father struggled a lot with alcohol and was abusive toward my mother.
I stayed in the United States with my father, and during that time, I decided to start a family at a very young age. By the age of 21, I already had five children. Very shortly after having my children, I was introduced to cocaine. Less than a year later, I was completely addicted.
By 1996, I had lost my five children to social services because I had become consumed by my addiction.
It controlled me completely—not only mentally, but also physically and emotionally. It numbed so much of the sadness, pain, and loneliness I had back then as a single mother.
There were many times I tried to leave it behind because people wanted me to change so I could get my children back and move forward. I was a young person, only 27 years old. With addiction, I didn’t just lose my dignity—I lost my pride and my faith.
There were many blows along the way because my own people looked at me differently and no one respected me anymore. The stigma crushed me completely, and I kept going with that pain.
I was treated badly. People called me “drug addict,” “dirty,” and told me I was worthless. They said, “They took your children away because you deserved it,” and, “Your family will never accept you like that.” There was a time in 2002 when I sought help, and my children were returned to me—but about a year and a half later, or less, I lost them again.
This is something I wrote:
“During the struggle with addiction for more than 10 years, one of the deepest wounds did not come only from the drugs, but from the stigma that surrounded me. People who called me an ‘addict’ looked at me with contempt, as if I were less than human. Over time, those words began to feel like the truth. I felt useless. I felt worthless, convinced that this was the only future waiting for me. Stigma doesn’t just hurt—it completely crushes you. It makes you believe you don’t deserve help. It makes you hide from people, hide like a worm all tangled up, making you think there is no way out. And when you are already at your lowest point, that judgment can push you even deeper—and it does. It wasn’t until I went through many jails and institutions that I was able to slow down enough to see what I could do and realize that there was hope for me. There, I received structure and support and the opportunity to begin to rebuild myself.”
When I left prison, I had already met someone—and that person did not judge me for who I was. That person supported me. I remember thinking, “That can’t be real because nobody loves me.” But he was the only one who stayed there, standing strong with me. That’s how my recovery began.

Carmen with her husband. Courtesy of Carmen Albrecht. I had to go to court, see the judge, report to parole, deal with social services, take care of my mental health, keep a job, and maintain a home—and for me, that was overwhelming. But with the support of the person who is now my husband, and the support of the job I had, I was able to complete all those programs in 18 months.
Then I said to myself, “I have to make a change in my life. I have to help those who are where I once was.” If I don’t help them, they won’t find a way out because this is incredibly hard.
So I set aside all the things that hurt me so much. Those names people called me and the ways they hurt me, that was the addiction, that wasn’t who I truly was. I am different. I am a strong person, and I can do this. Little by little, I kept going. I started studying and went back to school. I earned my GED. I completed an 18-month program in drug and alcohol counseling and got my first job serving people with mental health needs. By 2008, I was working as an assistant to social workers in a halfway house.
I had a deep hunger to keep moving forward and to keep learning more about what drugs do to people, about the damage I had done to myself, and how I was able to overcome the stigma of how people treated me and how they saw me. I had to learn to walk with my head held high, not look back, and give myself the pride of knowing that I am not that person anymore. I had to look at myself in the mirror every morning and say, “Wow, I am beautiful.”
So I kept studying. I also graduated as a Certified Recovery Specialist. I have a diploma in drug and alcohol counseling, and I also have more than 200 certificates related to working with addiction, alcohol, mental health, and homelessness because I went through all of that myself.
Until recently, I worked at the Hope Rescue Mission with people struggling with addiction, homelessness, and mental health. And now I am working as a bilingual community outreach coordinator at Peace and Harmony House in Berks County.
Even at the age I am now, I want to keep going forward. I want to help in every way I can. I have been able to help thousands and thousands of people, and I have helped send many people to rehabilitation centers who trust me deeply. I have a family that loves me unconditionally. My grandchildren love me. And by the grace of God, today I have been sober for 21 years.
I have spent 18 years working in the field of addiction, walking alongside people who are living what I once lived. Every day I see how stigma continues to be a huge barrier for those seeking help. That’s why I speak about this because no one should be defined by their worst moments. Recovery is possible when we replace judgment with compassion.
If you or anyone you know is considering suicide or self-harm or is anxious, depressed, upset, or needs to talk, call the Suicide & Crisis Lifeline at 988 or text the Crisis Text Line at 741-741. For international resources, here is a good place to begin.
If you’re looking for substance use disorder or mental health help in Pennsylvania, find a list of resources here.
This article first appeared on Public Good News and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Share This Post
-

Never Too Old?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Age Limits On Exercise?
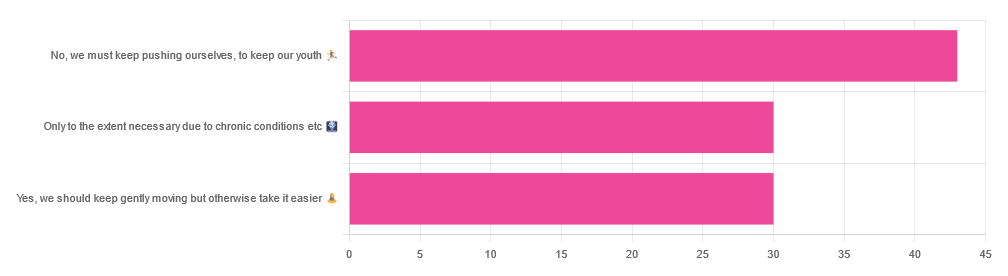
In Tuesday’s newsletter, we asked you your opinion on whether we should exercise less as we get older, and got the above-depicted, below-described, set of responses:
- About 42% said “No, we must keep pushing ourselves, to keep our youth“
- About 29% said “Only to the extent necessary due to chronic conditions etc”
- About 29% said “Yes, we should keep gently moving but otherwise take it easier”
One subscriber who voted for “No, we must keep pushing ourselves, to keep our youth“ wrote to add:
❝I’m 71 and I push myself. I’m not as fast or strong as I used to be but, I feel great when I push myself instead of going through the motions. I listen to my body!❞
~ 10almonds subscriber
One subscriber who voted for “Only to the extent necessary due to chronic conditions etc” wrote to add:
❝It’s never too late to get stronger. Important to keep your strength and balance. I am a Silver Sneakers instructor and I see first hand how helpful regular exercise is for seniors.❞
~ 10almonds subscriber
One subscriber who voted to say “Yes, we should keep gently moving but otherwise take it easier” wrote to add:
❝Keep moving but be considerate and respectful of your aging body. It’s a time to find balance in life and not put yourself into a positon to damage youself by competing with decades younger folks (unless you want to) – it will take much longer to bounce back.❞
~ 10almonds subscriber
These will be important, because we’ll come back to them at the end.
So what does the science say?
Endurance exercise is for young people only: True or False?
False! With proper training, age is no barrier to serious endurance exercise.
Here’s a study that looked at marathon-runners of various ages, and found that…
- the majority of middle-aged and elderly athletes have training histories of less than seven years of running
- there are virtually no relevant running time differences (p<0.01) per age in marathon finishers from 20 to 55 years
- after 55 years, running times did increase on average, but not consistently (i.e. there were still older runners with comparable times to the younger age bracket)
The researchers took this as evidence of aging being indeed a biological process that can be sped up or slowed down by various lifestyle factors.
See also:
Age & Aging: What Can (And Can’t) We Do About It?
this covers the many aspects of biological aging (it’s not one number, but many!) and how our various different biological ages are often not in sync with each other, and how we can optimize each of them that can be optimized
Resistance training is for young people only: True or False?
False! In fact, it’s not only possible for older people, but is also associated with a reduction in all-cause mortality.
Specifically, those who reported strength-training at least once per week enjoyed longer lives than those who did not.
You may be thinking “is this just the horse-riding thing again, where correlation is not causation and it’s just that healthier people (for other reasons) were able to do strength-training more, rather than the other way around?“
…which is a good think to think of, so well-spotted if you were thinking that!
But in this case no; the benefits remained when other things were controlled for:
❝Adjusted for demographic variables, health behaviors and health conditions, a statistically significant effect on mortality remained.
Although the effects on cardiac and cancer mortality were no longer statistically significant, the data still pointed to a benefit.
Importantly, after the physical activity level was controlled for, people who reported strength exercises appeared to see a greater mortality benefit than those who reported physical activity alone.❞
See the study: Is strength training associated with mortality benefits? A 15 year cohort study of US older adults
And a pop-sci article about it: Strength training helps older adults live longer
Closing thoughts
As it happens… All three of the subscribers we quoted all had excellent points!
Because in this case it’s less a matter of “should”, and more a selection of options:
- We (most of us, at least) can gain/regain/maintain the kind of strength and fitness associated with much younger people, and we need not be afraid of exercising accordingly (assuming having worked up to such, not just going straight from couch to marathon, say).
- We must nevertheless be mindful of chronic conditions or even passing illnesses/injuries, but that goes for people of any age
- We also can’t argue against a “safety first” cautious approach to exercise. After all, sure, maybe we can run marathons at any age, but that doesn’t mean we have to. And sure, maybe we can train to lift heavy weights, but if we’re content to be able to carry the groceries or perhaps take our partner’s weight in the dance hall (or the bedroom!), then (if we’re also at least maintaining our bones and muscles at a healthy level) that’s good enough already.
Which prompts the question, what do you want to be able to do, now and years from now? What’s important to you?
For inspiration, check out: Train For The Event Of Your Life!
Take care!
Share This Post
-
How Much Difference Can Short Bursts Of Exercise Make, Long-Term?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Exercise is good for the health” is not breaking news, and you don’t need a health science publication to tell you that.
But, most people do not do as much exercise as we’d like (even if we have the energy, often daily life gets in the way!), so, it’s reasonable to make sure that the exercise we do have time and energy to do, counts for as much good as possible!
So, here’s the science of doing just that:
What matters more, duration or intensity?
That’s the question that a team of researchers (Dr. Minxue Shen et al.) set out to answer, and found that indeed it’s not just total movement that matters—how intensely you move plays a major role in disease prevention.
Dr. Shen and her team looked at device-measured data (from wrist-worn fitness trackers) from 96,408 participants (of whom, 56.3% women, average age 62), over the course of 7 years.
What they found, in few words: participants who regularly engaged in short bursts of vigorous activity enjoyed significantly reduced risks of cardiovascular disease, atrial fibrillation, type 2 diabetes, inflammatory diseases, liver disease, respiratory disease, kidney disease, and dementia.
In particular, higher levels of vigorous activity were linked to:
- 63% lower risk of dementia
- 60% lower risk of type 2 diabetes
- 46% lower risk of death
As for the “which is best” question, intensity had a stronger protective effect than total activity for most diseases, especially inflammatory conditions and brain-related conditions.
There several main mechanisms of action that the researchers considered foremost:
- Short bursts of vigorous activity reduce inflammation, helping explain stronger effects on arthritis and psoriasis.
- Short bursts of intense activity stimulates protective brain chemicals and improve oxygen use, supporting lower dementia risk.
You may be wondering how little you can get away with. Per this study, a few minutes daily, adding up to 15–20 minutes per week, was already sufficient to deliver meaningful benefits.
See also: How Useful Is “Exercise Snacking”, Really?
The researchers also noted that short bursts like climbing stairs quickly, rushing for a bus, or brisk walking between tasks count too—it doesn’t have to be an intentional exercise session!
Writer’s anecdote: I remember one time my fitness tracker congratulated me on my good workout, and encouraged me to keep going, while I was changing my bedsheets!
You can read the paper in full, here: Volume vs intensity of physical activity and risk of cardiovascular and non-cardiovascular chronic diseases
If you’d like to get started, a good place to begin is: How To Do HIIT (Without Wrecking Your Body) ← important, because the “high-intensity” part can cause problems for some people, if not undertaken attentively!
Want to learn more?
You might like this book we reviewed a while back:
I Will Make You Passionate About Exercise – by Bevan Eyles
What this isn’t: a “just do it!” motivational pep-talk.
What this is: a compassionate and thoughtful approach to help non-exercisers become regular exercisers, by looking at the real life factors of what holds people back (learning from his own early failures as a coach, by paying attention now to things he inadvertently neglected back then), both in the material/practical and in the psychological/emotional.
Enjoy!
Share This Post



-
Age & Strength Loss: What Happens When, & How Much Is Unavoidable?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to aging and loss of strength, a lot of focus is placed on loss of muscle mass (sarcopenia).
We talked about this in our article: Protein vs Sarcopenia: How Much Do We Need, Really?
And that is important, but it’s not the whole story!
Strong at every age
You can be strong at every age, if and only if you’re very intentional about it.
Researchers (Dr. Maria Westerståhl et al.) followed 427 people for 47 years, repeatedly measuring fitness, strength, muscle endurance, and power from adolescence all the way through into older adulthood.
First, the bad news: physical performance overall peaks in early adulthood and begins declining at around 26 for women and 36 for men, with initially gradual losses that accelerate with advancing age.
About that acceleration: aerobic capacity and muscular endurance initially fall by about 0.3–0.6 percent per year, later speeding up to roughly 2.0–2.5 percent per year, and the deterioration in muscle power gets a similar age-related acceleration.
Next, the worse news: physical power specifically starts its decline even sooner than the other factors, with women having their peak around 19 and men having their peak around 27.
It does, however, get worse: total losses in physical capacity from peak to age 63 range from 30–48%, which latter end of the range is quite a dramatic loss of physical capacity indeed. Note that that’s the aggregate figure, so we’re not just talking about strength here.
Is there any good news? Yes: it’s never too late! People who became physically active in adulthood improved physical capacity by about 5–10%, showing that starting later still provides meaningful benefits. To be clear, that’s a net improvement of 5–10%, we’re not talking about shaving 5–10% off the 30–48% loss.
If you want to go through all these numbers (and more) in detail, here’s the paper: Rise and Fall of Physical Capacity in a General Population: A 47-Year Longitudinal Study
As for what this means in realistic terms: you’re probably not only not as strong as you used to be, but also not as fit, fast, mobile, and so forth. Your power (explosive power, like sprints or best-effort lifts) and endurance (like long-distance cardio, or isometric holds) are probably not what they used to be either.
- On the one hand, you can improve them.
- On the other hand, you do have to actually do it—merely knowing about it will not help if you don’t take action!
So, how to do that?
Read on…
Want to learn more?
Here are some very good starting points:
- Resistance Is Useful! (Especially As We Get Older)
- Overdone It? How To Speed Up Recovery After Exercise
- How To Do HIIT (Without Wrecking Your Body)
- HIIT, But Make It HIRT ← this is about high-intensity resistance training (HIRT); confusing the muscles like one confuses the heart in HIIT, which thus yields improved results
- Exercises To Do (And Ones To Avoid) If You Have Osteoporosis ← an important consideration for many
And if you’re really serious about it, then for a much deeper dive than we have room for here, we highly recommend this excellent book we reviewed a while back:
Unbreakable: A Woman’s Guide to Aging with Power – by Dr. Vonda Wright ← So, she wants us to avoid the train of sarcopenia → osteopenia → osteoporosis → fractures → infections → death, by reducing our risk factors early, and staying more robust and biologically younger.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Gut-Healthy Tacos
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Full of prebiotics and probiotics, healthy fats, colorful salad boasting vitamins and minerals aplenty, and of course satisfying protein too, these tacos are also boasting generous flavors to keep you coming back for more…
You will need
- 24 sardines—canned is fine (if vegetarian/vegan, substitute tempeh and season generously; marinade if you have time)
- 12 small wholewheat tortillas
- 1 14oz/400g can black beans, drained
- 1 ripe avocado, stoned and cut into small chunks
- 1 red onion, thinly sliced
- 1 little gem lettuce, shredded
- 12 cherry tomatoes, halved
- 1 bulb garlic, crushed
- 1 lemon, sliced
- 4 tbsp plain unsweetened yogurt (your choice what kind, but something with a live culture is best)
- 3oz pickled jalapeños, roughly chopped
- 1oz cilantro (or substitute parsley if you have the cilantro-tastes-like-soap gene), finely chopped
- 1 tbsp extra virgin olive oil
- 2 tsp black pepper
- 1 tsp smoked paprika
- Juice of 1 lime
- Optional: Tabasco sauce, or similar hot sauce
Method
(we suggest you read everything at least once before doing anything)
1) Preheat your oven to a low temperature; 200℉ or just under 100℃ is fine
2) Place the lemon slices on top of the sardines on top of foil on a baking tray; you want the foil to be twice as much as you’d expect to need, because now you’re going to fold it over and make a sort of sealed envelope. You could use a dish with a lid yes, but this way is better because there’s going to be less air inside. Upturn the edges of the envelope slightly so that juices won’t run out, and make sure the foil is imperfectly sealed so a little steam can escape but not much at a time. This will ensure it doesn’t dry out, while also ensuring your house doesn’t smell of fish. Put all this into the oven on a middle shelf.
3) Mix the lime juice with the onion in a bowl, and add the avocado and tomatoes, mixing gently. Add half the cilantro, and set aside.
4) Put the black beans in a sieve and pour boiling water over them to refresh and slightly warm them. Tip them into a bowl and add the olive oil, black pepper, and paprika. Mix thoroughly with a fork, and no need to be gentle this time; in fact, deliberately break the beans a little in this case.
5) Mix the yogurt, jalapeños, garlic, and remaining cilantro in a small bowl.
6) Get the warmed sardines from the oven; discard the lemon slices.
7) Assemble! We recommend the order: tortilla, lettuce, fish (2 per taco), black bean mixture, salad mixture, garlic jalapeño yogurt mixture. You can also add a splash of the hot sauce per your preference, or if catering for more people, let people add their own.
Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- We Are Such Stuff As Fish Are Made Of
- Level-Up Your Fiber Intake! (Without Difficulty Or Discomfort)
- Making Friends With Your Gut (You Can Thank Us Later)
- Our Top 5 Spices: How Much Is Enough For Benefits?
- Enjoy Pungent Polyphenols For Your Heart & Brain
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

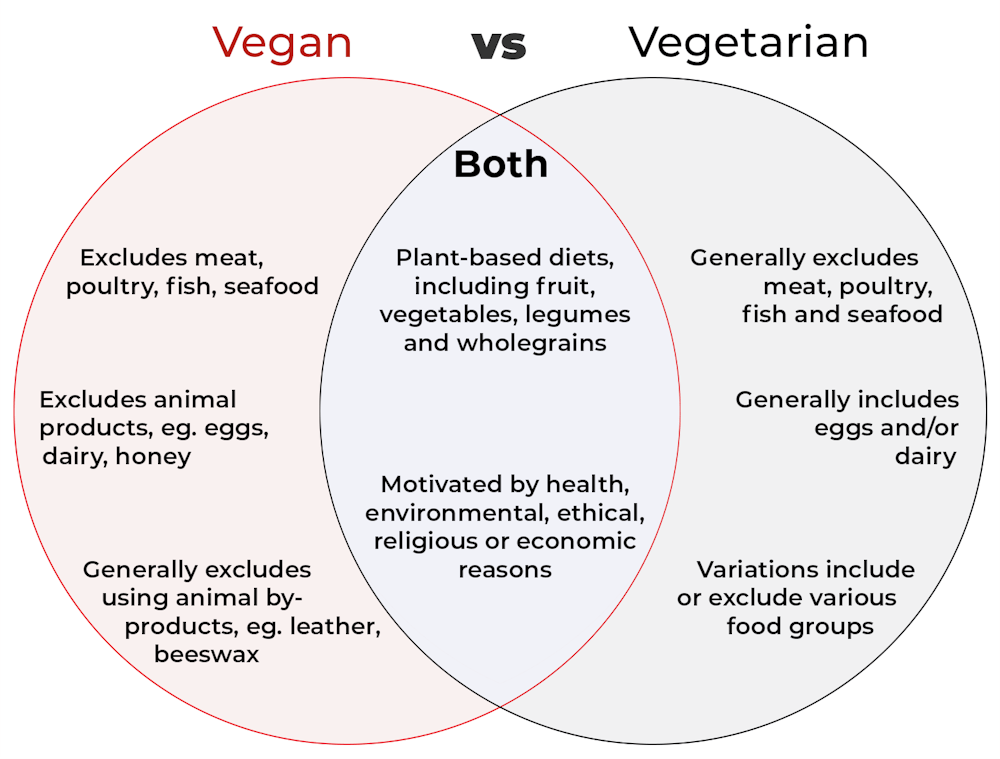
What’s the difference between vegan and vegetarian?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
Vegan and vegetarian diets are plant-based diets. Both include plant foods, such as fruits, vegetables, legumes and whole grains.
But there are important differences, and knowing what you can and can’t eat when it comes to a vegan and vegetarian diet can be confusing.
So, what’s the main difference?
Creative Cat Studio/Shutterstock What’s a vegan diet?
A vegan diet is an entirely plant-based diet. It doesn’t include any meat and animal products. So, no meat, poultry, fish, seafood, eggs, dairy or honey.
What’s a vegetarian diet?
A vegetarian diet is a plant-based diet that generally excludes meat, poultry, fish and seafood, but can include animal products. So, unlike a vegan diet, a vegetarian diet can include eggs, dairy and honey.
But you may be wondering why you’ve heard of vegetarians who eat fish, vegetarians who don’t eat eggs, vegetarians who don’t eat dairy, and even vegetarians who eat some meat. Well, it’s because there are variations on a vegetarian diet:
- a lacto-ovo vegetarian diet excludes meat, poultry, fish and seafood, but includes eggs, dairy and honey
- an ovo-vegetarian diet excludes meat, poultry, fish, seafood and dairy, but includes eggs and honey
- a lacto-vegetarian diet excludes meat, poultry, fish, seafood and eggs, but includes dairy and honey
- a pescatarian diet excludes meat and poultry, but includes eggs, dairy, honey, fish and seafood
- a flexitarian, or semi-vegetarian diet, includes eggs, dairy and honey and may include small amounts of meat, poultry, fish and seafood.
Are these diets healthy?
A 2023 review looked at the health effects of vegetarian and vegan diets from two types of study.
Observational studies followed people over the years to see how their diets were linked to their health. In these studies, eating a vegetarian diet was associated with a lower risk of developing cardiovascular disease (such as heart disease or a stroke), diabetes, hypertension (high blood pressure), dementia and cancer.
For example, in a study of 44,561 participants, the risk of heart disease was 32% lower in vegetarians than non-vegetarians after an average follow-up of nearly 12 years.
Further evidence came from randomised controlled trials. These instruct study participants to eat a specific diet for a specific period of time and monitor their health throughout. These studies showed eating a vegetarian or vegan diet led to reductions in weight, blood pressure, and levels of unhealthy cholesterol.
For example, one analysis combined data from seven randomised controlled trials. This so-called meta-analysis included data from 311 participants. It showed eating a vegetarian diet was associated with a systolic blood pressure (the first number in your blood pressure reading) an average 5 mmHg lower compared with non-vegetarian diets.
It seems vegetarian diets are more likely to be healthier, across a number of measures.
For example, a 2022 meta-analysis combined the results of several observational studies. It concluded a vegetarian diet, rather than vegan diet, was recommended to prevent heart disease.
There is also evidence vegans are more likely to have bone fractures than vegetarians. This could be partly due to a lower body-mass index and a lower intake of nutrients such as calcium, vitamin D and protein.
But it can be about more than just food
Many vegans, where possible, do not use products that directly or indirectly involve using animals.
So vegans would not wear leather, wool or silk clothing, for example. And they would not use soaps or candles made from beeswax, or use products tested on animals.
The motivation for following a vegan or vegetarian diet can vary from person to person. Common motivations include health, environmental, ethical, religious or economic reasons.
And for many people who follow a vegan or vegetarian diet, this forms a central part of their identity.
More than a diet: veganism can form part of someone’s identity. Shutterstock So, should I adopt a vegan or vegetarian diet?
If you are thinking about a vegan or vegetarian diet, here are some things to consider:
- eating more plant foods does not automatically mean you are eating a healthier diet. Hot chips, biscuits and soft drinks can all be vegan or vegetarian foods. And many plant-based alternatives, such as plant-based sausages, can be high in added salt
- meeting the nutrient intake targets for vitamin B12, iron, calcium, and iodine requires more careful planning while on a vegan or vegetarian diet. This is because meat, seafood and animal products are good sources of these vitamins and minerals
- eating a plant-based diet doesn’t necessarily mean excluding all meat and animal products. A healthy flexitarian diet prioritises eating more whole plant-foods, such as vegetables and beans, and less processed meat, such as bacon and sausages
- the Australian Dietary Guidelines recommend eating a wide variety of foods from the five food groups (fruit, vegetables, cereals, lean meat and/or their alternatives and reduced-fat dairy products and/or their alternatives). So if you are eating animal products, choose lean, reduced-fat meats and dairy products and limit processed meats.
Katherine Livingstone, NHMRC Emerging Leadership Fellow and Senior Research Fellow at the Institute for Physical Activity and Nutrition, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: