What Harm Can One Sleepless Night Do?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ll not bury the lede: a study found that just one night of 24-hour sleep deprivation can alter immune cell profiles in young, lean, healthy people to resemble those of people with obesity and chronic inflammation.
Chronic inflammation, in turn, causes very many other chronic diseases, and worsens most of the ones it doesn’t outright cause.
The reason this happens is because in principle, inflammation is supposed to be good for us—it’s our body’s defenses coming to the rescue. However, if we imagine our immune cells as firefighters, then compare:
- A team of firefighters who are in great shape and ready to deploy at a moment’s notice, are mostly allowed to rest, sometimes get training, and get called out to a fire from time time, just enough to keep them on their toes. Today, something in your house caught fire, and they showed up in 5 minutes and put it out safely.
- A team of firefighters who have been pulling 24-hour shifts every day for the past 20 years, getting called out constantly for lost cats, burned toast, wrong numbers, the neighbor’s music, a broken fridge, and even the occasional fire. Today, your printer got jammed so they broke down your door and also your windows just for good measure, and blasted your general desk area with a fire hose, which did not resolve the problem but now your computer itself is broken.
Which team would you rather have?
The former team is a healthy immune system; the latter is the immune system of someone with chronic inflammation.
But if it’s one night, it’s not chronic, right?
Contingently true. However, the problem is that because the immune profile was made to be like the bad team we described (imagine that chaos in your house, now remember that for this metaphor, it’s your body that that’s happening to), the immediate strong negative health impact will already have knock-on effects, which in turn make it more likely that you’ll struggle to get your sleep back on track quickly.
For example, the next night you may oversleep “to compensate”, but then the following day your sleep schedule is now slid back considerably; one thing leads to another, and a month later you’re thinking “I really must sort my sleep out”.
See also: How Regularity Of Sleep Can Be Even More Important Than Duration ← A recent, large (n=72,269) 8-year prospective* observational study of adults aged 40-79 found a strong association between irregular sleep and major cardiovascular events, to such an extent that it was worse than undersleeping.
*this means they started the study at a given point, and measured what happened for the next eight years—as opposed to a retrospective study, which would look at what had happened during the previous 8 years.
What about sleep fragmentation?
In other words: getting sleep, but heavily disrupted sleep.
The answer is: basically the same deal as with missed sleep.
Specifically, elevated proinflammatory cytokines (in this context, that’s bad) and an increase in nonclassical monocytes—as are typically seen in people with obesity and chronic inflammation.
Remember: these were young, lean, healthy participants going into the study, who signed up for a controlled sleep deprivation experiment.
This is important, because the unhealthy inflammatory profile means that people with such are a lot more likely to develop diabetes, heart disease, Alzheimer’s, and many more things besides. And, famously, most people in the industrialized world are not sleeping that well.
Even amongst 10almonds readers, a health-conscious demographic by nature, 62% of 10almonds readers do not regularly get the prescribed 7–9 hours sleep (i.e. they get under 7 hours).
You can see the data on this one, here: Why You Probably Need More Sleep ← yes, including if you are in the older age range; we bust that myth in the article too!*
*Unless you have a (rare!) mutated ADRB1 gene, which reduces that. But we also cover that in the article, and how to know whether you have it.
With regard to “most people in the industrialized world are not sleeping that well”, this means that most people in the industrialized world are subject to an unseen epidemic of sleep-deprivation-induced inflammation that is creating vulnerability to many other diseases. In short, the lifestyle of the industrialized world (especially: having to work certain hours) is making most of the working population sick.
Dr. Fatema Al-Rashed, lead researcher, concluded:
❝In the long term, we aim for this research to drive policies and strategies that recognize the critical role of sleep in public health.
We envision workplace reforms and educational campaigns promoting better sleep practices, particularly for populations at risk of sleep disruption due to technological and occupational demands.
Ultimately, this could help mitigate the burden of inflammatory diseases like obesity, diabetes, and cardiovascular diseases.❞
You can read the paper in full here: Impact of sleep deprivation on monocyte subclasses and function
What can we do about it?
With regard to sleep, we’ve written so much about this, but here are three key articles that contain a lot of valuable information:
- Get Better Sleep: Beyond The Basics
- Calculate (And Enjoy) The Perfect Night’s Sleep
- Safe Effective Sleep Aids For Seniors
…and with regard to inflammation, a good concise overview of how to dial it down is:
How To Prevent Or Reduce Inflammation
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

5 Steps To Quit Sugar Easily

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sugar is one of the least healthy things that most people consume, yet because it’s so prevalent, it can also be tricky to avoid at first, and the cravings can also be a challenge. So, how to quit it?
Step by step
Dr. Mike Hansen recommends the following steps:
- Be aware: a lot of sugar consumption is without realizing it or thinking about it, because of how common it is for there to be added sugar in things we might purchase ready-made, even supposedly healthy things like yogurts, or easy-to-disregard things like condiments.
- Recognize sugar addiction: a controversial topic, but Dr. Hansen comes down squarely on the side of “yes, it’s an addiction”. He wants us to understand more about the mechanics of how this happens, and what it does to us.
- Reduce gradually: instead of going “cold turkey”, he recommends we avoid withdrawal symptoms by first cutting back on liquid sugars like sodas, juices, and syrups, before eliminating solid sugar-heavy things like candy, sugar cookies, etc, and finally the more insidious “why did they put sugar in this?” added-sugar products.
- Find healthy alternatives: simple like-for-like substitutions; whole fruits instead of juices/smoothies, for example. 10almonds tip: stuffing dates with an almond each makes it very much like eating chocolate, experientially!
- Manage cravings: Dr. Hansen recommends distraction, and focusing on upping other healthy habits such as hydration, exercise, and getting more vegetables.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Which Sugars Are Healthier, And Which Are Just The Same?
- Mythbusting The Not-So-Sweet Science Of Sugar Addiction
Take care!
Share This Post
-

Women spend more of their money on health care than men. And no, it’s not just about ‘women’s issues’
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Medicare, Australia’s universal health insurance scheme, guarantees all Australians access to a wide range of health and hospital services at low or no cost.
Although access to the scheme is universal across Australia (regardless of geographic location or socioeconomic status), one analysis suggests women often spend more out-of-pocket on health services than men.
Other research has found men and women spend similar amounts on health care overall, or even that men spend a little more. However, it’s clear women spend a greater proportion of their overall expenditure on health care than men. They’re also more likely to skip or delay medical care due to the cost.
So why do women often spend more of their money on health care, and how can we address this gap?

Elizaveta Galitckaia/Shutterstock Women have more chronic diseases, and access more services
Women are more likely to have a chronic health condition compared to men. They’re also more likely to report having multiple chronic conditions.
While men generally die earlier, women are more likely to spend more of their life living with disease. There are also some conditions which affect women more than men, such as autoimmune conditions (for example, multiple sclerosis and rheumatoid arthritis).
Further, medical treatments can sometimes be less effective for women due to a focus on men in medical research.
These disparities are likely significant in understanding why women access health services more than men.
For example, 88% of women saw a GP in 2021–22 compared to 79% of men.
As the number of GPs offering bulk billing continues to decline, women are likely to need to pay more out-of-pocket, because they see a GP more often.
In 2020–21, 4.3% of women said they had delayed seeing a GP due to cost at least once in the previous 12 months, compared to 2.7% of men.
Data from the Australian Bureau of Statistics has also shown women are more likely to delay or avoid seeing a mental health professional due to cost.
Women are more likely to live with chronic medical conditions than men. Drazen Zigic/Shutterstock Women are also more likely to need prescription medications, owing at least partly to their increased rates of chronic conditions. This adds further out-of-pocket costs. In 2020–21, 62% of women received a prescription, compared to 37% of men.
In the same period, 6.1% of women delayed getting, or did not get prescribed medication because of the cost, compared to 4.9% of men.
Reproductive health conditions
While women are disproportionately affected by chronic health conditions throughout their lifespan, much of the disparity in health-care needs is concentrated between the first period and menopause.
Almost half of women aged over 18 report having experienced chronic pelvic pain in the previous five years. This can be caused by conditions such as endometriosis, dysmenorrhoea (period pain), vulvodynia (vulva pain), and bladder pain.
One in seven women will have a diagnosis of endometriosis by age 49.
Meanwhile, a quarter of all women aged 45–64 report symptoms related to menopause that are significant enough to disrupt their daily life.
All of these conditions can significantly reduce quality of life and increase the need to seek health care, sometimes including surgical treatment.
Of course, conditions like endometriosis don’t just affect women. They also impact trans men, intersex people, and those who are gender diverse.
Diagnosis can be costly
Women often have to wait longer to get a diagnosis for chronic conditions. One preprint study found women wait an average of 134 days (around 4.5 months) longer than men for a diagnosis of a long-term chronic disease.
Delays in diagnosis often result in needing to see more doctors, again increasing the costs.
Despite affecting about as many people as diabetes, it takes an average of between six-and-a-half to eight years to diagnose endometriosis in Australia. This can be attributed to a number of factors including society’s normalisation of women’s pain, poor knowledge about endometriosis among some health professionals, and the lack of affordable, non-invasive methods to accurately diagnose the condition.
There have been recent improvements, with the introduction of Medicare rebates for longer GP consultations of up to 60 minutes. While this is not only for women, this extra time will be valuable in diagnosing and managing complex conditions.
But gender inequality issues still exist in the Medicare Benefits Schedule. For example, both pelvic and breast ultrasound rebates are less than a scan for the scrotum, and no rebate exists for the MRI investigation of a woman’s pelvic pain.
Management can be expensive too
Many chronic conditions, such as endometriosis, which has a wide range of symptoms but no cure, can be very hard to manage. People with endometriosis often use allied health and complementary medicine to help with symptoms.
On average, women are more likely than men to use both complementary therapies and allied health.
While women with chronic conditions can access a chronic disease management plan, which provides Medicare-subsidised visits to a range of allied health services (for example, physiotherapist, psychologist, dietitian), this plan only subsidises five sessions per calendar year. And the reimbursement is usually around 50% or less, so there are still significant out-of-pocket costs.
In the case of chronic pelvic pain, the cost of accessing allied or complementary health services has been found to average A$480.32 across a two-month period (across both those who have a chronic disease management plan and those who don’t).
More spending, less saving
Womens’ health-care needs can also perpetuate financial strain beyond direct health-care costs. For example, women with endometriosis and chronic pelvic pain are often caught in a cycle of needing time off from work to attend medical appointments.
Our preliminary research has shown these repeated requests, combined with the common dismissal of symptoms associated with pelvic pain, means women sometimes face discrimination at work. This can lead to lack of career progression, underemployment, and premature retirement.
More women are prescribed medication than men. PeopleImages.com – Yuri A/Shutterstock Similarly, with 160,000 women entering menopause each year in Australia (and this number expected to increase with population growth), the financial impacts are substantial.
As many as one in four women may either shift to part-time work, take time out of the workforce, or retire early due to menopause, therefore earning less and paying less into their super.
How can we close this gap?
Even though women are more prone to chronic conditions, until relatively recently, much of medical research has been done on men. We’re only now beginning to realise important differences in how men and women experience certain conditions (such as chronic pain).
Investing in women’s health research will be important to improve treatments so women are less burdened by chronic conditions.
In the 2024–25 federal budget, the government committed $160 million towards a women’s health package to tackle gender bias in the health system (including cost disparities), upskill medical professionals, and improve sexual and reproductive care.
While this reform is welcome, continued, long-term investment into women’s health is crucial.
Mike Armour, Associate Professor at NICM Health Research Institute, Western Sydney University; Amelia Mardon, Postdoctoral Research Fellow in Reproductive Health, Western Sydney University; Danielle Howe, PhD Candidate, NICM Health Research Institute, Western Sydney University; Hannah Adler, PhD Candidate, Health Communication and Health Sociology, Griffith University, and Michelle O’Shea, Senior Lecturer, School of Business, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Caffeine Blues – by Stephen Cherniske
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Caffeine use is an interesting and often-underexamined factor in health. Beyond the most superficial of sleep hygiene advice (à la “if you aren’t sleeping well, consider skipping your triple espresso martini at bedtime”), it’s often considered a “everybody has this” drug.
In this book, Cherniske explores a lot of the lesser-known effects of caffeine, and the book certainly is a litany against caffeine dependence, ultimately arguing strongly against caffeine use itself. The goal is certainly to persuade the reader to desist in caffeine use, and while the book’s selling point is “learn about caffeine” not “how to quit caffeine”, a program for quitting caffeine is nevertheless included.
You may notice the title and cover design are strongly reminiscent of “Sugar Blues”, which came decades before it, and that’s clearly not accidental. The style is similar—very sensationalist, and with a lot of strong claims. In this case, however, there is actually a more robust bibliography, albeit somewhat dated now as science has continued to progress since this book was published.
Bottom line: in this reviewer’s opinion, the book overstates its case a little, and is prone to undue sensationalism, but there is a lot of genuinely very good information in here too, making it definitely worth reading.
Share This Post





-

Healthy Hormones And How To Hack Them
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Healthy Hormones And How To Hack Them!
Hormones are vital for far more than they tend to get credit for. Even the hormones that people think of first—testosterone and estrogen—do a lot more than just build/maintain sexual characteristics and sexual function. Without them, we’d lack energy, we’d be depressed, and we’d soon miss the general smooth-running of our bodies that we take for granted.
And that’s without getting to the many less-talked-about hormones that play a secondary sexual role or are in the same general system…
How are your prolactin levels, for example?
Unless you’re ill, taking certain medications, recently gave birth, or picked a really interesting time to read this newsletter, they’re probably normal, by the way.
But, prolactin can explain “la petite mort”, the downturn in energy and the somewhat depressed mood that many men experience after orgasm.
Otherwise, if you have too much prolactin in general, you will be sleepy and depressed.
Prolactin’s primary role? In women, it stimulates milk production when needed. In men, it plays a role in regulating mood and metabolism.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

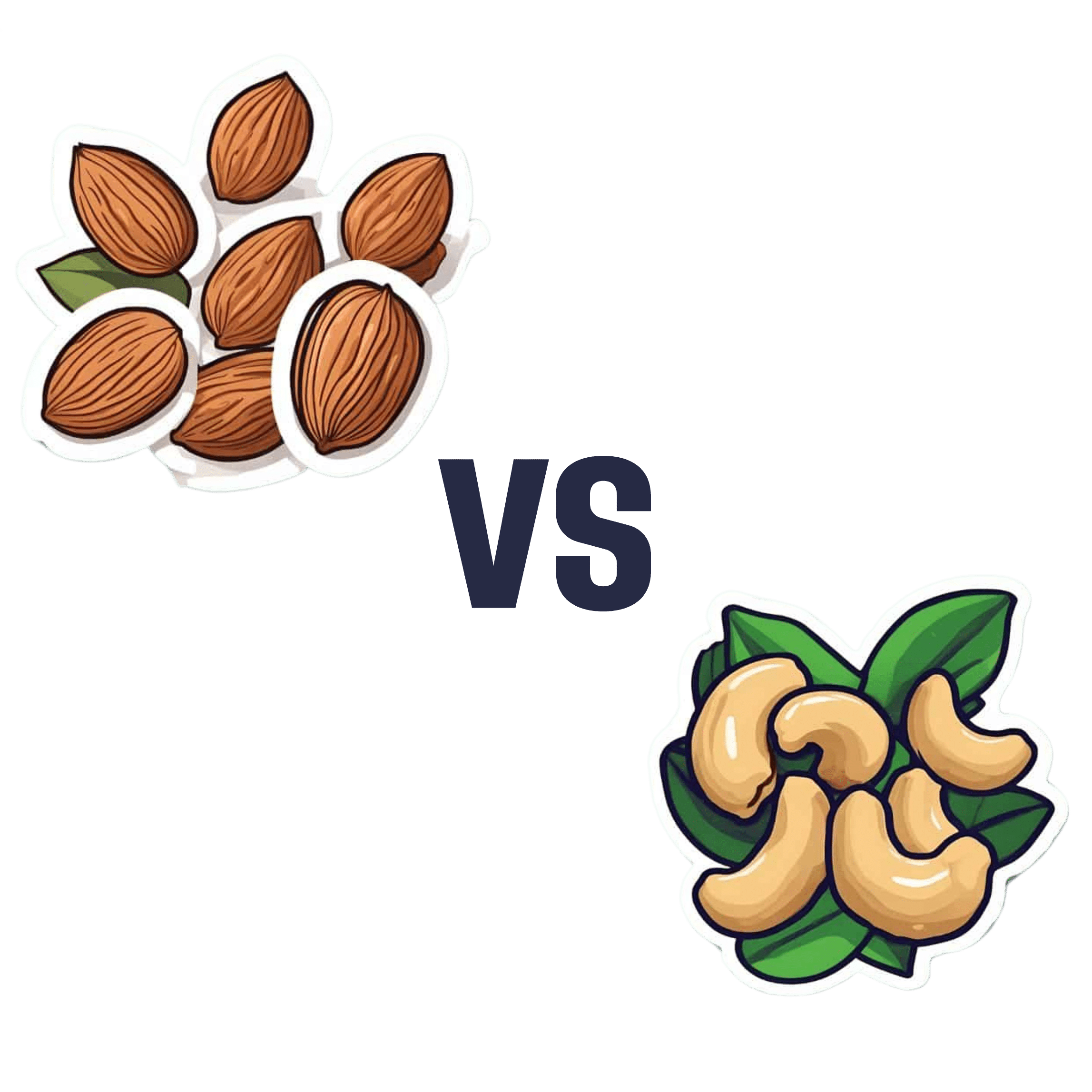
Almonds vs Cashews – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing almonds to cashews, we picked the almonds.
Why?
Both are great! But here’s why we picked the almonds:
In terms of macros, almonds have a little more protein and more than 4x the fiber. Given how critical fiber is to good health, and how most people in industrialized countries in general (and N. America in particular) aren’t getting enough, we consider this a major win for almonds.
Things are closer to even for vitamins, but almonds have a slight edge. Almonds are higher in vitamins A, B2, B3, B9, and especially 27x higher in vitamin E, while cashews are higher in vitamins B1, B5, B6, C & K. So, a moderate win for almonds.
In the category of minerals, cashews do a bit better on average. Cashews have moderately more copper, iron, phosphorus, selenium, and zinc, while almonds boast 6x more calcium, and slightly more manganese and potassium. We say this one’s a slight win for cashews.
Adding the categories up, however, makes it clear that almonds win the day.
However, of course, enjoy both! Diversity is healthy. Just, if you’re going to choose between them, we recommend almonds.
Want to learn more?
You might like to read:
- Why You’re Probably Not Getting Enough Fiber (And How To Fix It)
- Almonds vs Walnuts – Which is Healthier?
- Pistachios vs Cashews – Which is Healthier?
- Why You Should Diversify Your Nuts!
- What Matters Most For Your Heart?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Is It Dementia?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Spot The Signs (Because None Of Us Are Immune)
Dementia affects increasingly many people, and unlike a lot of diseases, it disproportionately affects people in wealthy industrialized nations.
There are two main reasons for this:
- Longevity (in poorer countries, more people die of other things sooner; can’t get age-related cognitive decline if you don’t age)
- Lifestyle (in the age of convenience, it has never been easier to live an unhealthy lifestyle)
The former is obviously no bad thing for those of us lucky enough to be in wealthier countries (though even in such places, good healthcare access is of course sadly not a given for all).
The latter, however, is less systemic and more epidemic. But it does cut both ways:
- An unhealthy lifestyle is much easier here, yes
- A healthier lifestyle is much easier here, too!
This then comes down to two factors in turn:
- Information: knowing about dementia, what things lead to it, what to look out for, what to do
- Motivation: priorities, and how much attention we choose to give this matter
So, let’s get some information, and then give it our attention!
More than just memory
It’s easy to focus on memory loss, but the four key disabilities directly caused by dementia (each person may not get all four), can be remembered by the mnemonic: “AAAA!”
No, somebody didn’t just murder your writer. It’s:
- Amnesia: memory loss, in one or more of its many forms
- e.g. short term memory loss, and/or inability to make new memories
- Aphasia: loss of ability to express oneself, and/or understand what is expressed
- e.g. “More people have been to Berlin than I have”
- Or even less communication-friendly, Broca’s (Expressive) Aphasia and Wernicke’s (Receptive) Aphasia
- Apraxia: loss of ability to do things, through no obvious physical disability
- e.g. staring at the bathroom mirror wondering how to brush one’s teeth
- Agnosia: loss of ability to recognize things
- e.g. prosopagnosia, also called face-blindness.
If any of those seem worryingly familiar, be aware that while yes, it could be a red flag, what’s most important is patterns of these things.
Another difference between having a momentary brainlapse and having dementia might be, for example, the difference between forgetting your keys, and forgetting what keys do or how to use one.
That said, some are neurological deficits that may show up quite unrelated to dementia, including most of those given as examples above. So if you have just one, then that’s probably worthy of note, but probably not dementia.
Writer’s anecdote: I have had prosopagnosia all my life. To give an example of what that is like and how it’s rather more than just “bad with faces”…
Recently I saw my neighbor, and I could tell something was wrong with her face, but I couldn’t put my finger on what it was. Then some moments later, I realized I had mistaken her hat for her face. It was a large beanie with a panda design on it, and that was facelike enough for me to find myself looking at the wrong face.
Subjective memory matters as much as objective
Objective memory tests are great indicators of potential cognitive decline (or improvement!), but even a subjective idea of having memory problems, that one’s memory is “not as good as it used to be”, can be an important indicator too:
Subjective memory may be marker for cognitive decline
And more recently:
If your memory feels like it’s not what it once was, it could point to a future dementia risk
If you’d like an objective test of memory and other cognitive impairments, here’s the industry’s gold standard test (it’s free):
SAGE: A Test to Detect Signs of Alzheimer’s and Dementia
(The Self-Administered Gerocognitive Exam (SAGE) is designed to detect early signs of cognitive, memory or thinking impairments)
There are things that can look like dementia that aren’t
A person with dementia may be unable to recognize their partner, but hey, this writer knows that feeling very well too. So what sets things apart?
More than we have room for today, but here’s a good overview:
What are the early signs of dementia, and how does it differ from normal aging?
Want to read more?
You might like our previous article more specifically about reducing Alzheimer’s risk:
Reducing Alzheimer’s Risk Early!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: