What happens if I eat too much protein?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The hype around protein intake doesn’t seem to be going away.
Social media is full of people urging you to eat more protein, including via supplements such as protein shakes. Food companies have also started highlighting protein content on food packages to promote sales.
But is all the extra protein giving us any benefit – and can you have too much protein?

Protein’s important – but many eat more than they need
Eating enough protein is important. It helps form muscle tissue, enzymes and hormones and it plays a role in immune function. It can also give you energy.
Australia’s healthy eating guidelines, penned by experts and backed by government, recommend we get 15–25% of our daily energy needs from protein.
The recommended daily intake of protein for adults is 0.84 grams per kilogram of body weight for men and 0.75 grams per kilogram of body weight for women
This is about 76 grams per day for a 90 kilogram man or 53 grams per day for a 70 kilogram woman. (It’s a bit more if you’re over 70 or a child, though).
Most Australian adults are already eating plenty of protein.
Even so, many people still go out of their way to add even more protein to their diet.
For people working to increase muscle mass through resistance training, such as lifting weights, a protein intake up to 1.6 grams per kilogram of body weight per day (that’s 144 grams a day for a 90 kilogram person) can help with increasing muscle strength and size.
But research shows there is no additional muscle gain benefit from eating any more than that.
For most of us, there’s no benefit in consuming protein above the recommended level.
In fact, having too much protein can cause problems.

What happens when I eat too much protein?
Excess protein is not all simply excreted from the body in urine or faeces. It stays in the body and has various effects.
Protein is a source of energy, so eating more protein means taking in more energy.
When we consume more energy than we need, our body converts any excess into fatty tissue for storage.
There are some health conditions where excess protein intake should be avoided. For example, people with chronic kidney disease should closely monitor their protein intake, under the supervision of a dietitian, to avoid damage to the kidneys.
There is also a condition called protein poisoning, which is where you eat too many proteins without getting enough fats, carbohydrates and other nutrients.
It’s also known as “rabbit starvation”, a term often linked to early 20th century explorer Vilhjalmur Stefansson, in reference to the fact that those who subsisted on a diet of mainly rabbits (which are famously lean) quickly fell dangerously ill.
Where you get your protein from matters
We can get protein in our diets from plant sources (such as beans, lentils, wholegrains) and animal sources (such as eggs, dairy, meat or fish).
A high intake of protein from animal sources has been associated with an increased risk of premature death among older Australians (especially death from cancer).
High animal protein intake is also associated with increased risk of type 2 diabetes.
On the other hand, consuming more plant sources of protein is associated with:
- a lower risk of dying from cancer
- a reduced risk of type 2 diabetes and
- improved blood cholesterol levels.
Many animal sources of protein are also relatively high in fat, particularly saturated fat.
A high intake of saturated fat contributes to increased risk of chronic diseases such as heart disease. Many Australians already eat more saturated fat than we need.
Many plant sources of protein, however, are also sources of dietary fibre, which most Australians don’t get enough of.
Having more dietary fibre helps reduce the risk of chronic diseases (such as heart disease) and supports gut health.
Striking a balance
Overall, where you get protein from – and having a balance between animal and plant sources – is more important than simply just trying to add ever more protein to your diet.
Protein, fats and carbohydrates all work together to keep your body healthy and the engine running smoothly.
We need all of these macro nutrients, along with vitamins and minerals, in the right proportions to support our health.
Margaret Murray, Senior Lecturer, Nutrition, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How Likely Are You To Live To 100?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How much hope can we reasonably have of reaching 100?
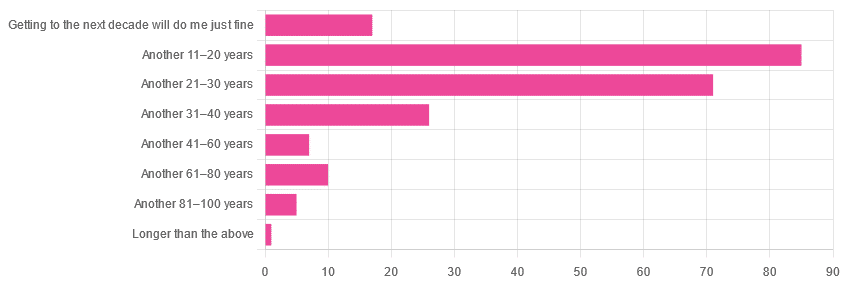
Yesterday, we asked you: assuming a good Health-Related Quality of Life (HRQoL), how much longer do you hope to live?

We got the above-depicted, below-described, set of responses:
- A little over 38% of respondents hope to live another 11–20 years
- A little over 31% hope to live another 31–40 years
- A little over 7% will be content to make it to the next decade
- One (1) respondent hopes to live longer than an additional 100 years
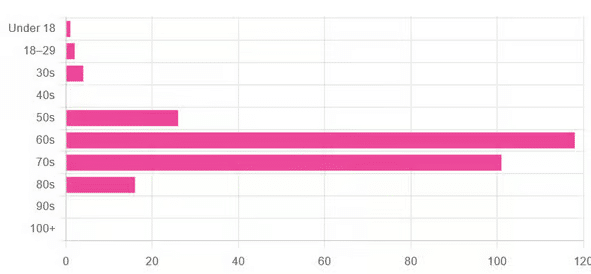
This is interesting when we put it against our graph of how old our subscribers are:

…because it corresponds inversely, right down to the gap/dent in the 40s. And—we may hypothesize—that one person under 18 who hopes to live to 120, perhaps.
This suggests that optimism remains more or less constant, with just a few wobbles that would probably be un-wobbled with a larger sample size.
In other words: most of our education-minded, health-conscious subscriber-base hope to make it to the age of 90-something, while for the most part feeling that 100+ is overly optimistic.
Writer’s anecdote: once upon a time, I was at a longevity conference in Brussels, and a speaker did a similar survey, but by show of hands. He started low by asking “put your hands up if you want to live at least a few more minutes”. I did so, with an urgency that made him laugh, and say “Don’t worry; I don’t have a gun hidden up here!”
Conjecture aside… What does the science say about our optimism?
First of all, a quick recap…
To not give you the same information twice, let’s note we did an “aging mythbusting” piece already covering:
- Aging is inevitable: True or False?
- Aging is, and always will be, unstoppable: True or False?
- We can slow aging: True or False?
- It’s too early to worry about… / It’s too late to do anything about… True or False?
- We can halt aging: True or False?
- We can reverse aging: True or False?
- But those aren’t really being younger, we’ll still die when our time is up: True or False?
You can read the answers to all of those here:
Age & Aging: What Can (And Can’t) We Do About It?
Now, onwards…
It is unreasonable to expect to live past 100: True or False?
True or False, depending on your own circumstances.
First, external circumstances: the modal average person in Hong Kong is currently in their 50s and can expect to live into their late 80s, while the modal average person in Gaza is 14 and may not expect to make it to 15 right now.
To avoid extremes, let’s look at the US, where the modal average person is currently in their 30s and can expect to live into their 70s:
United States Mortality Database
Now, before that unduly worries our many readers already in their 70s…
Next, personal circumstances: not just your health, but your socioeconomic standing. And in the US, one of the biggest factors is the kind of health insurance one has:
SOA Research Institute | Life Expectancy Calculator 2021
You may note that the above source puts all groups into a life expectancy in the 80s—whereas the previous source gave 70s.
Why is this? It’s because the SOA, whose primary job is calculating life insurance risks, is working from a sample of people who have, or are applying for, life insurance. So it misses out many people who die younger without such.
New advances in medical technology are helping people to live longer: True or False?
True, assuming access to those. Our subscribers are mostly in North America, and have an economic position that affords good access to healthcare. But beware…
On the one hand:
The number of people who live past the age of 100 has been on the rise for decades
On the other hand:
The average life expectancy in the U.S. has been on the decline for three consecutive years
COVID is, of course, largely to blame for that, though:
❝The decline of 1.8 years in life expectancy was primarily due to increases in mortality from COVID-19 (61.2% of the negative contribution).
The decline in life expectancy would have been even greater if not for the offsetting effects of decreases in mortality due to cancer (43.1%)❞
Source: National Vital Statistics Reports
The US stats are applicable to Canada, the UK, and Australia: True or False?
False: it’s not quite so universal. Differences in healthcare systems will account for a lot, but there are other factors too:
- Life expectancy in Canada fell for the 3rd year in a row. What’s happening?
- UK life expectancy lagging behind rest of G7 except the US
- Australians are living longer but what does it take to reach 100 years old?
Here’s an interesting (UK-based) tool that calculates not just your life expectancy, but also gives the odds of living to various ages (e.g. this writer was given odds of living to 87, 96, 100).
Check yours here:
Office of National Statistics | Life Expectancy Calculator
To finish on a cheery note…
Data from Italian centenarians suggests a “mortality plateau”:
❝The risk of dying leveled off in people 105 and older, the team reports online today in Science.
That means a 106-year-old has the same probability of living to 107 as a 111-year-old does of living to 112.
Furthermore, when the researchers broke down the data by the subjects’ year of birth, they noticed that over time, more people appear to be reaching age 105.❞
Pop-sci source: Once you hit this age, aging appears to stop
Actual paper: The plateau of human mortality: demography of longevity pioneers
Take care!
Share This Post
-

Clean Needles Save Lives. In Some States, They Might Not Be Legal.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Kim Botteicher hardly thinks of herself as a criminal.
On the main floor of a former Catholic church in Bolivar, Pennsylvania, Botteicher runs a flower shop and cafe.
In the former church’s basement, she also operates a nonprofit organization focused on helping people caught up in the drug epidemic get back on their feet.
The nonprofit, FAVOR ~ Western PA, sits in a rural pocket of the Allegheny Mountains east of Pittsburgh. Her organization’s home county of Westmoreland has seen roughly 100 or more drug overdose deaths each year for the past several years, the majority involving fentanyl.
Thousands more residents in the region have been touched by the scourge of addiction, which is where Botteicher comes in.
She helps people find housing, jobs, and health care, and works with families by running support groups and explaining that substance use disorder is a disease, not a moral failing.
But she has also talked publicly about how she has made sterile syringes available to people who use drugs.
“When that person comes in the door,” she said, “if they are covered with abscesses because they have been using needles that are dirty, or they’ve been sharing needles — maybe they’ve got hep C — we see that as, ‘OK, this is our first step.’”
Studies have identified public health benefits associated with syringe exchange services. The Centers for Disease Control and Prevention says these programs reduce HIV and hepatitis C infections, and that new users of the programs are more likely to enter drug treatment and more likely to stop using drugs than nonparticipants.
This harm-reduction strategy is supported by leading health groups, such as the American Medical Association, the World Health Organization, and the International AIDS Society.
But providing clean syringes could put Botteicher in legal danger. Under Pennsylvania law, it’s a misdemeanor to distribute drug paraphernalia. The state’s definition includes hypodermic syringes, needles, and other objects used for injecting banned drugs. Pennsylvania is one of 12 states that do not implicitly or explicitly authorize syringe services programs through statute or regulation, according to a 2023 analysis. A few of those states, but not Pennsylvania, either don’t have a state drug paraphernalia law or don’t include syringes in it.
Those working on the front lines of the opioid epidemic, like Botteicher, say a reexamination of Pennsylvania’s law is long overdue.
There’s an urgency to the issue as well: Billions of dollars have begun flowing into Pennsylvania and other states from legal settlements with companies over their role in the opioid epidemic, and syringe services are among the eligible interventions that could be supported by that money.
The opioid settlements reached between drug companies and distributors and a coalition of state attorneys general included a list of recommendations for spending the money. Expanding syringe services is listed as one of the core strategies.
But in Pennsylvania, where 5,158 people died from a drug overdose in 2022, the state’s drug paraphernalia law stands in the way.
Concerns over Botteicher’s work with syringe services recently led Westmoreland County officials to cancel an allocation of $150,000 in opioid settlement funds they had previously approved for her organization. County Commissioner Douglas Chew defended the decision by saying the county “is very risk averse.”
Botteicher said her organization had planned to use the money to hire additional recovery specialists, not on syringes. Supporters of syringe services point to the cancellation of funding as evidence of the need to change state law, especially given the recommendations of settlement documents.
“It’s just a huge inconsistency,” said Zoe Soslow, who leads overdose prevention work in Pennsylvania for the public health organization Vital Strategies. “It’s causing a lot of confusion.”
Though sterile syringes can be purchased from pharmacies without a prescription, handing out free ones to make drug use safer is generally considered illegal — or at least in a legal gray area — in most of the state. In Pennsylvania’s two largest cities, Philadelphia and Pittsburgh, officials have used local health powers to provide legal protection to people who operate syringe services programs.
Even so, in Philadelphia, Mayor Cherelle Parker, who took office in January, has made it clear she opposes using opioid settlement money, or any city funds, to pay for the distribution of clean needles, The Philadelphia Inquirer has reported. Parker’s position signals a major shift in that city’s approach to the opioid epidemic.
On the other side of the state, opioid settlement funds have had a big effect for Prevention Point Pittsburgh, a harm reduction organization. Allegheny County reported spending or committing $325,000 in settlement money as of the end of last year to support the organization’s work with sterile syringes and other supplies for safer drug use.
“It was absolutely incredible to not have to fundraise every single dollar for the supplies that go out,” said Prevention Point’s executive director, Aaron Arnold. “It takes a lot of energy. It pulls away from actual delivery of services when you’re constantly having to find out, ‘Do we have enough money to even purchase the supplies that we want to distribute?’”
In parts of Pennsylvania that lack these legal protections, people sometimes operate underground syringe programs.
The Pennsylvania law banning drug paraphernalia was never intended to apply to syringe services, according to Scott Burris, director of the Center for Public Health Law Research at Temple University. But there have not been court cases in Pennsylvania to clarify the issue, and the failure of the legislature to act creates a chilling effect, he said.
Carla Sofronski, executive director of the Pennsylvania Harm Reduction Network, said she was not aware of anyone having faced criminal charges for operating syringe services in the state, but she noted the threat hangs over people who do and that they are taking a “great risk.”
In 2016, the CDC flagged three Pennsylvania counties — Cambria, Crawford, and Luzerne — among 220 counties nationwide in an assessment of communities potentially vulnerable to the rapid spread of HIV and to new or continuing high rates of hepatitis C infections among people who inject drugs.
Kate Favata, a resident of Luzerne County, said she started using heroin in her late teens and wouldn’t be alive today if it weren’t for the support and community she found at a syringe services program in Philadelphia.
“It kind of just made me feel like I was in a safe space. And I don’t really know if there was like a come-to-God moment or come-to-Jesus moment,” she said. “I just wanted better.”
Favata is now in long-term recovery and works for a medication-assisted treatment program.
At clinics in Cambria and Somerset Counties, Highlands Health provides free or low-cost medical care. Despite the legal risk, the organization has operated a syringe program for several years, while also testing patients for infectious diseases, distributing overdose reversal medication, and offering recovery options.
Rosalie Danchanko, Highlands Health’s executive director, said she hopes opioid settlement money can eventually support her organization.
“Why shouldn’t that wealth be spread around for all organizations that are working with people affected by the opioid problem?” she asked.
In February, legislation to legalize syringe services in Pennsylvania was approved by a committee and has moved forward. The administration of Gov. Josh Shapiro, a Democrat, supports the legislation. But it faces an uncertain future in the full legislature, in which Democrats have a narrow majority in the House and Republicans control the Senate.
One of the bill’s lead sponsors, state Rep. Jim Struzzi, hasn’t always supported syringe services. But the Republican from western Pennsylvania said that since his brother died from a drug overdose in 2014, he has come to better understand the nature of addiction.
In the committee vote, nearly all of Struzzi’s Republican colleagues opposed the bill. State Rep. Paul Schemel said authorizing the “very instrumentality of abuse” crossed a line for him and “would be enabling an evil.”
After the vote, Struzzi said he wanted to build more bipartisan support. He noted that some of his own skepticism about the programs eased only after he visited Prevention Point Pittsburgh and saw how workers do more than just hand out syringes. These types of programs connect people to resources — overdose reversal medication, wound care, substance use treatment — that can save lives and lead to recovery.
“A lot of these people are … desperate. They’re alone. They’re afraid. And these programs bring them into someone who cares,” Struzzi said. “And that, to me, is a step in the right direction.”
At her nonprofit in western Pennsylvania, Botteicher is hoping lawmakers take action.
“If it’s something that’s going to help someone, then why is it illegal?” she said. “It just doesn’t make any sense to me.”
This story was co-reported by WESA Public Radio and Spotlight PA, an independent, nonpartisan, and nonprofit newsroom producing investigative and public-service journalism that holds power to account and drives positive change in Pennsylvania.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-

Why You Can’t Skimp On Amino Acids
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our body requires 20 amino acids (the building blocks of protein), 9 of which it can’t synthesize (thus called: “essential”) and absolutely must get from food. Normally, we get these amino acids from protein in our diet, and we can also supplement them by taking amino acid supplements if we wish.
Specifically, we require (per kg of bodyweight) a daily average of:
- Histidine: 10 mg
- Isoleucine: 20 mg
- Leucine: 39 mg
- Lysine: 30 mg
- Methionine: 10.4 mg
- Phenylalanine*: 25 mg
- Threonine: 15 mg
- Tryptophan: 4 mg
- Valine: 26 mg
*combined with the non-essential amino acid tyrosine
Source: Protein and Amino Acid Requirements In Human Nutrition: WHO Technical Report
Why this matters
A lot of attention is given to protein, and making sure we get enough of it, especially as we get older, because the risk of sarcopenia (muscle mass loss) increases with age:
However, not every protein comes with a complete set of essential amino acids, and/or have only trace amounts of of some amino acids, meaning that a dietary deficiency can arrive if one’s diet is too restrictive.
And, if we become deficient in even just one amino acid, then bad things start to happen quite soon. We only have so much space, so we’re going to oversimplify here, but:
- Histidine: is needed to produce histamine (vital for immune responses, amongst other things), and is also important for maintaining the myelin sheaths on nerve cells.
- Isoleucine: is very involved in muscle metabolism and makes up the bulk of muscle tissue.
- Leucine: is critical for muscle synthesis and repair, as well as wound healing in general, and blood sugar regulation.
- Lysine: is also critical in muscle synthesis, as well as calcium absorption and hormone production, as well as making collagen.
- Methionine: is very important for energy metabolism, zinc absorption, and detoxification.
- Phenylalanine: is a necessary building block of a lot of neurotransmitters, as well as being a building block of some amino acids not listed here (i.e., the ones your body synthesizes, but can’t without phenylalanine).
- Threonine: is mostly about collagen and elastin production, and is also very important for your joints, as well as fat metabolism.
- Tryptophan: is the body’s primary precursor to serotonin, so good luck making the latter without the former.
- Valine: is mostly about muscle growth and regeneration.
So there you see, the ill effects of deficiency can range from “muscle atrophy” to “brain stops working” and “bones fall apart” and more. In short, any essential amino acid deficiency not remedied will ultimately result in death; we literally become non-viable as organisms without these 9 things.
What to do about it (the “life hack” part)
Firstly, if you eat a lot of animal products, those are “complete” proteins, meaning that they contain all 9 essential amino acids in sensible quantities. The reason that all animal products have these, is because they are just as essential for the other animals as they are for us, so they, just like us, must consume (and thus contain) them.
However, a lot of animal products come with other health risks:
Do We Need Animal Products To Be Healthy? ← this covers which animal products are definitely very health-risky, and which are probably fine according to current best science
…so many people may prefer to get more (or possibly all) dietary protein from plants.
However, plants, unlike us, do not need to consume all 9 essential amino acids, and thus may or may not contain them all.
Soy is famously a “complete” protein insofar as it has all the amino acids we need.
But what if you’re allergic to soy?
Good news! Peas are also a “complete” protein and will do the job just fine. They’re also usually cheaper.
Final note
An oft-forgotten thing is that some other amino acids are “conditionally essential”, meaning that while we can technically synthesize them, sometimes we can’t synthesize enough and must get them from our diet.
The conditions that trigger this “conditionally essential” status are usually such things as fighting a serious illness, recovering from a serious injury, or pregnancy—basically, things where your body has to work at 110% efficiency if it wants to get through it in one piece, and that extra 10% has to come from somewhere outside the body.
Examples of commonly conditionally essential amino acids are arginine and glycine.
Arginine is critical for a lot of cell-signalling processes as well as mitochondrial function, as well as being a precursor to other amino acids, including creatine.
As for glycine?
Check out: The Sweet Truth About Glycine
Enjoy!
Share This Post

-
We analysed almost 1,000 social media posts about 5 popular medical tests. Most were utterly misleading
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When Kim Kardashian posted on Instagram about having had a full-body MRI, she enthused that the test can be “life saving”, detecting diseases in the earliest stages before symptoms arise.
What Kardashian neglected to say was there’s no evidence this expensive scan can bring benefits for healthy people. She also didn’t mention it can carry harms including unnecessary diagnoses and inappropriate treatments.
With this post in mind, we wanted to explore what influencers are telling us about medical tests.
In a new study published today in JAMA Network Open, we analysed nearly 1,000 Instagram and TikTok posts about five popular medical tests which can all do more harm than good to healthy people, including the full-body MRI scan.
We found the overwhelming majority of these posts were utterly misleading.

C-R-V/Shutterstock 5 controversial tests
Before we get into the details of what we found, a bit about the five tests included in our study.
While these tests can be valuable to some, all five carry the risk of overdiagnosis for generally healthy people. Overdiagnosis is the diagnosis of a condition which would have never caused symptoms or problems. Overdiagnosis leads to overtreatment, which can cause unnecessary side effects and stress for the person, and wasted resources for the health system.
As an example, estimates suggest 29,000 cancers a year are overdiagnosed in Australia alone.
Overdiagnosis is a global problem, and it’s driven in part by healthy people having tests like these. Often, they’re promoted under the guise of early screening, as a way to “take control” of your health. But most healthy people simply don’t need them.
These are the five tests we looked at:
The full-body MRI scan claims to test for up to 500 conditions, including cancer. Yet there is no proven benefit of the scan for healthy people, and a real risk of unnecessary treatment from “false alarm” diagnoses.
The “egg timer” test (technically known as the AMH, or anti-mullarian hormone test) is often falsely promoted as a fertility test for healthy women. While it may be beneficial for women within a fertility clinic setting, it cannot reliably predict the chance of a woman conceiving, or menopause starting. However, low results can increase fear and anxiety, and lead to unnecessary and expensive fertility treatments.
Multi-cancer early detection blood tests are being heavily marketed as the “holy grail of cancer detection”, with claims they can screen for more than 50 cancers. In reality, clinical trials are still a long way from finished. There’s no good evidence yet that the benefits will outweigh the harms of unnecessary cancer diagnoses.
The gut microbiome test of your stool promises “wellness” via early detection of many conditions, from flatulence to depression, again without good evidence of benefit. There’s also concern that test results can lead to wasted resources.
Testosterone testing in healthy men is not supported by any high-quality evidence, with concerns direct-to-consumer advertising leads men to get tested and take testosterone replacement therapy unnecessarily. Use of testosterone replacement therapy carries its own risk of potential harms with the long-term safety in relation to heart disease and mortality still largely unknown.
Multi-cancer early detection blood tests are heavily marketed. Yuri A/Shutterstock What we found
Together with an international group of health researchers, we analysed 982 posts pertaining to the above tests from across Instagram and TikTok. The posts we looked at came from influencers and account holders with at least 1,000 followers, some with a few million followers. In total, the creators of the posts we included had close to 200 million followers.
Even discounting the bots, that’s a massive amount of influence (and likely doesn’t reflect their actual reach to non-followers too).
The vast majority of posts were misleading, failing to even mention the possibility of harm arising from taking one of these tests. We found:
- 87% of posts mentioned test benefits, while only 15% mentioned potential harms
- only 6% of posts mentioned the risk of overdiagnosis
- only 6% of posts discussed any scientific evidence, while 34% of posts used personal stories to promote the test
- 68% of influencers and account holders had financial interests in promoting the test (for example, a partnership, collaboration, sponsorship or selling for their own profit in some way).
Further analysis revealed medical doctors were slightly more balanced in their posts. They were more likely to mention the harms of the test, and less likely to have a strongly promotional tone.
The vast majority of posts we looked at were misleading. DimaBerlin/Shutterstock As all studies do, ours had some limitations. For example, we didn’t analyse comments connected to posts. These may give further insights into the information being provided about these tests, and how social media users perceive them.
Nonetheless, our findings add to the growing body of evidence showing misleading medical information is widespread on social media.
What can we do about it?
Experts have proposed a range of solutions including pre-bunking strategies, which means proactively educating the public about common misinformation techniques.
However, solutions like these often place responsibility on the individual. And with all the information on social media to navigate, that’s a big ask, even for people with adequate health literacy.
What’s urgently needed is stronger regulation to prevent misleading information being created and shared in the first place. This is especially important given social media platforms including Instagram are moving away from fact-checking.
In the meantime, remember that if information about medical tests promoted by influencers sounds too good to be true, it probably is.
Brooke Nickel, NHMRC Emerging Leader Research Fellow, University of Sydney; Joshua Zadro, NHMRC Emerging Leader Research Fellow, Sydney Musculoskeletal Health, University of Sydney, and Ray Moynihan, Assistant Professor, Faculty of Health Sciences & Medicine, Bond University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Bored of Lunch – by Nathan Anthony
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cooking with a slow cooker is famously easy, but often we settle down on a few recipes and then don’t vary. This book brings a healthy dose of inspiration and variety.
The recipes themselves range from comfort food to fancy entertaining, pasta dishes to risottos, and even what the author categorizes as “fakeaways” (a play on the British English “takeaway”, cf. AmE “takeout”), so indulgent nights in have never been healthier!
For each recipe, you’ll see a nice simple clear layout of all you’d expect (ingredients, method, etc) plus calorie count, so that you can have a rough idea of how much food each meal is.
In terms of dietary restrictions you may have, there’s quite a variety here so it’ll be easy to find things for all needs, and in addition to that, optional substitutions are mostly quite straightforward too.
Bottom line: if you have a slow cooker but have been cooking only the same three things in it for the past ten years, this is the book to liven things up, while staying healthy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The Best Way To Take Creatine: Timing, Dosage, & More
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Creatine is mostly associated with bodybuilding, but its benefits go far beyond that, and also change with age:
Muscle & brain benefits
Creatine offers benefits beyond exercise, such as improving muscle, strength, quickness, memory, and reducing dementia risk. Creatine monohydrate is the most common and effective form; it’s tasteless, inexpensive, and widely available. Get it micronized if you want to to be non-clumping (easier to mix into liquids), but this is only a physical change not a chemical one, and doesn’t affect its effects.
Dr. Hardwick-Smith recommends, as a daily dose:
- If under 120 lbs: start with 2.5g
- If between 120–160 lbs: start with 5g
- If over 160 lbs: consider starting with 10g
Doses up to 30 grams/day have been studied with no harm.
Many people use higher doses for the first week (a “loading period”), but this is not necessary and can cause bloating due to water retention, so she recommends not doing that.
About timing, she says that consistency is key: take it daily at a regular convenient time, such as paired to some time-specific habit, for example one’s morning coffee. Beyond that, she says timing and food intake do not matter—just take it regularly.
For more on all of this in her own words, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Creatine: Very Different For Young & Old People
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: