Tribulus Terrestris For Testosterone?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
(Clinical) Trials and Tribul-ations
In the category of supplements that have enjoyed use as aphrodisiacs, Tribulus terrestris (also called caltrop, goat’s head, gokshura, or puncture vine) has a long history, having seen wide use in both Traditional Chinese Medicine and in Ayurveda.
It’s been used for other purposes too, and has been considered a “general wellness” plant.
So, what does the science say?
Good news: very conclusive evidence!
Bad news: the conclusion is not favorable…
Scientists are known for their careful use of clinical language, and it’s very rare for a study/review to claim something as proven (scientists leave journalists to do that part), and in this case, when it comes to Tribulus’s usefulness as a testosterone-enhancing libido-boosting supplement…
❝analysis of empirical evidence from a comprehensive review of available literature proved this hypothesis wrong❞
Strong words! You can read it in full here; they do make some concessions along the way (e.g. mentioning unclear or contradictory findings, suggesting that it may have some effect, but by an as-yet unknown mechanism if it does—although some potential effect on nitric oxide levels has been hypothesized, which is reasonable if so, as NO does feature in arousal-signalling), but the general conclusion is “no, this doesn’t have androgen-enhancing properties”:
Pro-sexual and androgen enhancing effects of Tribulus terrestris L.: Fact or Fiction
That’s a review though, what about taking a look at a representative RCT? Here we go:
❝Tribulus terrestris was not more effective than placebo on improving symptoms of erectile dysfunction or serum total testosterone❞
As a performance-enhancer in sport
We’ll be brief here: it doesn’t seem to work and it may not be safe:
Insights into Supplements with Tribulus Terrestris used by Athletes
From sport, into general wellness?
Finally, a study that finds it may be useful for something!
❝Overall, participants supplemented with TT displayed significant improvements in lipid profile. Inflammatory and hematological biomarkers showed moderate beneficial effects with no significant changes on renal biomarkers. No positive effects were observed on the immune system response. Additionally, no TT-induced toxicity was reported.
In conclusion, there was no clear evidence of the beneficial effects of TT supplementation on muscle damage markers and hormonal behavior.❞
About those lipids…
Animal studies have shown that it may not only improve lipid profiles, but also may partially repair the endothelial dysfunction resulting from hyperlipidemia:
Want to try some?
In the unlikely event that today’s research review has inspired you with an urge to try Tribulus terrestris, here’s an example product on Amazon
If on the other hand you’d like to actually increase testosterone levels, then we suggest:
Topping Up Testosterone? ← a previous main feature did earlier this year
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What should I do if I can’t see a psychiatrist?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
People presenting at emergency with mental health concerns are experiencing the longest wait times in Australia for admission to a ward, according to a new report from the Australasian College of Emergency Medicine.
But with half of New South Wales’ public psychiatrists set to resign next week after ongoing pay disputes – and amid national shortages in the mental health workforce – Australians who rely on psychiatry support may be wondering where else to go.
If you can’t get in to see a psychiatrist and you need help, there are some other options. However in an emergency, you should call 000.
Why do people see a psychiatrist?
Psychiatrists are doctors who specialise in mental health and can prescribe medication.
People seek or require psychiatry support for many reasons. These may include:
- severe depression, including suicidal thoughts or behaviours
- severe anxiety, panic attacks or phobias
- post-traumatic stress disorder (PTSD)
- eating disorders, such as anorexia or bulimia
- attention deficit hyperactivity disorder (ADHD).
Psychiatrists complement other mental health clinicians by prescribing certain medications and making decisions about hospital admission. But when psychiatry support is not available a range of team members can contribute to a person’s mental health care.
Can my GP help?
Depending on your mental health concerns, your GP may be able to offer alternatives while you await formal psychiatry care.
GPs provide support for a range of mental health concerns, regardless of formal diagnosis. They can help address the causes and impact of issues including mental distress, changes in sleep, thinking, mood or behaviour.
The GP Psychiatry Support Line also provides doctors advice on care, prescription medication and how support can work.
It’s a good idea to book a long consult and consider taking a trusted person. Be explicit about how you’ve been feeling and what previous supports or medication you’ve accessed.
What about psychologists, counsellors or community services?
Your GP should also be aware of supports available locally and online.
For example, Head to Health is a government initiative, including information, a nationwide phone line, and in-person clinics in Victoria. It aims to improve mental health advice, assessment and access to treatment.
Medicare Mental Health Centres provide in-person care and are expanding across Australia.
There are also virtual care services in some areas. This includes advice on individualised assessment including whether to go to hospital.
Some community groups are led by peers rather than clinicians, such as Alternatives to Suicide.
How about if I’m rural or regional?
Accessing support in rural or regional areas is particularly tough.
Beyond helplines and formal supports, other options include local Suicide Prevention Networks and community initiatives such as ifarmwell and Men’s sheds.
Should I go to emergency?
As the new report shows, people who present at hospital emergency departments for mental health should expect long wait times before being admitted to a ward.
But going to a hospital emergency department will be essential for some who are experiencing a physical or mental health crisis.
Managing suicide-related distress
With the mass resignation of NSW psychiatrists looming, and amid shortages and blown-out emergency waiting times, people in suicide-related distress must receive the best available care and support.
Roughly nine Australians die by suicide each day. One in six have had thoughts of suicide at some point in their lives.
Suicidal thoughts can pass. There are evidence-based strategies people can immediately turn to when distressed and in need of ongoing care.
Safety planning is a popular suicide prevention strategy to help you stay safe.
What is a safety plan?
This is a personalised, step-by-step plan to remain safe during the onset or worsening of suicidal urges.
You can develop a safety plan collaboratively with a clinician and/or peer worker, or with loved ones. You can also make one on your own – many people like to use the Beyond Now app.
Safety plans usually include:
- recognising personal warning signs of a crisis (for example, feeling like a burden)
- identifying and using internal coping strategies (such as distracting yourself by listening to favourite music)
- seeking social supports for distraction (for example, visiting your local library)
- letting trusted family or friends know how you’re feeling – ideally, they should know they’re in your safety plan
- knowing contact details of specific mental health services (your GP, mental health supports, local hospital)
- making the environment safer by removing or limiting access to lethal means
- identifying specific and personalised reasons for living.
Our research shows safety planning is linked to reduced suicidal thoughts and behaviour, as well as feelings of depression and hopelessness, among adults.
Evidence from people with lived experience shows safety planning helps people to understand their warning signs and practice coping strategies.

Sharing your safety plan with loved ones may help understand warning signs of a crisis. Dragana Gordic/Shutterstock Are there helplines I can call?
There are people ready to listen, by phone or online chat, Australia-wide. You can try any of the following (most are available 24 hours a day, seven days a week):
Suicide helplines:
- Lifeline 13 11 14
- Suicide Call Back Service 1300 659 467
There is also specialised support:
- for men: MensLine Australia 1300 78 99 78
- children and young people: Kids’ Helpline 1800 55 1800
- Aboriginal and Torres Strait Islander people: 13YARN 13 92 76
- veterans and their families: Open Arms 1800 011 046
- LGBTQIA+ community: QLife 1300 184 527
- new and expecting parents: PANDA 1300 726 306
- people experiencing eating disorders: Butterfly Foundation 1800 33 4673.
Additionally, each state and territory will have its own list of mental health resources.
With uncertain access to services, it’s helpful to remember that there are people who care. You don’t have to go it alone.
Monika Ferguson, Senior Lecturer in Mental Health, University of South Australia and Nicholas Procter, Professor and Chair: Mental Health Nursing, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Amid Wildfire Trauma, L.A. County Dispatches Mental Health Workers to Evacuees
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
PASADENA, Calif. — As Fernando Ramirez drove to work the day after the Eaton Fire erupted, smoke darkened the sky, ash and embers rained onto his windshield, and the air smelled of melting rubber and plastic.
He pulled to the side of the road and cried at the sight of residents trying to save their homes.
“I could see people standing on the roof, watering it, trying to protect it from the fire, and they just looked so hopeless,” said Ramirez, a community outreach worker with the Pasadena Public Health Department.
That evening, the 49-year-old volunteered for a 14-hour shift at the city’s evacuation center, as did colleagues who had also been activated for emergency medical duty. Running on adrenaline and little sleep after finding shelter for homeless people all day, Ramirez spent the night circulating among more than a thousand evacuees, offering wellness checks, companionship, and hope to those who looked distressed.
Local health departments, such as Ramirez’s, have become a key part of governments’ response to wildfires, floods, and other extreme weather events, which scientists say are becoming more intense and frequent due to climate change. The emotional toll of fleeing and possibly losing a home can help cause or exacerbate mental health conditions such as anxiety, depression, post-traumatic stress disorder, suicidal ideation, and substance use, according to health and climate experts.
Wildfires have become a recurring experience for many Angelenos, making it difficult for people to feel safe in their home or able to go about daily living, said Lisa Wong, director of the Los Angeles County Department of Mental Health. However, with each extreme weather event, the county has improved its support for evacuees, she said.
For instance, Wong said the county deployed a team of mental health workers trained to comfort evacuees without retraumatizing them, including by avoiding asking questions likely to bring up painful memories. The department has also learned to better track people’s health needs and redirect those who may find massive evacuation settings uncomfortable to other shelters or interim housing, Wong said. In those first days, the biggest goal is often to reduce people’s anxiety by providing them with information.
“We’ve learned that right when a crisis happens, people don’t necessarily want to talk about mental health,” said Wong, who staffed the evacuation site Jan. 8 with nine colleagues.
Instead, she and her team deliver a message of support: “This is really bad right now, but you’re not going to do this alone. We have a whole system set up for recovery too. Once you get past the initial shock of what happened — initial housing needs, medication needs, all those things — then there’s this whole pathway to recovery that we set up.”
The convention center in downtown Pasadena, which normally hosts home shows, comic cons, and trade shows, was transformed into an evacuation site with hundreds of cots. It was one of at least 13 shelters opened to serve more than 200,000 residents under evacuation orders.
The January wildfires have burned an estimated 64 square miles — an area larger than the city of Paris — and destroyed at least 12,300 buildings since they started Jan. 7. AccuWeather estimates the region will likely face more than $250 billion in economic losses from the blazes, surpassing the estimates from the state’s record-breaking 2020 wildfire season.
Lisa Patel, executive director of the Medical Society Consortium on Climate and Health, said she’s most concerned about low-income residents, who are less likely to access mental health support.
“There was a mental health crisis even before the pandemic,” said Patel, who is also a clinical associate professor of pediatrics at Stanford School of Medicine, referring to the covid-19 pandemic. “The pandemic made it worse. Now you lace in all of this climate change and these disasters into a health care system that isn’t set up to care for the people that already have mental health illness.”
Early research suggests exposure to large amounts of wildfire smoke can damage the brain and increase the risk of developing anxiety, she added.
At the Pasadena Convention Center, Elaine Santiago sat on a cot in a hallway as volunteers pulled wagons loaded with soup, sandwiches, bottled water, and other necessities.
Santiago said she drew comfort from being at the Pasadena evacuation center, knowing that she wasn’t alone in the tragedy.
“It sort of gives me a sense of peace at times,” Santiago said. “Maybe that’s weird. We’re all experiencing this together.”
She had been celebrating her 78th birthday with family when she fled her home in the small city of Sierra Madre, east of Pasadena. As she watched flames whip around her neighborhood, she, along with children and grandkids, scrambled to secure their dogs in crates and grabbed important documents before they left.
The widower had leaned on her husband in past emergencies, and now she felt lost.
“I did feel helpless,” Santiago said. “I figured I’m the head of the household; I should know what to do. But I didn’t know.”
Donny McCullough, who sat on a neighboring green cot draped in a Red Cross blanket, had fled his Pasadena home with his family early on the morning of Jan. 8. Without power at home, the 68-year-old stayed up listening for updates on a battery-powered radio. His eyes remained red from smoke irritation hours later.
“I had my wife and two daughters, and I was trying not to show fear, so I quietly, inside, was like, ‘Oh my God,’” said McCullough, a music producer and writer. “I’m driving away, looking at the house, wondering if it’s going to be the last time I’m going to see it.”
He saved his master recording from a seven-year music project, but he left behind his studio with all his other work from a four-decade career in music.
Not all evacuees arrived with family. Some came searching for loved ones. That’s one of the hardest parts of his shift, Ramirez said. The community outreach worker helped walk people around the building, cot by cot.
A week in, at least two dozen people had been killed in the wildfires.
The work takes a toll on disaster relief workers too. Ramirez said many feared losing their homes in the fires and some already had. He attends therapy weekly, which he said helps him manage his emotions.
At the evacuation center, Ramirez described being on autopilot.
“Some of us react differently. I tend to go into fight mode,” Ramirez said. “I react. I run towards the fire. I run towards personal service. Then once that passes, that’s when my trauma catches up with me.”
Need help? Los Angeles County residents in need of support can call the county’s mental health helpline at 1-800-854-7771. The national Suicide & Crisis Lifeline, 988, is also available for those who’d like to speak with someone confidentially, free of charge.
This article was produced by KFF Health News, which publishes California Healthline, an editorially independent service of the California Health Care Foundation.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Share This Post
-
Beyond Castor: Vegetable Oils That Regenerate Your Skin
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Castor oil is very popular on social media, with enthusiastic advice to put it everywhere from your eyes to your vagina.
We did a main feature on it a little while ago, sorting out:
- what things does science actually say it’s good for,
- what things lack evidence, and
- what things go into the category of “wow definitely do not do that”?
Which body parts go into which category (according to the actual science) will probably surprise you: Castor Oil: All-Purpose Life-Changer, Or Snake Oil?
But what about other oils?
Time to get oiled up (but, correctly!)
Dr. Nina Poljšak and her research team were curious (as researchers often are), and investigated very closely (as in: under a microscope, not relying on nebulous before-and-after photos and hoping any difference was because of the oil) the effects of various oils and oil-constituting substances on the skin, specifically in the context of its regenerative ability.
Specifically, they tested the effects of seven vegetable oils (coconut, olive, linden, poppy, pomegranate, marigold, linseed) and their pure fatty acid or unsaponifiable components (unsaponifiable = you can’t make soap out of them; may seem a silly distinction here, but chemically speaking, it’s a useful way of sorting them, since the components that can’t be made into soap share certain properties, which are being looked at here), on skin’s keratinocytes and fibroblasts.
Even more specifically, they measured how each oil affects cell growth (proliferation) and cell movement (migration) in a wound‑healing test. The migration might sound like a strange thing to measure, but this is the means by which new skin cells replace old ones; in the human body, that means going from underneath to outside. They’re not just randomly going on tour or something (if they do, that’s cancer).
Here’s what they found!
The good:
- Poppy seed oil (high in linoleic acid) gave strong boosts to keratinocyte growth, especially at 0.1–0.15% concentration
- Marigold oil (high in calendic and linoleic acids) mildly improved growth of both cell types at similar doses
- Linden oil and linseed oils (especially high in essential fatty acids like linoleic and α‑linolenic acid) also promoted proliferation significantly
The bad:
- Olive oil (mostly oleic acid) slowed migration significantly and changed cell shapes
- Pomegranate seed oil (dominated by punicic acid) strongly inhibited both fibroblast and keratinocyte growth—even at low concentrations (0.01%)
The useless:
- Coconut oil (rich in lauric/myristic acids) showed no significant effect either way
- Unsaponifiable compounds were a mixed bag; some (such as β‑sitosterol or β‑carotene) helped keratinocyte growth; others (like squalene or ferulic acid) hindered fibroblasts; the conclusion the researchers drew here was that they add complexity but aren’t the main drivers of effects.
You can read the paper itself, here: Influence of vegetable oils and their constituents on in vitro human keratinocyte and fibroblast proliferation and migration
In summary…
If you’re looking for natural oils that gently boost skin cell renewal, go for oils high in linoleic acid—like poppy, marigold, linseed, or linden oils.
Skip the pomegranate seed oil (too inhibitory for regeneration in vitro), and be aware that oleic-rich oils like olive oil may cause subtle organizational effects in healing tissues, and slow the replacement of skin cells generally.
Olive oil is wonderful, but best kept to the kitchen: All About Olive Oil ← about its nutritional wonders and why it’s such a healthy oil
Want to learn more?
If you want an even simpler (not to mention: cheaper) approach:
“Slugging” Skin Care Routine (Tips From A Dermatologist)
Take care!
Share This Post



Related Posts
-

The Doctor Who Wants Us To Exercise Less, & Move More
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Today we’re talking about Dr. Rangan Chatterjee. He’s a medical doctor with decades of experience, and he wants us all to proactively stay in good health, rather than waiting for things to go wrong.
Great! What’s his deal?
Dr. Chatterjee advises that we take care of the following four pillars of good health:
- Relaxation
- Food
- Movement
- Sleep
And, they’re not in this order at random. Usually advice starts with diet and exercise, doesn’t it?
But for Dr. Chatterjee, it’s useless to try to tackle diet first if one is stressed-to-death by other things. As for food next, he knows that a good diet will fuel the next steps nicely. Speaking of next steps, a day full of movement is the ideal setup to a good night’s sleep—ready for a relaxing next day.
Relaxation
Here, Dr. Chatterjee advises that we go with what works for us. It could be meditation or yoga… Or it could be having a nice cup of tea while looking out of the window.
What’s most important, he says, is that we should take at least 15 minutes per day as “me time”, not as a reward for when we’ve done our work/chores/etc, but as something integrated into our routine, preferably early in the day.
Food
There are no grand surprises here: Dr. Chatterjee advocates for a majority plant-based diet, whole foods, and importantly, avoiding sugar.
He’s also an advocate of intermittent fasting, but only so far as is comfortable and practicable. Intermittent fasting can give great benefits, but it’s no good if that comes at a cost of making us stressed and suffering!
Movement
This one’s important. Well, they all are, but this one’s particularly characteristic to Dr. Chatterjee’s approach. He wants us to exercise less, and move more.
The reason for this is that strenuous exercise will tend to speed up our metabolism to the point that we will be prompted to eat high calorie quick-energy foods to compensate, and when we do, our body will rush to store that as fat, understanding (incorrectly) that we are in a time of great stress, because why else would we be exerting ourselves that much?
Instead, he advocates for building as much natural movement into our daily routine as possible. Walking more, taking the stairs, doing the gardening/housework.
That said, he does also advise some strength-training on a daily basis—bodyweight exercises like squats and lunges are top of his list.
Sleep
Here, aside from the usual “sleep hygiene” advices (dark cool room, fresh bedding, etc), he also advises we do as he does, and take an hour before bedtime as a purely wind-down time. In gentle lighting, perhaps reading (not on a bright screen!), for example.
Ready to start the next day, relaxed and ready to go.
If you’d like to know more about Dr. Chatterjee’s approach…
You can check out his:
If you don’t know where to start, we recommend the blog! It has a lot of guests there too, including Wim Hof, Gabor Maté, Mindy Pelz, and come to think of it, a lot of other people we’ve also featured ideas from previously!
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
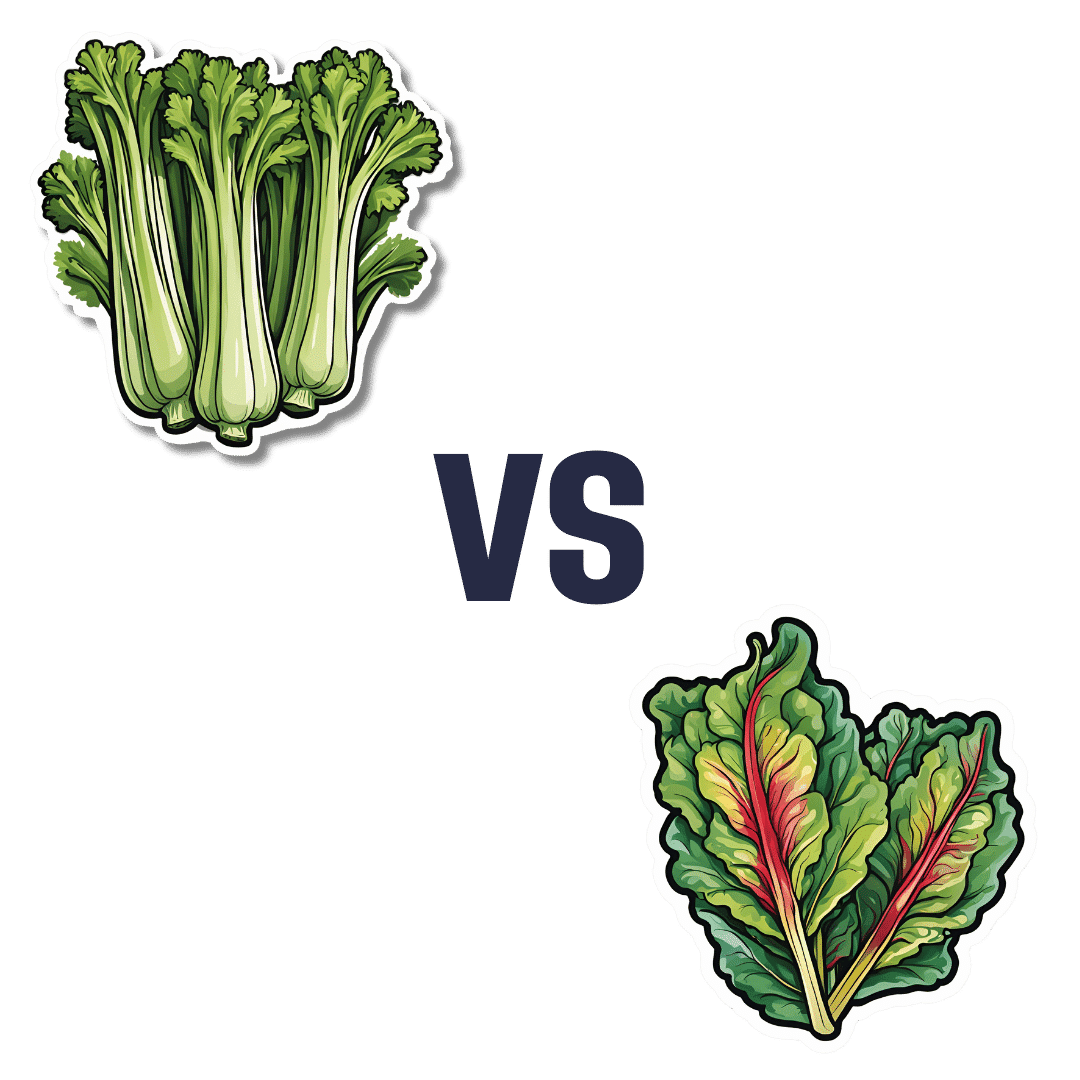
Celery vs Chard – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing celery to chard, we picked the chard.
Why?
In terms of macros, chard has more fiber, carbs, and protein, making it the more nutrient-dense option and thus the winner of the macros category.
In the category of vitamins, celery has more of vitamins B5 and B9, while chard has more of vitamins A, B1, B2, B3, B6, C, E, K, and choline—another win for chard.
When it comes to minerals, celery is not higher in any minerals, while chard has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. One more very clear win for chard!
Looking at polyphenols, celery has very little to boast, about 3mg/100g furanocoumarins and nothing else, while chard has an impressive array of polyphenols, with 9mg/100g kaempferol and 7.5mg/100g quercetin atop the list of 12 polyphenols. Yet another win for chard.
Adding up the sections is not difficult arithmetic today: chard sweeps every category. But by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Dr. Greger’s Daily Dozen ← the “dozen” in question includes getting a good amount of of leafy greens per day
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Superfood Pesto Pizza
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Not only is this pizza full of foods that punch above their weight healthwise, there’s no kneading and no waiting when it comes to the base, either. Homemade pizzas made easy!
You will need
For the topping:
- 1 zucchini, sliced
- 1 red bell pepper, cut into strips
- 3 oz mushrooms, sliced
- 3 shallots, cut into quarters
- 6 sun-dried tomatoes, roughly chopped
- ½ bulb garlic (paperwork done, but cloves left intact, unless they are very large, in which case halve them)
- 1 oz pitted black olives, halved
- 1 handful arugula
- 1 tbsp extra virgin olive oil
- 2 tsp black pepper, coarse ground
- ½ tsp MSG or 1 tsp low-sodium salt
For the base:
- ½ cup chickpea flour (also called besan or gram flour)
- 2 tsp extra virgin olive oil
- ½ tsp baking powder
- ⅛ tsp MSG or ¼ tsp low-sodium salt
For the pesto sauce:
- 1 large bunch basil, chopped
- ½ avocado, pitted and peeled
- 1 oz pine nuts
- ¼ bulb garlic, crushed
- 2 tbsp nutritional yeast
- 1 tsp black pepper
- Juice of ½ lemon
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 400℉ / 200℃.
2) Toss the zucchini, bell pepper, mushrooms, shallots, and garlic cloves in 1 tbsp olive oil, ensuring an even coating. Season with the black pepper and MSG/salt, and put on a baking tray lined with baking paper, to roast for about 20 minutes, until they are slightly charred.
3) When the vegetables are in the oven, make the pizza base by combining the dry ingredients in a bowl, making a pit in the middle of it, adding the olive oil and whisking it in, and then slowly (i.e., a little bit at a time) whisking in 1 cup cold water. This should take under 5 minutes.
4) Don’t panic when this doesn’t become a dough; it is supposed to be a thick batter, so that’s fine. Pour it into a 9″ pizza pan, and bake for about 15 minutes, until firm. Rotate it if necessary partway through; whether it needs this or not will depend on your oven.
5) While the pizza base is in the oven, make the pesto sauce by blending all the pesto sauce ingredients in a high-speed blender until smooth.
6) When the base and vegetables are ready (these should be finished around the same time), spread the pesto sauce on the base, scatter the arugula over it followed by the vegetables and then the olives and sun-dried tomatoes.
7) Serve, adding any garnish or other final touches that take your fancy.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Which Bell Peppers To Pick? A Spectrum Of Specialties
- Ergothioneine In Mushrooms: “The Longevity Vitamin” (That’s Not A Vitamin)
- Black Olives vs Green Olives – Which is Healthier
- Lycopene’s Benefits For The Gut, Heart, Brain, & More
- Coconut vs Avocado – Which is Healthier?
- Herbs for Evidence-Based Health & Healing
- Spermidine For Longevity
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: