The Epigenetics Revolution – by Dr. Nessa Carey
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you enjoyed the book “Inheritance” that we reviewed a couple of days ago, you might love this as a “next read” book. But you can also just dive straight in here, if you like!
This one, as the title suggests, focuses entirely on epigenetics—how our life events can shape our genetic expression, and that of our descendants. Or to look at it in the other direction, how our genetic expression can be shaped by the life experiences of, for example, our grandparents.
The style of this book is very much pop-science, but contains a lot of information from hard science throughout. We learn not just about longitudinal population studies as one might expect, but also about the intricacies of DNA methylation and histone modifications, for example.
Depending on your outlook, you may find some of this very bleak (“great, I am shackled by what my grandparents did”) or very optimism-inducing (“oh wow, I’m not nearly so constrained by genetics as I thought; this stuff is so malleable!”). This is also the same author who wrote “Hacking The Code of Life“, by the way, but we’ll review that another day.
Bottom line: this book is the best one-shot primer on epigenetics that this reviewer has read (you may be wondering how many that is, and the answer is… about seven or so? I’m not good at counting).
Click here to check out The Epigenetics Revolution, and learn how dynamic you really are!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

I’m feeling run down. Why am I more likely to get sick? And how can I boost my immune system?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It has been a long winter, filled with many viruses and cost-of-living pressures, on top of the usual mix of work, study, life admin and caring responsibilities.
Stress is an inevitable part of life. In short bursts, our stress response has evolved as a survival mechanism to help us be more alert in fight or flight situations.
But when stress is chronic, it weakens the immune system and makes us more vulnerable to illnesses such as the common cold, flu and COVID.

Pexels/Ketut Subiyanto Stress makes it harder to fight off viruses
When the immune system starts to break down, a virus that would normally have been under control starts to flourish.
Once you begin to feel sick, the stress response rises, making it harder for the immune system to fight off the disease. You may be sick more often and for longer periods of time, without enough immune cells primed and ready to fight.
In the 1990s, American psychology professor Sheldon Cohen and his colleagues conducted a number of studies where healthy people were exposed to an upper respiratory infection, through drops of virus placed directly into their nose.
These participants were then quarantined in a hotel and monitored closely to determine who became ill.
One of the most important factors predicting who got sick was prolonged psychological stress.
Cortisol suppresses immunity
“Short-term stress” is stress that lasts for a period of minutes to hours, while “chronic stress” persists for several hours per day for weeks or months.
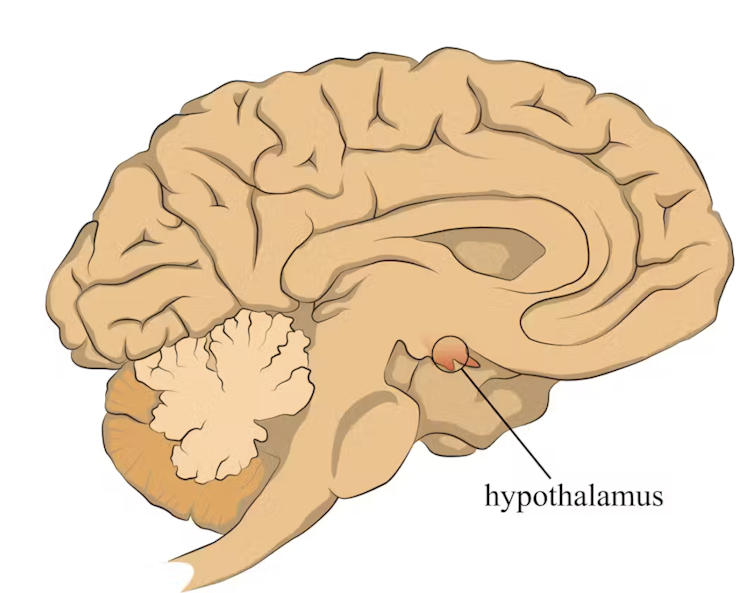
When faced with a perceived threat, psychological or physical, the hypothalamus region of the brain sets off an alarm system. This signals the release of a surge of hormones, including adrenaline and cortisol.
The hypothalamus sets off an alarm system in response to a real or perceived threat. stefan3andrei/Shutterstock In a typical stress response, cortisol levels quickly increase when stress occurs, and then rapidly drop back to normal once the stress has subsided. In the short term, cortisol suppresses inflammation, to ensure the body has enough energy available to respond to an immediate threat.
But in the longer term, chronic stress can be harmful. A Harvard University study from 2022 showed that people suffering from psychological distress in the lead up to their COVID infection had a greater chance of experiencing long COVID. They classified this distress as depression, probable anxiety, perceived stress, worry about COVID and loneliness.
Those suffering distress had close to a 50% greater risk of long COVID compared to other participants. Cortisol has been shown to be high in the most severe cases of COVID.
Stress causes inflammation
Inflammation is a short-term reaction to an injury or infection. It is responsible for trafficking immune cells in your body so the right cells are present in the right locations at the right times and at the right levels.
The immune cells also store a memory of that threat to respond faster and more effectively the next time.
Initially, circulating immune cells detect and flock to the site of infection. Messenger proteins, known as pro-inflammatory cytokines, are released by immune cells, to signal the danger and recruit help, and our immune system responds to neutralise the threat.
During this response to the infection, if the immune system produces too much of these inflammatory chemicals, it can trigger symptoms such as nasal congestion and runny nose.
Our immune response can trigger symptoms such as a runny nose. Alyona Mandrik/Shutterstock What about chronic stress?
Chronic stress causes persistently high cortisol secretion, which remains high even in the absence of an immediate stressor.
The immune system becomes desensitised and unresponsive to this cortisol suppression, increasing low-grade “silent” inflammation and the production of pro-inflammatory cytokines (the messenger proteins).
Immune cells become exhausted and start to malfunction. The body loses the ability to turn down the inflammatory response.
Over time, the immune system changes the way it responds by reprogramming to a “low surveillance mode”. The immune system misses early opportunities to destroy threats, and the process of recovery can take longer.
So how can you manage your stress?
We can actively strengthen our immunity and natural defences by managing our stress levels. Rather than letting stress build up, try to address it early and frequently by:
1) Getting enough sleep
Getting enough sleep reduces cortisol levels and inflammation. During sleep, the immune system releases cytokines, which help fight infections and inflammation.
2) Taking regular exercise
Exercising helps the lymphatic system (which balances bodily fluids as part of the immune system) circulate and allows immune cells to monitor for threats, while sweating flushes toxins. Physical activity also lowers stress hormone levels through the release of positive brain signals.
3) Eating a healthy diet
Ensuring your diet contains enough nutrients – such as the B vitamins, and the full breadth of minerals like magnesium, iron and zinc – during times of stress has a positive impact on overall stress levels. Staying hydrated helps the body to flush out toxins.
4) Socialising and practising meditation or mindfulness
These activities increase endorphins and serotonin, which improve mood and have anti-inflammatory effects. Breathing exercises and meditation stimulate the parasympathetic nervous system, which calms down our stress responses so we can “reset” and reduce cortisol levels.
Sathana Dushyanthen, Academic Specialist & Lecturer in Cancer Sciences & Digital Health| Superstar of STEM| Science Communicator, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Goji Berries vs Pomegranate – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing goji berries to pomegranate, we picked the goji berries.
Why?
Both fruits with substantial phytochemical benefits, but…
In terms of macros, goji berries have a lot more protein, carbs, and fiber, the ratio of which latter two brings the glycemic index to the same place as pomegranate’s—specifically, that eating either of these will not raise a person’s blood glucose levels. We thus call this a win for goji berries, as the “more food per food” option.
In the category of vitamins, goji berries have a lot more of vitamins A, B3, B6, and C, while pomegranate is not higher in any vitamins.
When it comes to minerals, goji berries have more calcium, iron, magnesium, selenium, and zinc, while pomegranate has more copper. Another win for goji berries here.
With regard to those phytochemical benefits we talked about; it’s worth noting that they come in abundance in goji berries, while in pomegranates, most of the benefits are in the peel, not the flesh/seeds that people most often eat. So, again goji berries win.
Adding up the sections makes for an easy win for goji berries today.
Want to learn more?
You might like to read:
- Goji Berries: Which Benefits Do They Really Have?
- The Sugary Food That Lowers Blood Sugars ← this is about goji berries
- Pomegranate’s Health Gifts Are Mostly In Its Peel
Take care!
Share This Post
-

Antibiotics? Think Thrice
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Antibiotics: Useful Even Less Often Than Previously Believed (And Still Just As Dangerous)
You probably already know that antibiotics shouldn’t be taken unless absolutely necessary. Not only does taking antibiotics frivolously increase antibiotic resistance (which is bad, and kills people), but also…
It’s entirely possible for the antibiotics to not only not help, but instead wipe out your gut’s “good bacteria” that were keeping other things in check.
Those “other things” can include fungi like Candida albicans.
Candida, which we all have in us to some degree, feeds on sugar (including the sugar formed from breaking down alcohol, by the way) and refined carbs. Then it grows, and puts its roots through your intestinal walls, linking with your neural system. Then it makes you crave the very things that will feed it and allow it to put bigger holes in your intestinal walls.
Don’t believe us? Read: Candida albicans-Induced Epithelial Damage Mediates Translocation through Intestinal Barriers
(That’s scientist-speak for “Candida puts holes in your intestines, and stuff can then go through those holes”)
And as for how that comes about, it’s like we said:
See also: Candida albicans as a commensal and opportunistic pathogen in the intestine
That’s not all…
And that’s just C. albicans, never mind things like C. diff. that can just outright kill you easily.
We don’t have room to go into everything here, but you might like to check out:
Four Ways Antibiotics Can Kill You
It gets worse (now comes the new news)
So, what are antibiotics good for? Surely, for clearing up chesty coughs, lower respiratory tract infections, right? It’s certainly one of the two things that antibiotics are most well-known for being good at and often necessary for (the other being preventing/treating sepsis, for example in serious and messy wounds).
But wait…
A large, nationwide (US) observational study of people who sought treatment in primary or urgent care settings for lower respiratory tract infections found…
(drumroll please)
…the use of antibiotics provided no measurable impact on the severity or duration of coughs even if a bacterial infection was present.
Read for yourself:
And in the words of the lead author of that study,
❝Lower respiratory tract infections tend to have the potential to be more dangerous, since about 3% to 5% of these patients have pneumonia. But not everyone has easy access at an initial visit to an X-ray, which may be the reason clinicians still give antibiotics without any other evidence of a bacterial infection.❞
So, what’s to be done about this? On a large scale, Dr. Merenstein recommends:
❝Serious cough symptoms and how to treat them properly needs to be studied more, perhaps in a randomized clinical trial as this study was observational and there haven’t been any randomized trials looking at this issue since about 2012.❞
This does remind us that, while not a RCT, there is a good ongoing observational study that everyone with a smartphone can participate in:
Dr. Peter Small’s medical AI: “The Cough Doctor”
In the meantime, he advises that when COVID and SARS have been ruled out, then “basic symptom-relieving medications plus time brings a resolution to most people’s infections”.
You can read a lot more detail here:
Antibiotics aren’t effective for most lower tract respiratory infections
In summary…
Sometimes, antibiotics really are a necessary and life-saving medication. But most of the time they’re not, and given their great potential for harm, they may be best simultaneously viewed as the very dangerous threat they also are, and used only when those “heavy guns” are truly what’s required.
Take care!
Share This Post


Related Posts
-

Butter vs Ghee – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing butter to ghee, we picked the butter.
Why?
Assuming a comparable source for each—e.g. butter from grass-fed cows, or ghee made from butter from grass-fed cows—both have a mostly comparable nutritional profile.
Note: the above is not a safe assumption to make in the US, unless you’re paying attention. Grass-fed cows are not the norm in the US, so it’s something that has to be checked for. On the other hand, ghee is usually imported, and grass-fed cows are the norm in most of the rest of the world, including the countries that export ghee the most. So if “buying blind”, ghee will be the safer bet. However, checking labels can overcome this.
Many of the Internet-popular health claims for ghee are exaggerated. For example, yes it contains butyrate… But at 1% or less. You’d be better off getting your butyrate from fibrous fruit and vegetables. Yes it contains medium-chain triglycerides (that’s also good), but in trace amounts. It even has conjugated linoleic acid, but you guessed it, the dose is insignificant.
Meanwhile, both butter and ghee contain heart-unhealthy animal-based saturated fats (which are usually worse for the health than some, but not all, of their plant-based equivalents). However…
- A tablespoon of butter contains about 7 grams of saturated fat
- A tablespoon of ghee contains about 9 grams of saturated fat
So, in this case, “ghee is basically butter, but purer” becomes a bad thing (and the deciding factor between the two).
There is one reason to choose butter over ghee, but it’s not health-related—it simply has a higher smoke point, as is often the case for fats that have been more processed compared to fats that have been less processed.
In short: either can be used in moderation, but even 2 tbsp of butter are taking an average person (because it depends on your metabolism, so we’ll say average) to the daily limit for saturated fats already, so we recommend to go easy even on that.
Want to know more?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
5 Golden Rules To Lose Belly Fat
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our belly is often the first place we gain fat and the last to lose it—due to hormonal changes, poor blood flow, and fat cell types. This also means that weight loss efforts can result in it looking worse before it looks better, as we lose weight from elsewhere around it. But, there is a way forwards:
What to do about it
Cori Lefkowith, of “Redefining Strength” and “Strength At Any Age” fame, advise that we follow the following “5 golden rules”:
- Mindset: avoid “All or Nothing” thinking; focus on small, sustainable changes and consistent habits.
- Macros: prioritize protein (40%+ of calories), balance fats and carbs for hormonal health, and avoid extreme calorie deficits (your body will try to save you from starvation by slowing your metabolism to conserve energy, and storing fat).
- Nutrition quality: focus on whole, nutrient-dense foods for better satiety, gut health, and energy. Get plenty of fiber and water; your body still needs those too.
- Muscle building: strength training preserves muscle, boosts metabolism, and improves body composition—don’t ditch your strength training for cardio; it won’t help and that swap would hinder..
- Daily walks: 15–20 minutes of walking after dinner aids digestion, and reduces stress (remember: stress invites your body to store extra fat, especially at the belly). It also incidentally burns calories without stressing the body, but honestly, it’s really not very many calories, so that’s not the main reason to do it.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Visceral Belly Fat & How To Lose It ← this is not the same thing as subcutaneous fat; the remedy is partly the same though, and it’s important to do both if you’re carrying excess weight both on your belly and in your viscera, if you want to reduce your overall waist size.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
30 Days Of Weight Vest Use: Lessons Learned
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Robin, from “The Science of Self-Care”, has insights:
How to have an easier time of it
Per peer-reviewed science (linked under the video on YouTube), there are some benefits:
- Cardiovascular fitness: increases workout intensity, improving heart and lung health.
- Muscle strength & endurance: strengthens core, legs, glutes, and calves.
- Bone density: helps prevent osteoporosis through weight-bearing exercise.
- Caloric expenditure: burns more calories, aiding in weight loss.
- Balance & posture: improves balance, though posture effects were mixed.
She chose a 30 lb weighted vest, which felt much heavier than expected. Initially, this was uncomfortable but became comforting over time (much like a weighted blanket). She also found that walks became noticeably more intense, leading to increased sweating and hunger.
Over the course of the month, she found:
- Week 1: adjusting to the extra weight; walks felt significantly harder.
- Weeks 2-3: strength improvements; carrying groceries felt easier, walking without the vest felt effortless.
- Week 3: started craving the weighted vest, but also began experiencing shoulder discomfort.
- Week 4: reduced walk duration to 20 minutes due to shoulder strain.
She concluded that the vest design was flawed—all weight rested on shoulders instead of distributing across the body, which led to shoulder discomfort and posture issues. To mitigate these things, she switched to wearing the vest around the waist like a skirt. She now plans to try a weighted belt for better weight distribution, though also simply a different kind of vest would work better (the kind that looks like combat body armor distributes the weight a lot more easily)
In short, her verdict:
- Weighted walking: 10/10, highly beneficial and easy to incorporate into daily routines.
- Vest used: 2/10, poor weight distribution, causing discomfort and shoulder strain.
For more on all of this, plus links to the relevant scientific papers, enjoy:

Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Weight Vests Against Osteoporosis: Do They Really Build Bone?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: