The Age-Proof Brain – by Dr. Marc Milstein
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Biological aging is not truly just one thing, but rather the amalgam of many things intersecting—and most of them are modifiable. The cells of your body neither know nor care how many times you have flown around the sun; they just respond to the stimuli they’re given.
Which is what fuels this book. The idea is to have a brain that is less-assailed by the things that would make it age, and more rejuvenated by the things that can make it biologically younger.
Dr. Milstein doesn’t neglect the rest of the body, and indeed notes the brain’s connections with the immune system, the heart, the gut, and more. But everything in this book is done with the brain in mind and its good health as the top priority outcome of all the things he advises.
On which note, yes, there is plenty of practical, implementable advice here. For a book that is consistently full of study paper citations, he does take care to make everything useful to the reader, and makes everything as easy as possible for the layperson along the way.
Bottom line: if you would like your brain to age less, this is an excellent, very evidence-based, guidebook.
Click here to check out The Age-Proof Brain, and age-proof your brain!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Cancer Journey – by Dr. Chadi Nabhan

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
After a brief introduction of what cancer actually is and what causes it, the layout of the rest of the book is in chronological order of patient experience, that is to say, what to expect during the journey from screening and diagnosis, to one’s first oncology visit (the author being an oncologist himself), how cancer staging works, getting second opinions, and a chapter-by-chapter review of many different treatment options, ranging from surgery and chemotherapy, to radiation and hormonal therapies, and even more modern targeted therapies, immunotherapy, cellular therapies, and yes, complementary and alternative therapies, amongst others we haven’t listed for the sake of brevity.
He doesn’t leave it there though; he also talks managing side effects, monitoring for recurrence, and even caring for the caregiver(s), along with eventual survivorship and that emotional journey, or if it comes down to it, palliative and hospice care.
Finishing on a hopeful note, he also brings attention to novel approaches that are being trialled presently, and the prospects for the near future of cancer care.
The style is very human and readable, notwithstanding that the author has hundreds of peer-reviewed publications to his name, the content here is presented in a much more approachable, less clinical way, while still conveying all the information that needs to be conveyed.
Bottom line: if you or a loved one is facing cancer, this book will be an invaluable resource.
Click here to check out The Cancer Journey, and understand each part of it!
Share This Post
-

How to Vary Breakfast for Digestion?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Would appreciate your thoughts on how best to promote good digestion. For years, my breakfast has consisted of flaxseeds, sunflower seeds, and almonds – all well ground up – eaten with a generous amount of kefir. This works a treat as far as my digestion is concerned. But I sometimes wonder whether it would be better for my health if I varied or supplemented this breakfast. How might I do this without jeopardising my good digestion?❞
Sounds like you’re already doing great! Those ingredients are all very nutrient-dense, and grinding them up improves digestion greatly, to the point that you’re getting nutrients your body couldn’t get at otherwise. And the kefir, of course, is a top-tier probiotic.
Also, you’re getting plenty of protein and healthy fats in with your carbs, which results in the smoothest blood sugar curve.
As for variety…
Variety is good in diet, but variety within a theme. Our gut microbiota change according to what we eat, so sudden changes in diet are often met with heavy resistance from our gut.
- For example, people who take up a 100% plant-based diet overnight often spend the next day in the bathroom, and wonder what happened.
- Conversely, a long-time vegan who (whether by accident or design) consumes meat or dairy will likely find themself quickly feeling very unwell, because their gut microbiota have no idea what to do with this.
So, variety yes, but within a theme, and make any changes gradual for the easiest transition.
All in all, the only obvious suggestion for improvement is to consider adding some berries. These can be fresh, dried, or frozen, and will confer many health benefits (most notably a lot of antioxidant activity).
Enjoy!
Share This Post
-

Wheat Belly, Revised & Expanded Edition – by Dr. William Davis
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This review pertains to the 2019 edition of the book, not the 2011 original, which will not have had all of the same research.
We are told, by scientific consensus, to enjoy plenty of whole grains as part of our diet. So, what does cardiologist Dr. William Davis have against wheat?
Firstly, not all grains are interchangeable, and wheat—in particular, modern strains of wheat—cannot be described as the same as the wheat of times past.
While this book does touch on the gluten aspect (and Celiac disease), and notes that modern wheat has a much higher gluten content than older strains, most of this book is about other harms that wheat can do to us.
Dr. Davis explores and explains the metabolic implications of wheat’s unique properties on organs such as our pancreas, liver, heart, and brain.
The book does also have recipes and meal plans, though in this reviewer’s opinion they were a little superfluous. Wheat is not hard to cut out unless you are living in a food desert or are experiencing food poverty, in which case, those recipes and meal plans would also not help.
Bottom line: this book, filled with plenty of actual science, makes a strong case against wheat, and again, mostly for reasons other than its gluten content. You might want to cut yours down!
Click here to check out Wheat Belly, and see if skipping the wheat could be good for you!
Share This Post
Related Posts
-

Our blood-brain barrier stops bugs and toxins getting to our brain. Here’s how it works
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our brain is an extremely complex and delicate organ. Our body fiercely protects it by holding onto things that help it and keeping harmful things out, such as bugs that can cause infection and toxins.
It does that though a protective layer called the blood-brain barrier. Here’s how it works, and what it means for drug design.

The Conversation, Rattiya Thongdumhyu/Shutterstock, Petr Ganaj/Pexels First, let’s look at the circulatory system
Adults have roughly 30 trillion cells in their body. Every cell needs a variety of nutrients and oxygen, and they produce waste, which needs to be taken away.
Our circulatory system provides this service, delivering nutrients and removing waste.
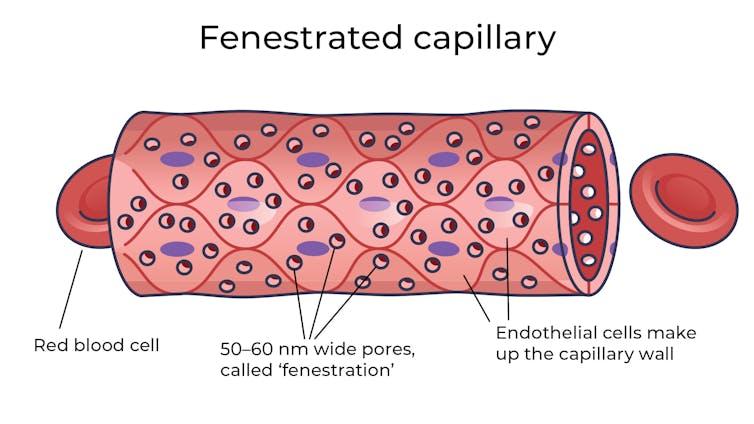
Fenestrated capillaries let nutrients and waste pass through. Vectormine/Shutterstock Where the circulatory system meets your cells, it branches down to tiny tubes called capillaries. These tiny tubes, about one-tenth the width of a human hair, are also made of cells.
But in most capillaries, there are some special features (known as fenestrations) that allow relatively free exchange of nutrients and waste between the blood and the cells of your tissues.
It’s kind of like pizza delivery
One way to think about the way the circulation works is like a pizza delivery person in a big city. On the really big roads (vessels) there are walls and you can’t walk up to the door of the house and pass someone the pizza.
But once you get down to the little suburban streets (capillaries), the design of the streets means you can stop, get off your scooter and walk up to the door to deliver the pizza (nutrients).
We often think of the brain as a spongy mass without much blood in it. In reality, the average brain has about 600 kilometres of blood vessels.
The difference between the capillaries in most of the brain and those elsewhere is that these capillaries are made of specialised cells that are very tightly joined together and limit the free exchange of anything dissolved in your blood. These are sometimes called continuous capillaries.
Continuous capillaries limit the free exchange of anything dissolved in your blood. Vectormine/Shutterstock This is the blood brain barrier. It’s not so much a bag around your brain stopping things from getting in and out but more like walls on all the streets, even the very small ones.
The only way pizza can get in is through special slots and these are just the right shape for the pizza box.
The blood brain barrier is set up so there are specialised transporters (like pizza box slots) for all the required nutrients. So mostly, the only things that can get in are things that there are transporters for or things that look very similar (on a molecular scale).
The analogy does fall down a little bit because the pizza box slot applies to nutrients that dissolve in water. Things that are highly soluble in fat can often bypass the slots in the wall.
Why do we have a blood-brain barrier?
The blood brain barrier is thought to exist for a few reasons.
First, it protects the brain from toxins you might eat (think chemicals that plants make) and viruses that often can infect the rest of your body but usually don’t make it to your brain.
It also provides protection by tightly regulating the movement of nutrients and waste in and out, providing a more stable environment than in the rest of the body.
Lastly, it serves to regulate passage of immune cells, preventing unnecessary inflammation which could damage cells in the brain.
What it means for medicines
One consequence of this tight regulation across the blood brain barrier is that if you want a medicine that gets to the brain, you need to consider how it will get in.
There are a few approaches. Highly fat-soluble molecules can often pass into the brain, so you might design your drug so it is a bit greasy.
The blood-brain barrier stops many medicines getting into the brain. Ron Lach/Pexels Another option is to link your medicine to another molecule that is normally taken up into the brain so it can hitch a ride, or a “pro-drug”, which looks like a molecule that is normally transported.
Using it to our advantage
You can also take advantage of the blood brain barrier.
Opioids used for pain relief often cause constipation. They do this because their target (opioid receptors) are also present in the nervous system of the intestines, where they act to slow movement of the intestinal contents.
Imodium (Loperamide), which is used to treat diarrhoea, is actually an opioid, but it has been specifically designed so it can’t cross the blood brain barrier.
This design means it can act on opioid receptors in the gastrointestinal tract, slowing down the movement of contents, but does not act on brain opioid receptors.
In contrast to Imodium, Ozempic and Victoza (originally designed for type 2 diabetes, but now popular for weight-loss) both have a long fat attached, to improve the length of time they stay in the body.
A consequence of having this long fat attached is that they can cross the blood-brain barrier, where they act to suppress appetite. This is part of the reason they are so effective as weight-loss drugs.
So while the blood brain barrier is important for protecting the brain it presents both a challenge and an opportunity for development of new medicines.
Sebastian Furness, ARC Future Fellow, School of Biomedical Sciences, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why do I poo in the morning? A gut expert explains
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
No, you’re not imagining it. People really are more likely to poo in the morning, shortly after breakfast. Researchers have actually studied this.
But why mornings? What if you tend to poo later in the day? And is it worth training yourself to be a morning pooper?
To understand what makes us poo when we do, we need to consider a range of factors including our body clock, gut muscles and what we have for breakfast.
Here’s what the science says.
H_Ko/Shutterstock So morning poos are real?
In a UK study from the early 1990s, researchers asked nearly 2,000 men and women in Bristol about their bowel habits.
The most common time to poo was in the early morning. The peak time was 7-8am for men and about an hour later for women. The researchers speculated that the earlier time for men was because they woke up earlier for work.
About a decade later, a Chinese study found a similar pattern. Some 77% of the almost 2,500 participants said they did a poo in the morning.
But why the morning?
There are a few reasons. The first involves our circadian rhythm – our 24-hour internal clock that helps regulate bodily processes, such as digestion.
For healthy people, our internal clock means the muscular contractions in our colon follow a distinct rhythm.
There’s minimal activity in the night. The deeper and more restful our sleep, the fewer of these muscle contractions we have. It’s one reason why we don’t tend to poo in our sleep.
Your lower gut is a muscular tube that contracts more strongly at certain times of day. Vectomart/Shutterstock But there’s increasing activity during the day. Contractions in our colon are most active in the morning after waking up and after any meal.
One particular type of colon contraction partly controlled by our internal clock are known as “mass movements”. These are powerful contractions that push poo down to the rectum to prepare for the poo to be expelled from the body, but don’t always result in a bowel movement. In healthy people, these contractions occur a few times a day. They are more frequent in the morning than in the evening, and after meals.
Breakfast is also a trigger for us to poo. When we eat and drink our stomach stretches, which triggers the “gastrocolic reflex”. This reflex stimulates the colon to forcefully contract and can lead you to push existing poo in the colon out of the body. We know the gastrocolic reflex is strongest in the morning. So that explains why breakfast can be such a powerful trigger for a bowel motion.
Then there’s our morning coffee. This is a very powerful stimulant of contractions in the sigmoid colon (the last part of the colon before the rectum) and of the rectum itself. This leads to a bowel motion.
How important are morning poos?
Large international surveys show the vast majority of people will poo between three times a day and three times a week.
This still leaves a lot of people who don’t have regular bowel habits, are regular but poo at different frequencies, or who don’t always poo in the morning.
So if you’re healthy, it’s much more important that your bowel habits are comfortable and regular for you. Bowel motions do not have to occur once a day in the morning.
Morning poos are also not a good thing for everyone. Some people with irritable bowel syndrome feel the urgent need to poo in the morning – often several times after getting up, during and after breakfast. This can be quite distressing. It appears this early-morning rush to poo is due to overstimulation of colon contractions in the morning.
Can you train yourself to be regular?
Yes, for example, to help treat constipation using the gastrocolic reflex. Children and elderly people with constipation can use the toilet immediately after eating breakfast to relieve symptoms. And for adults with constipation, drinking coffee regularly can help stimulate the gut, particularly in the morning.
A disturbed circadian rhythm can also lead to irregular bowel motions and people more likely to poo in the evenings. So better sleep habits can not only help people get a better night’s sleep, it can help them get into a more regular bowel routine.
A regular morning coffee can help relieve constipation. Caterina Trimarchi/Shutterstock Regular physical activity and avoiding sitting down a lot are also important in stimulating bowel movements, particularly in people with constipation.
We know stress can contribute to irregular bowel habits. So minimising stress and focusing on relaxation can help bowel habits become more regular.
Fibre from fruits and vegetables also helps make bowel motions more regular.
Finally, ensuring adequate hydration helps minimise the chance of developing constipation, and helps make bowel motions more regular.
Monitoring your bowel habits
Most of us consider pooing in the morning to be regular. But there’s a wide variation in normal so don’t be concerned if your poos don’t follow this pattern. It’s more important your poos are comfortable and regular for you.
If there’s a major change in the regularity of your bowel habits that’s concerning you, see your GP. The reason might be as simple as a change in diet or starting a new medication.
But sometimes this can signify an important change in the health of your gut. So your GP may need to arrange further investigations, which could include blood tests or imaging.
Vincent Ho, Associate Professor and clinical academic gastroenterologist, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

America Worries About Health Costs — And Voters Want to Hear From Biden and Republicans
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
President Joe Biden is counting on outrage over abortion restrictions to help drive turnout for his reelection. Former President Donald Trump is promising to take another swing at repealing Obamacare.
But around America’s kitchen tables, those are hardly the only health topics voters want to hear about in the 2024 campaigns. A new KFF tracking poll shows that health care tops the list of basic expenses Americans worry about — more than gas, food, and rent. Nearly 3 in 4 adults — and majorities of both parties — say they’re concerned about paying for unexpected medical bills and other health costs.
“Absolutely health care is something on my mind,” Rob Werner, 64, of Concord, New Hampshire, said in an interview at a local coffee shop in January. He’s a Biden supporter and said he wants to make sure the Affordable Care Act, also known as Obamacare, is retained and that there’s more of an effort to control health care costs.
The presidential election is likely to turn on the simple question of whether Americans want Trump back in the White House. (Nikki Haley, the former South Carolina governor and U.S. ambassador to the United Nations, remained in the race for the Republican nomination ahead of Super Tuesday, though she had lost the first four primary contests.) And neither major party is basing their campaigns on health care promises.
But in the KFF poll, 80% of adults said they think it’s “very important” to hear presidential candidates talk about what they’d do to address health care costs — a subject congressional and state-level candidates can also expect to address.
“People are most concerned about out-of-pocket expenses for health care, and rightly so,” said Andrea Ducas, vice president of health policy at the Center for American Progress, a Washington, D.C.-based progressive think tank.
Here’s a look at the major health care issues that could help determine who wins in November.
Abortion
Less than two years after the Supreme Court overturned the constitutional right to an abortion, it is shaping up to be the biggest health issue in this election.
That was also the case in the 2022 midterm elections, when many voters rallied behind candidates who supported abortion rights and bolstered Democrats to an unexpectedly strong showing. Since the Supreme Court’s decision, voters in six states — including Kansas, Kentucky, and Ohio, where Republicans control the legislatures — have approved state constitutional amendments protecting abortion access.
Polls show that abortion is a key issue to some voters, said Robert Blendon, a public opinion researcher and professor emeritus at the Harvard T.H. Chan School of Public Health. He said up to 30% across the board see it as a “personal” issue, rather than policy — and most of those support abortion rights.
“That’s a lot of voters, if they show up and vote,” Blendon said.
Proposals to further protect — or restrict — abortion access could drive voter turnout. Advocates are working to put abortion-related measures on the ballot in such states as Arizona, Florida, Missouri, and South Dakota this November. A push in Washington toward a nationwide abortion policy could also draw more voters to the polls, Blendon said.
A surprise ruling by the Alabama Supreme Court in February that frozen embryos are children could also shake up the election. It’s an issue that divides even the anti-abortion community, with some who believe that a fertilized egg is a unique new person deserving of full legal rights and protections, and others believing that discarding unused embryos as part of the in vitro fertilization process is a morally acceptable way for couples to have children.
Pricey Prescriptions
Drug costs regularly rank high among voters’ concerns.
In the latest tracking poll, more than half — 55% — said they were very worried about being able to afford prescription drugs.
Biden has tried to address the price of drugs, though his efforts haven’t registered with many voters. While its name doesn’t suggest landmark health policy, the Inflation Reduction Act, or IRA, which the president signed in August 2022, included a provision allowing Medicare to negotiate prices for some of the most expensive drugs. It also capped total out-of-pocket spending for prescription drugs for all Medicare patients, while capping the price of insulin for those with diabetes at $35 a month — a limit some drugmakers have extended to patients with other kinds of insurance.
Drugmakers are fighting the Medicare price negotiation provision in court. Republicans have promised to repeal the IRA, arguing that forcing drugmakers to negotiate lower prices on drugs for Medicare beneficiaries would amount to price controls and stifle innovation. The party has offered no specific alternative, with the GOP-led House focused primarily on targeting pharmacy benefit managers, the arbitrators who control most Americans’ insurance coverage for medicines.
Costs of Coverage
Health care costs continue to rise for many Americans. The cost of employer-sponsored health plans have hit new highs in the past few months, raising costs for employers and workers alike. Experts have attributed the increase to high demand and expensive prices for certain drugs and treatments, notably weight loss drugs, as well as to medical inflation.
Meanwhile, the ACA is popular. The KFF poll found that more adults want to see the program expanded than scaled back. And a record 21.3 million people signed up for coverage in 2024, about 5 million of them new customers.
Enrollment in Republican-dominated states has grown fastest, with year-over-year increases of 80% in West Virginia, nearly 76% in Louisiana, and 62% in Ohio, according to the Centers for Medicare & Medicaid Services.
Public support for Obamacare and record enrollment in its coverage have made it politically perilous for Republicans to pursue the law’s repeal, especially without a robust alternative. That hasn’t stopped Trump from raising that prospect on the campaign trail, though it’s hard to find any other Republican candidate willing to step out on the same limb.
“The more he talks about it, the more other candidates have to start answering for it,” said Jarrett Lewis, a partner at Public Opinion Strategies, a GOP polling firm.
“Will a conversation about repeal-and-replace resonate with suburban women in Maricopa County?” he said, referring to the populous county in Arizona known for being a political bellwether. “I would steer clear of that if I was a candidate.”
Biden and his campaign have pounced on Trump’s talk of repeal. The president has said he wants to make permanent the enhanced premium subsidies he signed into law during the pandemic that are credited with helping to increase enrollment.
Republican advisers generally recommend that their candidates promote “a market-based system that has the consumer much more engaged,” said Lewis, citing short-term insurance plans as an example. “In the minds of Republicans, there is a pool of people that this would benefit. It may not be beneficial for everyone, but attractive to some.”
Biden and his allies have criticized short-term insurance plans — which Trump made more widely available — as “junk insurance” that doesn’t cover care for serious conditions or illnesses.
Entitlements Are Off-Limits
Both Medicaid and Medicare, the government health insurance programs that cover tens of millions of low-income, disabled, and older people, remain broadly popular with voters, said the Democratic pollster Celinda Lake. That makes it unlikely either party would pursue a platform that includes outright cuts to entitlements. But accusing an opponent of wanting to slash Medicare is a common, and often effective, campaign move.
Although Trump has said he wouldn’t cut Medicare spending, Democrats will likely seek to associate him with other Republicans who support constraining the program’s costs. Polls show that most voters oppose reducing any Medicare benefits, including by raising Medicare’s eligibility age from 65. However, raising taxes on people making more than $400,000 a year to shore up Medicare’s finances is one idea that won strong backing in a recent poll by The Associated Press and NORC Center for Public Affairs Research.
Brian Blase, a former Trump health adviser and the president of Paragon Health Institute, said Republicans, if they win more control of the federal government, should seek to lower spending on Medicare Advantage — through which commercial insurers provide benefits — to build on the program’s efficiencies and ensure it costs taxpayers less than the traditional program.
So far, though, Republicans, including Trump, have expressed little interest in such a plan. Some of them are clear-eyed about the perils of running on changing Medicare, which cost $829 billion in 2021 and is projected to consume nearly 18% of the federal budget by 2032.
“It’s difficult to have a frank conversation with voters about the future of the Medicare program,” said Lewis, the GOP pollster. “More often than not, it backfires. That conversation will have to happen right after a major election.”
Addiction Crisis
Many Americans have been touched by the growing opioid epidemic, which killed more than 112,000 people in the United States in 2023 — more than gun deaths and road fatalities combined. Rural residents and white adults are among the hardest hit.
Federal health officials have cited drug overdose deaths as a primary cause of the recent drop in U.S. life expectancy.
Republicans cast addiction as largely a criminal matter, associating it closely with the migration crisis at the U.S. southern border that they blame on Biden. Democrats have sought more funding for treatment and prevention of substance use disorders.
“This affects the family, the neighborhood,” said Blendon, the public opinion researcher.
Billions of dollars have begun to flow to states and local governments from legal settlements with opioid manufacturers and retailers, raising questions about how to best spend that money. But it isn’t clear that the crisis, outside the context of immigration, will emerge as a campaign issue.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: