10 Ways To Balance Blood Sugars
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Let Them Eat Cake”, She Said…
This is Jessie Inchauspé, a French biochemist and author. She’s most known for her best-selling “Glucose Revolution: The Life-Changing Power Of Balancing Your Blood Sugar”.
It’s a great book (which we reviewed recently) and you absolutely should read it, but meanwhile, we’re going to distill at least the most critical core ideas, 10almonds style. In this case, her “ten hacks”:
Eat foods in the right order
The order is:
- Fiber first
- Protein and fat second
- Starches and sugars last
What happens here is… the fiber perks up the gut bacteria, the protein and fat will then be better-digested next, and the starches and sugars will try to jump the line, but they can’t because the fiber is a physical speedbump and the proteins and fats are taking the prime place for being digested. So instead, the starches and sugars—usually responsible for blood sugar spikes—get processed much more gradually, resulting in a nice even curve.
Add a green starter to all your meals
We know what you’re thinking: “that’s just the first one again”, but no. This is an extra starter, before you get to that. If you’re the cook of the household, this can absolutely simply mean snacking on green ingredients while cooking.
Stop counting calories
Especially, she advises: stop worrying about extra calories from fats, such as if doing an oil-and-vinegar dressing for salad—which she also recommends, because all three components (the oil, the vinegar, and the salad) help even out blood sugar levels.
Flatten your breakfast curve
For many, breakfast is the starchiest meal of the day, if not the sugariest. Inchauspé recommends flipping this (ideally) or softening it (if you really must have a carb-based breakfast):
- Top choices include: a warm vegetable salad, fish, or eggs (or tofu if you don’t do animal products).
- Next-best include: if you must have toast, make sure to have butter (and/or the aforementioned egg/tofu, for example) to give your digestion an extra thing to do.
- Also: she recommends skipping the juice in favour of home-made breakfast smoothies. That way, instead of basically just sugar with some vitamins, you’re getting a range of nutrients that, if you stack it right, can constitute a balanced meal itself, with fiber + protein + fat + carbs.
Have any type of sugar—they’re all the same
They’re technically not, but the point is that your body will immediately take them apart and then they will be just the same. Whether it’s the cheapest white sugar or the most expensive organic lovingly hand-reared free-range agave nectar, your body is going to immediately give it the chop-shop treatment (a process so quick as to be practically instantaneous) and say “this is now glucose”.
Pick a dessert over a sweet snack
Remember that about the right order for foods? A dessert, when your body is already digesting dinner, is going to make much less of a glucose spike than, say, a blueberry muffin when all you’ve had this morning is coffee and juice.
Reach for the vinegar before you eat
We recently did a whole main feature about this, so we’ll not double up today!
After you eat, move
The glucose you eat will be used to replace lost muscle glycogen, before any left over is stored as fat… and, while it’s waiting to be stored as fat, just sitting in your bloodstream being high blood sugars. So, this whole thing will go a lot better if you are actively using muscle glycogen (by moving your body).
Inchauspé gives a metaphor: imagine a steam train worker, shoveling coal into the furnace. Meanwhile, other workers are bringing more coal. If the train is moving quickly, the coal can be shoveled into the furnace and burned and won’t build up so quickly. But if the train is moving slowly or not at all, that coal is just going to build up and build up, until the worker can shovel no more because of being neck-deep in coal.
Same with your blood sugars!
If you want to snack, go low-sugar
In the category of advice that will shock nobody: sugary snacks aren’t good for avoiding blood sugar spikes! This one probably didn’t need a chapter devoted to it, but anyway: low sugar is indeed the way to go for snacks.
Put some clothes on your carbs
This is about olive oil on pasta, butter on potatoes, and so forth. Basically, anything starchy is going to be broken down quickly to sugar and sent straight into the bloodstream, if there’s nothing to slow it down. If you’re wondering what to do with rice: adding a tablespoon of chia seeds to the rice while cooking (so they’re cooked together) will add very healthy fats to your rice, and (because they’ve been cooked) will not seem like eating seeds, by the way. In terms of texture and appearance, it’ll be as though you threw some black pepper in*
*which you should also do for many reasons, but that’s beyond the scope of this “about blood sugars” feature!
Wanting to know more about the science of this?
We’ve done all we have room for here today, but Inchauspé is, as ever, happy to explain it herself:
Prefer text? Check out:
The Science Behind Glucose Goddess
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Beyond “Make Your Bed”—life lessons from experience

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Beyond “Make Your Bed”—life lessons from experience

This is Admiral William H. McRaven, a former United States Navy four-star admiral who served as the ninth commander of the United States Special Operations Command.
So, for those of us whose day-to-day lives don’t involve coordinating military operations, what does he have to offer?
Quick note: 10almonds’ mission statement is “to make health and productivity crazy simple”.
We tend to focus on the health side of this, and in the category of productivity, it’s often what most benefits our mental health.
We’re writing less for career-driven technopreneurs in the 25–35 age bracket and more for people with a more holistic view of productivity and “a good life well-lived”.
So today’s main feature is more in that vein!
Start each day with an accomplishment
McRaven famously gave a speech (and wrote a book) that began with the advice, “make your bed”. The idea here doesn’t have to be literal (if you’ll pardon the pun). Indeed, if you’re partnered, then depending on schedules and habits, it could be you can’t (sensibly) make your bed first thing because your partner is still in it. But! What you can do is start the day with an accomplishment—however small. A short exercise routine is a great example!
Success in life requires teamwork
We’re none of us an island (except in the bathtub). The point is… Nobody can do everything alone. Self-sufficiency is an illusion. You can make your own coffee, but could you have made the coffee machine, or even the cup? How about, grown the coffee? Transported it? So don’t be afraid to reach out for (and acknowledge!) help from others. Teamwork really does make the dream work.
It’s what’s inside that counts
It’s a common trap to fall into, getting caught up the outside appearance of success, rather than what actually matters the most. We need to remember this when it comes to our own choices, as well as assessing what others might bring to the table!
A setback is only permanent if you let it be
No, a positive attitude won’t reverse a lifelong degenerative illness, for example. But what we can do, is take life as comes, and press on with the reality, rather than getting caught up in the “should be”.
Use failure to your advantage
Learn. That’s all. Learn, and improve.
Be daring in life
To borrow from another military force, the SAS has the motto “Who dares, wins”. Caution has it place, but if we’ve made reasonable preparations*, sometimes being bold is the best (or only!) way forward.
*Meanwhile the Parachute Regiment, from which come 80% of all SAS soldiers, has the motto “Utrinque paratus”, “prepared on all sides”.
Keep courage close
This is about not backing down when we know what’s right and we know what we need to do. Life can be scary! But if we don’t overcome our fears, they can become self-realizing.
Writer’s note: a good example of this is an advice I sometimes gave during my much more exciting (military) life of some decades ago, and it pertains to getting into a knife-fight (top advice for civilians: don’t).
But, if you’re in one, you need to not be afraid of getting cut.
Because if you’re not afraid of getting cut, you will probably get cut.
But if you are afraid of getting cut, you will definitely get cut.
Hopefully your life doesn’t involve knives outside of the kitchen (mine doesn’t, these days, and I like it), but the lesson applies to other things too.
Sometimes the only way out is through.
Be your best at your worst
Sometimes life is really, really hard. But if we allow those moments to drive us forwards, they’re also a place we can find more strength than we ever knew we had.
Keep on swimming
It’s said that the majority in life is about showing up—and often it is. But you have to keep showing up, day after day. So make what you’re doing sustainable for you, and keep on keeping on.
Share This Post
-

Rainbow Roasted Potato Salad
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This salad has potatoes in it, but it’s not a potato salad as most people know it. The potatoes are roasted, but in a non-oily-dressing, that nevertheless leaves them with an amazing texture—healthy and delicious; the best of both worlds. And the rest? We’ve got colorful vegetables, we’ve got protein, we’ve got seasonings full of healthy spices, and more.
You will need
- 1½ lbs new potatoes (or any waxy potatoes; sweet potato is also a great option; don’t peel them, whichever you choose) cut into 1″ chunks
- 1 can / 1 cup cooked cannellini beans (or your preferred salad beans)
- 1 carrot, grated
- 2 celery stalks, finely chopped
- 3 spring onions, finely chopped
- ½ small red onion, finely sliced
- 2 tbsp white wine vinegar
- 1 tbsp balsamic vinegar
- 1 tbsp lemon juice
- 1 tbsp nutritional yeast
- 1 tsp garlic powder
- 1 tsp black pepper
- ½ tsp red chili powder
- We didn’t forget salt; it’s just that with the natural sodium content of the potatoes plus the savory flavor-enhancing properties of the nutritional yeast, it’s really not needed here. Add if you feel strongly about it, opting for low-sodium salt, or MSG (which has even less sodium).
- To serve: 1 cup basil pesto (we’ll do a recipe one of these days; meanwhile, store-bought is fine, or you can use the chermoula we made the other day, ignoring the rest of that day’s recipe and just making the chermoula component)
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven as hot as it goes!
2) Combine the potatoes, white wine vinegar, nutritional yeast, garlic powder, black pepper, and red chili powder, mixing thoroughly (but gently!) to coat.
3) Spread the potatoes on a baking tray, and roast in the middle of the oven (for best evenness of cooking); because of the small size of the potato chunks, this should only take about 25 minutes (±5mins depending on your oven); it’s good to turn them halfway through, or at least jiggle them if you don’t want to do all that turning.
4) Allow to cool while still on the baking tray (this allows the steam to escape immediately, rather than the steam steaming the other potatoes, as it would if you put them in a bowl).
5) Now put them in a serving bowl, and mix in the beans, vegetables, balsamic vinegar, and lemon juice, mixing thoroughly but gently
6) Add generous lashings of the pesto to serve; it should be gently mixed a little too, so that it’s not all on top.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- White Potato vs Sweet Potato – Which is Healthier?
- Eat More (Of This) For Lower Blood Pressure
- Our Top 5 Spices: How Much Is Enough For Benefits?
Take care!
Share This Post
-

Language Fluency Beats General Intelligence & Memory For Longevity
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
And no, it doesn’t have to be a second language, although that helps a lot:
An Underrated Tool Against Alzheimer’s ← you don’t even have to learn the second language to a high level, to benefit
Rather, what we’re talking about today is your first language fluency. So, for most of our readers, English. For the study participants it was German, because this was a German research team using data from the German population.
The Berlin Aging Study
Previous research has linked intelligence to longevity, but intelligence comprises multiple traits. So, what’s most important? Memory? General intelligence? Nope. Language fluency!
Let’s clarify something before we continue: “fluency” does not, in linguistics, mean what most people use it to mean. It’s not about the size of one’s overall knowledge of the language (e.g. vocabulary size), but rather, it is about one’s ability to speak and/or write fluently—literally, fluently means “flowingly”, i.e. without undue hesitation or difficulty.
The study used data from the Berlin Aging Study, which tracked 516 people aged 70–105 from 1989 onwards.
Researchers assessed four cognitive abilities, with two kinds of tests for each of:
- Verbal fluency (detailed description below)
- Perceptual speed (pattern-recognition speed)
- Verbal knowledge (vocabulary size)
- Episodic memory (personal memory recall)
General intelligence, meanwhile, was assessed as “the average of those 8 scores”.
The two tests for the cognitive ability of “verbal fluency” were:
Categories
Participants had to name as many different animals as possible within 90 seconds. Their answers were subsequently rated for correctness by two independent research assistants, to assure that noticed or unnoticed repetitions, wrong categories, and morphological variants were not coded as correct.
Word beginnings
Participants were asked to name as many different real words starting with the letter s as possible within 90 seconds. The named words were rated for correctness by two independent research assistants to avoid considering repetitions, morphological variants, and wrong words as correct.
You can read about these and the other tests for the other cognitive abilities, in the paper itself:
Verbal Fluency Selectively Predicts Survival in Old and Very Old Age ← if you’re looking for the test descriptions, scroll to “Method” and then scroll past the table, and you’ll see the test descriptions
They found that of all these metrics, only the two verbal fluency tests (and none of the other tests) showed a significant link to longevity.
Why this is important
Although the study does not prove causality (it could be that people who are predisposed to live longer for other reasons are more verbally fluent because of some common factor that influences both language fluency and longevity), it seems as good a reason as any to develop and maintain language fluency.
This builds on what was found in “The Nun Study“, that followed a convent of nuns (because they are a very homogenous sample in terms of occupation, location, diet, routine, etc, so a lot of confounding factors were already controlled-for) and made numerous major discoveries about things that impact aging (including the relevance of the APOE4 gene! That was The Nun Study).
When it came to nuns and language…
Based on the autobiographies written by the nuns in their youth upon taking their vows, there were two factors that were later correlated with not getting dementia:
- Longer sentences
- Positive outlook
- “Idea density”
That latter item means the relative linguistic density of ideas and complexity thereof, and the fluency and vivacity with which they were expressed (this was not a wishy-washy assessment; there was a hard-science analysis to determine numbers).
Want to spruce up yours? You might like to check out:
Reading, Better: Reading As A Cognitive Exercise
…for specific, evidence-based ways to tweak your reading to fight cognitive decline.
Take care!
Share This Post

Related Posts
-

Asbestos in mulch? Here’s the risk if you’ve been exposed
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Mulch containing asbestos has now been found at 41 locations in New South Wales, including Sydney parks, schools, hospitals, a supermarket and at least one regional site. Tests are under way at other sites.
As a precautionary measure, some parks have been cordoned off and some schools have closed temporarily. Fair Day – a large public event that traditionally marks the start of Mardi Gras – was cancelled after contaminated mulch was found at the site.
The New South Wales government has announced a new taskforce to help investigate how the asbestos ended up in the mulch.
Here’s what we know about the risk to public health of mulch contaminated with asbestos, including “friable” asbestos, which has been found in one site (Harmony Park in Surry Hills).
What are the health risks of asbestos?
Asbestos is a naturally occurring, heat-resistant fibre that was widely used in building materials from the 1940s to the 1980s. It can be found in either a bonded or friable form.
Bonded asbestos means the fibres are bound in a cement matrix. Asbestos sheeting that was used for walls, fences, roofs and eaves are examples of bonded asbestos. The fibres don’t escape this matrix unless the product is severely damaged or worn.
A lot of asbestos fragments from broken asbestos products are still considered bonded as the fibres are not released as they lay on the ground.
Asbestos sheeting was used for walls and roofs.
Tomas Regina/ShutterstockFriable asbestos, in contrast, can be easily crumbled by touch. It will include raw asbestos fibres and previously bonded products that have worn to the point that they crumble easily.
The risk of disease from asbestos exposure is due to the inhalation of fibres. It doesn’t matter if those fibres are from friable or bonded sources.
However, fibres can more easily become airborne, and therefore inhalable, if the asbestos is friable. This means there is more of a risk of exposure if you are disturbing friable asbestos than if you disturb fragments of bonded asbestos.
Who is most at risk from asbestos exposure?
The most important factor for disease risk is exposure – you actually have to inhale fibres to be at risk of disease.
Just being in the vicinity of asbestos, or material containing asbestos, does not put you at risk of asbestos-related disease.
For those who accessed the contaminated areas, the level of exposure will depend on disturbing the asbestos and how many fibres become airborne due to that disturbance.
However, if you have been exposed to, and inhaled, asbestos fibres it does not mean you will get an asbestos-related disease. Exposure levels from the sites across Sydney will be low and the chance of disease is highly unlikely.
The evidence for disease risk from ingestion remains highly uncertain, although you are not likely to ingest sufficient fibres from the air, or even the hand to mouth activities that may occur with playing in contaminated mulch, for this to be a concern.
The risk of disease from exposure depends on the intensity, frequency and duration of that exposure. That is, the more you are exposed to asbestos, the greater the risk of disease.
Most asbestos-related disease has occurred in people who work with raw asbestos (for example, asbestos miners) or asbestos-containing products (such as building tradespeople). This has been a tragedy and fortunately asbestos is now banned.
There have been cases of asbestos-related disease, most notably mesothelioma – a cancer of the lining of the lung (mostly) or peritoneum – from non-occupational exposures. This has included people who have undertaken DIY home renovations and may have only had short-term exposures. The level of exposure in these cases is not known and it is also impossible to determine if those activities have been the only exposure.
There is no known safe level of exposure – but this does not mean that one fibre will kill. Asbestos needs to be treated with caution.
As far as we are aware, there have been no cases of mesothelioma, or other asbestos-related disease, that have been caused by exposure from contaminated soils or mulch.
Has asbestos been found in mulch before?
Asbestos contamination of mulch is, unfortunately, not new. Environmental and health agencies have dealt with these situations in the past. All jurisdictions have strict regulations about removing asbestos products from the green waste stream but, as is happening in Sydney now, this does not always happen.
Mulch contamination is not new.
gibleho/ShutterstockWhat if I’ve been near contaminated mulch?
Exposure from mulch contamination is generally much lower than from current renovation or construction activities and will be many orders of magnitude lower than past occupational exposures.
Unlike activities such as demolition, construction and mining, the generation of airborne fibres from asbestos fragments in mulch will be very low. The asbestos contamination will be sparsely spread throughout the mulch and it is unlikely there will be sufficient disturbance to generate large quantities of airborne fibres.
Despite the low chance of exposure, if you’re near contaminated mulch, do not disturb it.
If, by chance, you have had an exposure, or think you have had an exposure, it’s highly unlikely you will develop an asbestos-related disease in the future. If you’re worried, the Asbestos Safety and Eradication Agency is a good source of information.

Peter Franklin, Associate Professor and Director, Occupational Respiratory Epidemiology, The University of Western Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
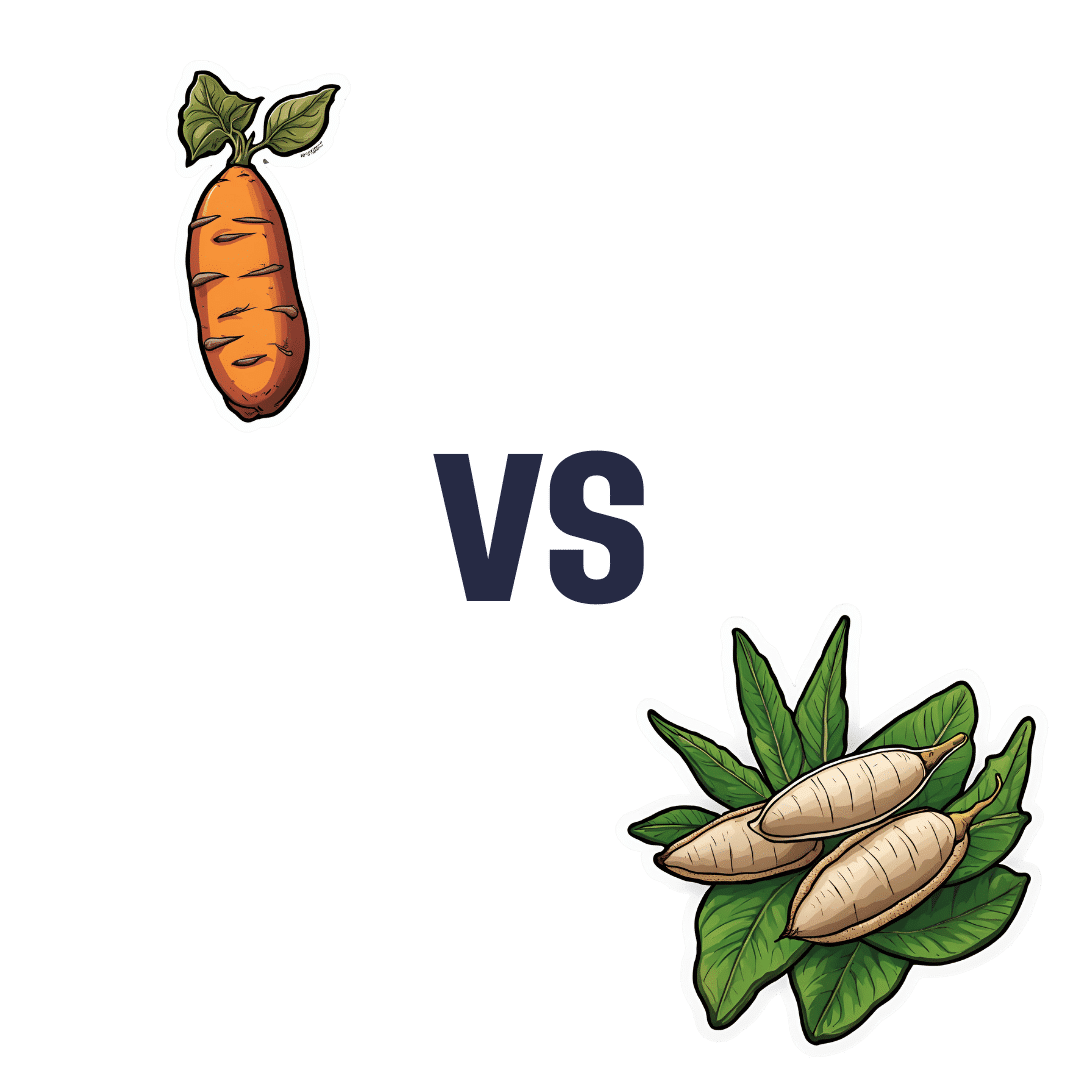
Sweet Potato vs Cassava – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing sweet potato to cassava, we picked the sweet potato.
Why?
For any unfamiliar with cassava, it’s also called manioc or yuca/yucca, and it’s a tuber that can be used a lot like sweet potato. It’s popular in S. America, often in recipes that aren’t the healthiest (deep-fried chunky “cassava chips” are popular in Brazil, for example, and farofa, a flour made from cassava, is less healthy even than refined white flour from wheat), but today we’re going to judge it on its own merit—since after all, almost anything can be deep-fried and many things can be turned into flour, but it doesn’t mean we have to do that.
Let’s talk macros first: sweet potato has nearly 2x the protein, while cassava has nearly 2x the carbs. As for fiber to soften those carbs’ impact on our blood sugars, well, sweet potato has about 2x the fiber. All in all for macros, a clear and easy win for sweet potato.
Important note: as for the impact that has on glycemic index: the exact glycemic index will depend on what you do with it (different cooking methods change the GI), but broadly speaking, sweet potatoes are considered a medium GI food, while cassava is a very high GI food, to the point that it’s higher than sucrose, and nearly equal to pure glucose. Which is impressive, for a tuber.
In terms of vitamins, sweet potato’s famously high vitamin A content raises the bar, but it’s not all it has to offer: sweet potato has more of vitamins A, B1, B2, B3, B5, B6, E, and K, while cassava has more of vitamins B9 and choline. Just for amusement’s sake, let’s note that the sweet potato has over 1,478x the vitamin A content. In any case, the vitamins category is another clear win for sweet potato.
When it comes to minerals, it’s again quite one-sided: sweet potato has more calcium, copper, iron, magnesium, manganese, phosphorus, and potassium, while cassava has more selenium. So, sweet potato wins yet again.
In short: definitely a case of “the less widely-available option is not necessarily the healthier”!
Want to learn more?
You might like to read:
Glycemic Index vs Glycemic Load vs Insulin Index
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
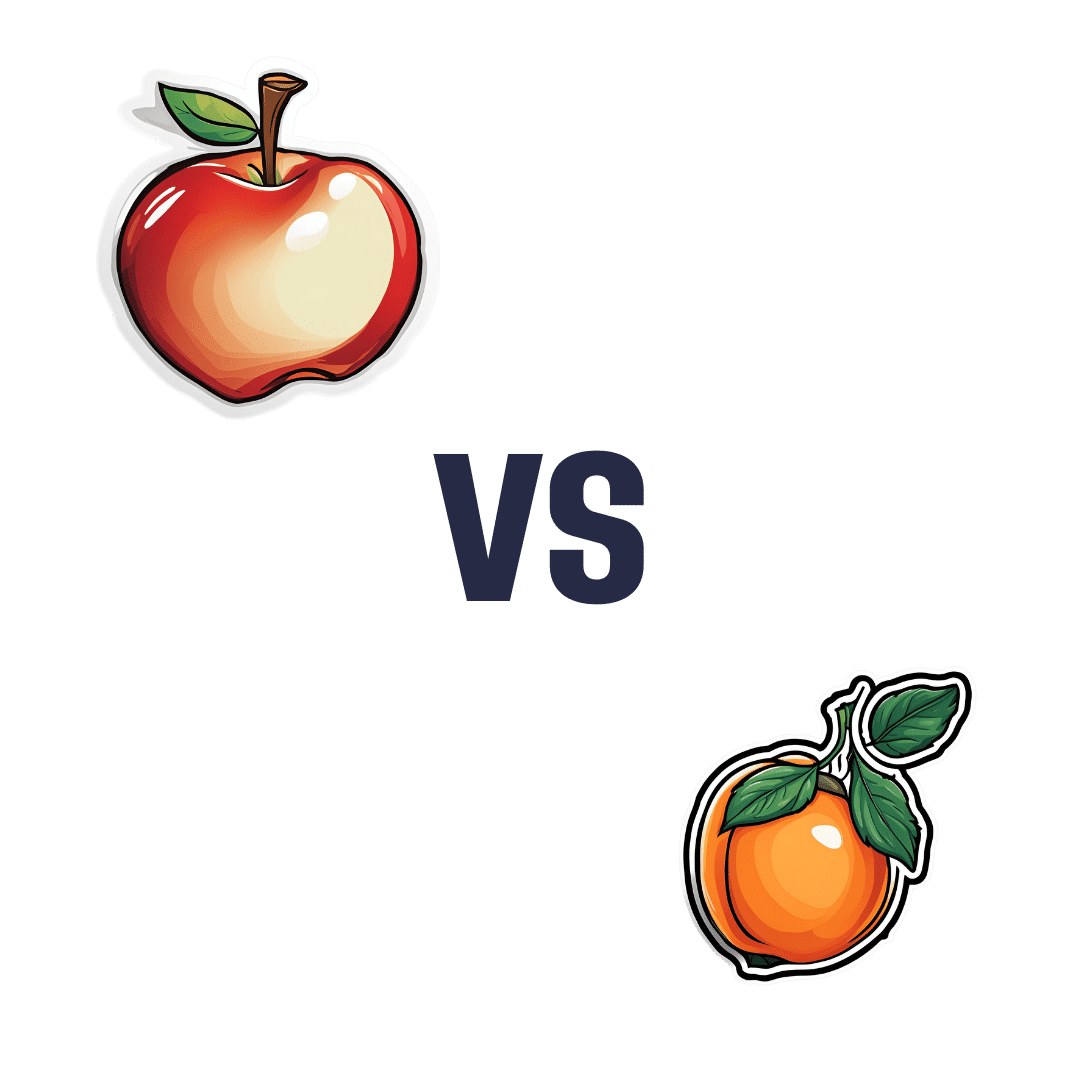
Apple vs Apricot – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apple to apricot, we picked the apricot.
Why?
In terms of macros, there’s not too much between them; apples are higher in carbs and only a little higher in fiber, which disparity makes for a slightly higher glycemic index, but it’s not a big difference and they are both low GI foods.
Micronutrients, however, set these two fruits apart:
In the category of vitamins, apple is a tiny bit higher in choline, while apricots are higher in vitamins A, B1, B2, B3, B5, B6, B9, C, E, and K—in most cases, by quite large margins, too. All in all, a clear and easy win for apricots.
When it comes to minerals, apples are not higher in any minerals, while apricots are higher in calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. There’s simply no contest here.
In short, if an apple a day keeps the doctor away, then an apricot will give the doctor a nice weekend break somewhere.
Want to learn more?
You might like to read:
Top 8 Fruits That Prevent & Kill Cancer
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: