Strawberries vs Blackberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing strawberries to blackberries, we picked the blackberries.
Why?
Shocking nobody, both are very healthy options. However, blackberries do come out on top:
In terms of macros, the main thing that sets them apart is that blackberries have more than 2x the fiber. Other differences in macros are also in blackberries’ favor, but only very marginally, so we’ll not distract with those here. The fiber difference is distinctly significant, though.
In the category of vitamins, blackberries lead with more of vitamins A, B2, B3, B5, B9, E, and K, as well as more choline. Meanwhile, strawberries boast more of vitamins B1, B6, and C. So, a 8:2 advantage for blackberries (and some of the margins are very large, such as 9x more choline, 4x more vitamin E, and nearly 18x more vitamin A).
When it comes to minerals, things are not less clear: blackberries have considerably more calcium, copper, iron, magnesium, manganese, and zinc. The two fruits are equal in other minerals that they both contain, and strawberries don’t contain any mineral in greater amounts than blackberries do.
A discussion of these berries’ health benefits would be incomplete without at least mentioning polyphenols, but both of them are equally good sources of such, so there’s no distinction to set one above the other in this category.
As ever, enjoy both, though! Diversity is good.
Want to learn more?
You might like to read:
- Strawberries vs Cherries – Which is Healthier?
- Blackberries vs Blueberries – Which is Healthier?
- Strawberries vs Raspberries – Which is Healthier?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Uric Acid’s Extensive Health Impact (And How To Lower It)

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Uric Acid’s Extensive Health Impact (And How To Lower It)

This is Dr. David Perlmutter. He’s a medical doctor, and a Fellow of the American College of Nutrition. He’s a member of the Editorial Board for the Journal of Alzheimer’s Disease, and has been widely published in many other peer-reviewed journals.
What does he want us to know?
He wants us to know about the health risks of uric acid (not something popularly talked about so much!), and how to reduce it.
First: what is it? Uric acid is a substance we make in our own body. However, unlike most substances we make in our body, we have negligible use for it—it’s largely a waste product, usually excreted in urine.
However, if we get too much, it can build up (and crystallize), becoming such things as kidney stones, or causing painful inflammation if it shows up in the joints, as in gout.
More seriously (unpleasant as kidney stones and gout may be), this inflammation can have a knock-on effect triggering (or worsening) other inflammatory conditions, ranging from non-alcoholic fatty liver disease, to arthritis, to dementia, and even heart problems. See for example:
- David Perlmutter | Uric Acid and Cognitive Decline
- American Heart Association | Uric acid linked to later risk for irregular heart rhythm
- World Journal of Gastroenterology | The role of uric acid in non-alcoholic steatohepatitis development
How can we reduce our uric acid levels?
Uric acid is produced when we metabolize purine nucleotides, which are found in many kinds of food. We can therefore reduce our uric acid levels by reducing our purine intake, as well as things that mess up our liver’s ability to detoxify things. Offsetting the values for confounding variables (such as fiber content, or phytochemicals that mitigate the harm), the worst offenders include…
Liver-debilitating things:
- Alcohol (especially beer)
- High-fructose corn syrup (and other fructose-containing things that aren’t actual fruit)
- Other refined sugars
- Wheat / white flour products (this is why beer is worse than wine, for example; it’s a double-vector hit)
Purine-rich things:
- Red meats and game
- Organ meats
- Oily fish, and seafood (great for some things; not great for this)
Some beans and legumes are also high in purines, but much like real fruit has a neutral or positive effect on blood sugar health despite its fructose content, the beans and legumes that are high in purines, also contain phytochemicals that help lower uric acid levels, so have a beneficial effect.
Eggs (consumed in moderation) and tart cherries have a uric-acid lowering effect.
Water is important for all aspects of health, and doubly important for this.
Hydrate well!
Lifestyle matters beyond diet
The main key here is metabolic health, so Dr. Perlmutter advises the uncontroversial lifestyle choices of moderate exercise and good sleep, as well as (more critically) intermittent fasting. We wrote previously on other things that can benefit liver health:
…in this case, that means the liver gets a break to recuperate (something it’s very good at, but does need to get a chance to do), which means that while you’re not giving it something new to do, it can quickly catch up on any backlog, and then tackle any new things fresh, next time you start eating.
Want to know more about this from Dr. Perlmutter?
You might like his article:
An Integrated Plan for Lowering Uric Acid ← more than we had room for here; he also talks about extra things to include in your diet/supplementation regime for beneficial effects!
And/or his book:
…on which much of today’s main feature was based.
Take care!
Share This Post
-

Eat This Daily For No Wrinkles (& How It Works)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Andrea Suarez explains:
Go nuts for…
Almonds! They’re rich in vitamin E (alpha-tocopherol), beta-sitosterol, squalane, protein, and fiber:
- Vitamin E acts as an antioxidant, protecting skin lipids.
- Lipids in almonds support the skin barrier and hydration.
- Protein is necessary for collagen synthesis.
- Fiber promotes gut health, indirectly benefiting skin.
- Polyphenolic compounds in almond skins (not the shells, the skins, the fibrous brown part that slides off if you blanch them) provide additional skin protection.
The science (yes, there have been almond intervention studies!):
- 2019 Study:
- Participants: 28 post-menopausal women with fair skin (Fitzpatrick phototype 1-2).
- Design: 20% of daily calories from almonds vs. a calorie-matched snack.
- Results: 9% decrease in facial wrinkles in the almond group, no change in oil production or barrier function.
- 2021 Study:
- Extended Duration: 24 weeks with a similar design as the 2019 study.
- Findings: further wrinkle reduction and improvement in skin pigmentation.
- Mechanism: vitamin E may reduce hyperpigmentation and support antioxidant defense.
- UV Protection Study (2021):
- Participants: healthy Asian women (18–45 years, Fitzpatrick phototype 2-4).
- Method: daily almond snack vs pretzel snack for 12 weeks.
- Outcome: increased skin resistance to UV damage in the almond group.
Obviously, a limitation is there is not really an option to make a RCT with a blinded control; “…and group B will only think they are eating almonds” doesn’t really work. Hence, interventional RCTs with a non-blinded control (the calorie-matched snack).
Almonds may not be the cure to all things, but they certainly are potent nuts. Best enjoyed, of course, as part of a healthy overall diet (Mediterranean diet is great), and it’s certainly advisable to take care of your skin from the outside too (sunscreen as a must; other things optional).
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Why You Should Diversify Your Nuts
Take care!
Share This Post
-

Mastering Gut Health for Women – by Karín Feltman
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The author, a registered nurse, has a focus on holistic health, and in this book it’s all about wellness from the inside out.
To effect this, she lays out a 12-week program of transformations:
- Week 1: transform your knowledge
- Week 2: transform your brain
- Week 3: transform your digestion
- Week 4: transform your immunity
- Week 5: transform your emotions
- Week 6: transform your sleep
- Week 7: transform your energy/vitality
- Week 8: transform your activity
- Week 9: transform your hormones
- Week 10: transform your diet
- Week 11: transform your weight
- Week 12: transform your habits
Which all adds up to quite a comprehensive overall transformation!
Of course, it’s possible you might want to implement everything at once; an exciting prospect for sure, but oftentimes it really is best to just change one thing at once before moving on; that way it’s a lot more likely to stick, and that’s why she presents it in this format.
On the other hand, maybe you might want to take longer than the 12 weeks, if for example it takes you more than a week to do a certain part. That’s fine too, though for most people without serious constraints (or suffering some unexpected major interruption to your usual life), the 12-week program should be quite doable as-is.
The style is personable and friendly, albeit with frequent references to science and appropriate citations.
Bottom line: the title centers gut health, and so does the book itself, but this is truly a holistic approach that goes far beyond the gut, which makes it even more worthwhile.
Click here to check out Mastering Gut Health For Women, and master gut health for yourself!
Share This Post


Related Posts
-
Kettlebell Swings Are Not What Most People Think They Are (They’re Better)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Commonly assumed to be mostly a shoulders-and-arms exercise, they’re actually mostly about the hips and core:
From the hips
Correctly executed kettlebell swings primarily strengthens muscles from the hamstrings and glutes the to abs and back; in other words, muscles whose strength is essential for power, posture, and injury prevention.
The core in particular is not to be underestimated, with deep stabilizing muscles supporting posture, balance, and movement. Strengthening these areas can also help reduce lower back pain.
How to do it correctly: start with your feet shoulder-width apart (this is important, if you like having knees) and grip the kettlebell with both hands. Hinge at your hips, lowering the kettlebell between your legs while keeping your back flat and core engaged. Then, drive your hips forward explosively to swing the kettlebell up to shoulder height before allowing it to return down with control. The most common mistake is using the arms to lift the kettlebell, but the real power should come from the hips to maximize benefits and prevent injury.
Example workout: 30 seconds of kettlebell swings followed by 30 seconds of rest, repeated for 10 sets. This 10-minute routine provides a full-body workout that builds strength and endurance. As you progress, you can increase the weight, duration, number of sets, etc.
Timeline of changes: within a few weeks of regular kettlebell swings, you should notice stronger glutes, better endurance, and improved posture. After a month, you may experience reduced lower back pain (if you had lower back pain) and more power in your everyday movements. By two to three months, visible muscle definition and fat loss are likely to become noticeable, along with increased overall strength.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Body Sculpting with Kettlebells for Women – by Lorna Kleidman
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How influencers and content creators discuss birth control on social media: What research shows
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
News articles in recent weeks have documented the spread of misinformation about hormonal birth control methods on popular social media platforms like TikTok, YouTube and X, formerly called Twitter. Influencers with large and small followings are sharing unsubstantiated claims about the side effects of contraceptives, while directly or indirectly encouraging others to stop using them.
This trend has not escaped researchers, who for several years have been investigating what people who can get pregnant are posting on social media platforms about hormonal and non-hormonal birth control methods. Understanding the drivers of these trends is important because they have implications for policy and patient care, according to researchers. Some worry that during the post-Dobbs era, when there are continued strikes against reproductive rights in the U.S., misinformation about birth control on social media could have a negative influence on contraceptive preferences — potentially leading to more unwanted pregnancies.
More than 90% of women of reproductive age have used at least one contraceptive method, according to a 2023 report by the U.S. National Center for Health Statistics. However, the report also finds that the use of male condoms and withdrawal methods increased between 2006 and 2019, while the use of the birth control pill decreased. Non-hormonal contraception methods, including condoms, spermicides, withdrawal and menstrual cycle tracking, are 10% or less effective than hormonal contraceptives. The only exceptions are surgical sterilization and the copper intrauterine device.
To be sure, not all birth control-related content posted on social media platforms is negative, studies show. Health care professionals are sharing educational material with a high rate of engagement and non-health care professional users share their positive experiences with the birth control methods they use.
But as you will see in the studies curated below, researchers also find that social media users, including influencers, share inaccurate information about hormonal contraceptives on various social media platforms, discuss their discontinuation of birth control in favor of non-hormonal methods and engage in unsubstantiated fear-mongering of hormonal contraceptives.
Researchers also have learned that the content posted on social media platforms has changed in tone over time, mirroring the shift in the national political discourse.
In a 2021 study published in the American Journal of Obstetrics & Gynecology, researchers analyzed more than 800,000 English-language tweets mentioning at least one contraceptive method between March 2006, when Twitter was founded, and December 2019. They coded the sentiment of tweets as positive, neutral or negative.
“What we found over time was that the number of neutral tweets went down for each and every one of the birth control methods, and people became more polarized with regards to how they talk on these social media platforms over those 13 years,” says study co-author Dr. Deborah Bartz, an OB-GYN at Brigham and Women’s Hospital with expertise in complex family planning and an associate professor at Harvard Medical School.
In a February 2024 commentary in the Journal of Women’s Health, University of Delaware researchers Emily Pfender and Leah Fowler argue that ongoing dialogue about contraception on social media provides “a glimpse into public sentiment about available options” to people who can get pregnant.
The authors also note that misinformation and disinformation about hormonal contraception may have a larger effect on health disparities, especially among historically marginalized groups who may already mistrust the medical establishment.
“This may contribute to unintended pregnancy and delayed care, further widening health disparities and hindering progress toward equitable reproductive health outcomes,” Pfender and Fowler write.
Side effects
There are known side effects to hormonal birth control methods, including headaches, nausea, sore breasts and spotting. Most are mild and disappear with continued use or with switching to another method. Among hormonal contraceptives, only the Depo-Provera injection has been linked with weight gain, studies show.
But some social media influencers have spread false claims about the potential side effects of hormonal birth control methods, ranging from infertility to abortion to unattractiveness. Despite these false claims, physicians and professional organizations such as the American College of Obstetricians and Gynecologists find today’s contraceptive options safe and very effective.
“They’re about the most low-risk prescription that I give,” says Dr. Megana Dwarakanath, an adolescent medicine physician in Pittsburgh. “I always joke that if something goes wrong in someone’s life, they’re within the reproductive years, it always gets blamed on birth control.”
Dwarakanath says her young patients are most worried about two side effects: weight gain and mood. “Those are the things that they will almost always attribute to their birth control at a time that their bodies are also changing very rapidly,” she says. “Things like mental health diagnoses or personality disorders also tend to crop up during the time young people have started or have been on birth control.”
Most research on the link between oral contraceptives and cancer risk comes from observational studies, according to the National Cancer Institute. Overall, the studies have consistently shown that the risks of breast and cervical cancer are slightly increased for women who use oral contraceptives, whereas the risk of endometrial, ovarian and colorectal cancers are reduced.
The use of hormonal birth control has also been associated with an increase in the risk of developing blood clots, studies show. But that risk is not universal for everyone who takes hormonal birth control. This risk is higher for women 35 and older, those who smoke, are very overweight or have a history of cardiovascular disease. Overall, 3 to 9 out of 10,000 women who take the pill are at risk of developing blood clots within a given year. The risk for women who don’t take the pill is 1 to 5 out of 10,000.
There is no association between the pill and mood disorders, according to a large body of research, including a 2021 cohort study of nearly 740,000 young women.
It’s worth noting the dearth of research into women’s reproductive health due to chronic underfunding of women’s health research. An analysis of funding by the U.S. National Institutes of Health finds that in nearly three-quarters of the cases where a disease affects mainly one gender, the institute’s funding pattern favored males. Either the disease affected more women and was underfunded, or the disease affected more men and was overfunded, according to the 2021 study published in the Journal of Women’s Health.
Aside from underfunding, conducting robust research into the long-term effects of birth control is complex.
“Historically, people haven’t felt that it’s ethically OK to randomize people to birth control methods in large part because the outcome of unintended pregnancy is greater,” for people who are given the placebo, Bartz says.
Research on birth control misinformation on social media
Social media use is widespread among young adults. More than 90% of Americans between 18 and 29 reported ever using YouTube, while 78% said they had used Instagram, 62% used TikTok and 42% used Twitter, according to a 2023 survey of 5,733 U.S. adults by Pew Research Center.
These years overlap with the demographic of people who are most likely to use birth control. And because the use of contraceptives is less stigmatized today, people are more likely to talk with one another about their questions and concerns or share that information online.
In addition to investigating the general landscape of social media posts about birth control, researchers are also interested in the type of content influencers, who typically have 20,000 or more followers, post, because of their persuasive power over their audiences.
“When influencers disclose personal experiences and beliefs about various topics, audience members tend to form similar attitudes especially when they feel connected to the influencer,” Pfender and M. Marie Devlin write in a 2023 study published in the journal Health Communication.
Below we have curated several studies published in recent years documenting the spread of birth control misinformation on social media. The roundup is followed by a quick reference guide on female contraceptives and their actual potential side effects.
Contraceptive Content Shared on Social Media: An Analysis of Twitter
Melody Huang, et al. Contraception and Reproductive Medicine, February 2024.The study: The authors explore how contraceptive information is shared on X and understand how those posts affect women’s decisions. They analyze a random 1% of publicly available English-language tweets about reversible prescription contraceptive methods, from January 2014 and December 2019. The 4,434 analyzed tweets included at least 200 tweets per birth control method — IUDs, implants, the pill, patch and ring.
The findings: 26.7% of tweets about contraceptive methods discussed decision-making and 20.5% discussed side effects, especially the side effects of IUDs and the depot medroxyprogesterone acetate (DMPA or Depo-Provera) shot. Discussions about the pill, patch or ring prompted more discussions on logistics and adherence. About 6% of tweets explicitly requested information. Tweets about IUDs were most popular in terms of likes.
More importantly, 50.6% of the tweets were posted by contraceptive users, while only 6% came from official health or news sources. Tweets from news or journalistic sources were more frequent than tweets from a health care professional or organization.
Some tweets contained misinformation represented as facts, such as the unsubstantiated claim that IUDs can cause fertility issues. Others were outwardly misogynistic, shaming women and claiming that they wouldn’t be able to have kids because of using hormonal birth control.
One takeaway: “While Twitter may provide valuable insight, with more tweets being created by personal contraceptive users than official healthcare sources, the available information may vary in reliability. Asking patients about information from social media can help reaffirm to patients the importance of social networks in contraceptive decision-making while also addressing misconceptions to improve contraceptive counseling,” the authors write.
What Do Social Media Influencers Say About Birth Control? A Content Analysis of YouTube Vlogs About Birth Control
Emily J. Pfender and M. Marie Devlin. Health Communication, January 2023.The study: To explore what social media influencers shared on YouTube about their experiences with hormonal and non-hormonal methods of birth control, the researchers analyzed 50 vlogs posted between December 2019 and December 2021. Most of the 50 influencers were categorized on YouTube as Lifestyle (72%) and Fitness (16%). They had between 20,000 and 2.2 million subscribers each.
The findings: In total, 74% of the influencers talked about discontinuing hormonal birth control. About 44% said the main reason they were discontinuing birth control was to be more natural, while 32% said they wanted to improve their mental health and 20% were concerned about weight gain.
Forty percent of influencers mentioned using non-hormonal birth control methods such as menstrual cycle tracking, condoms, non-hormonal IUDs and the pull-out method. Twenty percent reported switching from hormonal to non-hormonal methods.
One takeaway: “Our content analysis revealed that discontinuation of hormonal birth control is commonly discussed among [social media influencers] on YouTube and sexual health information from influencers might not provide accurate educational information and tools… this is especially concerning given that social media is young adults’ primary tool for sexual health information. Future research is needed to understand the effects of SMI birth control content on sexual health behaviors,” the authors write.
Hormonal Contraceptive Side Effects and Nonhormonal Alternatives on TikTok: A Content Analysis
Emily J. Pfender, Kate Tsiandoulas, Stephanie R. Morain and Leah R. Fowler. Health Promotion Practice, January 2024.The study: The authors analyzed the content of 100 TikTok videos that used the hashtags #birthcontrolsideeffects and #nonhormonalcontraception. Their goal was to understand the types of content about side effects of hormonal and non-hormonal contraceptives on TikTok.
The findings: The videos averaged about 1 minute and garnered an average of 27,795 likes, 251 comments and 623 shares. For #birthcontrolsideeffects, 80% of the audience was 18 to 24 years old and videos with that hashtag had 43 million views worldwide as of July 7, 2023.
Thirty-two percent of the videos were by regular users (non-influencers), 26 by clinicians, 13% by health coaches and 2% by companies. Only 3% had a sponsorship disclosure and 6% included a medical disclaimer, that the person was not a doctor or was not providing medical advice.
Most of the 100 videos (71%) mentioned hormonal contraception. Among them 51% discussed unspecific hormonal contraceptives, 31% talked about the pill and 11% about hormonal IUDs. Four of the 71 creators explicitly recommended against using hormonal contraceptives.
Claims about hormonal contraceptives were mostly based on personal experience. About 25% of the creators cited no basis for their claims, 23% included outside evidence, including unspecified studies or information from the FDA insert, and 11% used a combination of personal and outside evidence.
Almost half (49%) mentioned discontinuing their hormonal contraception, with negative side effects cited as the most common reason.
The creators talked about mental health issues, weight gain, headaches, and less common risks of various cancers or chronic illness, change in personality and blood clots. They were less likely to mention the positive aspects of birth control.
About 52% of videos mentioned non-hormonal contraception, including copper IUDs and cycle tracking.
Nine of the 100 creators expressed feeling dismissed, pressured, gaslit or insufficiently informed about contraception by medical providers.
One takeaway: “Our findings support earlier work suggesting social media may fuel ‘hormonophobia,’ or negative framing and scaremongering about hormonal contraception and that this phobia is largely driven by claims of personal experience rather than scientific evidence,” the authors write. “Within these hashtag categories, TikTok creators frame their provider interactions negatively. Many indicate feeling ignored or upset after medical appointments, not sufficiently informed about contraceptive options, and pressured to use hormonal contraceptives. This finding aligns with previous social media research and among the general population, suggesting opportunities for improvements in contraceptive counseling.”
Popular Contraception Videos on TikTok: An Assessment of Content Topics
Rachel E. Stoddard, et al. Contraception, January 2024.The study: Researchers analyzed 700 English-language TikTok videos related to hormonal contraception, with a total of 1.2 billion views and 1.5 million comments, posted between October 2019 and December 2021. Their aim was to explore the types of contraception content on TikTok and to understand how the platform influences the information patients take into birth control counseling visits.
The findings: More than half of the videos (52%) were about patient experiences and how to use contraceptives. Other common topics included side effects (35%) and pregnancy (39%).
Only 19% of the videos were created by health care professionals, including midwives, physician assistants and medical doctors, although those videos garnered 41% of the total views, indicating higher engagement. While 93% of health care providers shared educational content, 23% of non-health care providers shared educational content.
One takeaway: “Our findings show an exceptional opportunity for education around contraception for young reproductive-aged individuals, given the accessibility and popularity of these videos. This may also extend to other topics around sex education and family planning, including sexually transmitted infection prevention and treatment and procuring abortion care,” the authors write.
TikTok, #IUD, and User Experience With Intrauterine Devices Reported on Social Media
Jenny Wu, Esmé Trahair, Megan Happ and Jonas Swartz. Obstetrics & Gynecology, January 2023.The study: Researchers used a web-scraping application to collect the top 100 TikTok videos tagged #IUD on April 6, 2022, based on views, comments, likes and shares. Their aim was to understand the perspectives and experiences of people with IUDs shared on TikTok. The videos had a total of 471 million views, 32 million likes and 1 million shares. Their average length was 33 seconds.
The findings: Some 89% of the creators identified as female and nearly 90% were from the United States; 37% were health care professionals; and 78% were 21 years or older.
Video types included patients’ own experiences with IUD removal (32%), educational (30%) and humorous (25%). More videos (38%) had a negative tone compared with 19% with a positive tone. The videos that portrayed negative user experiences emphasized pain and distrust of health care professionals.
Half of the videos were very accurate, while nearly a quarter were inaccurate (the authors did not use the term misinformation).
One takeaway: “The most liked #IUD videos on TikTok portray negative experiences related to pain and informed consent. Awareness of this content can help health care professionals shape education given the high prevalence of TikTok use among patients,” the authors write. “TikTok differs from other platforms because users primarily engage with an algorithmically curated feed individualized to the user’s interests and demographics.”
Types of female birth control
Most female hormonal contraceptives contain the synthetic version of natural female hormones estrogen and progesterone. They affect women’s hormone levels, preventing mature eggs from being released by the ovaries, a process that’s known as ovulation, hence, preventing a possible pregnancy.
Of the two hormones, progesterone (called progestin in synthetic form) is primarily responsible for preventing pregnancy. In addition to playing a role in preventing ovulation, progesterone inhibits sperm from penetrating through the cervix. Estrogen inhibits the development of follicles in the ovaries.
The information below is sourced from the CDC, the National Library of Medicine, the Cleveland Clinic and the Mayo Clinic.
Intrauterine contraception
Also called Long-Acting Reversible Contraception, or LARC, this method works by thickening the cervical mucus so the sperm can’t reach an egg. There are two types of IUDs: hormonal and non-hormonal.
- Levonorgestrel intrauterine system is a T-shaped device that’s placed inside the uterus by a doctor. It releases a small amount of progestin daily to prevent pregnancy. It can stay in place for 3 to 8 years. Its failure rate is 0.1% to 0.4%.
- Copper T intrauterine device is also T-shaped and is placed inside the uterus by a doctor. It does not contain hormones and can stay in place for up to 10 years. Its failure rate is 0.8%.
- Side effects: Copper IUDs may cause more painful and heavy periods, while progestin IUDs may cause irregular bleeding. In the very rare cases of pregnancy while having an IUD, there’s a greater chance of an ectopic pregnancy, which is when a fertilized egg grows outside of the uterus.
Hormonal methods
- The implant is a single, thin rod that’s inserted under the skin of the upper arm. It releases progestin over 3 years. Its failure rate is 0.1%, making it the most effective form of contraception available.
- Side effects: The most common side effect of an implant is irregular bleeding.
- The injection Depo-Provera or “shot” or “Depo” delivers progestin in the buttocks or arms every three months at the doctor’s office. Its failure rate is 4%.
- Side effects: The shot may cause irregular bleeding. The shot is also the only contraceptive that may cause weight gain. It may also be more difficult to predict when fertility returns once the shot is stopped.
- Combined oral contraceptives or “the pill” contain estrogen and progestin. They’re prescribed by a doctor. The pill has to be taken at the same time daily. The pill is not recommended for people who are older than 35 and smoke, have a history of blood clots or breast cancer. Its failure rate is 7%. Among women aged 15 to 44 who use contraception, about 25% use the pill.
- The skin patch is worn on the lower abdomen, buttocks or upper body, releasing progestin and estrogen. It is prescribed by a doctor. A new patch is used once a week for three weeks. No patch is worn for the fourth week. Its failure rate is 7%.
- Hormonal vaginal contraceptive ring releases progestin and estrogen. It’s placed inside the vagina. It is worn for three weeks and taken out on the fourth week. Its typical failure rate is 7%.
- Side effects: Contraceptives with estrogen, including the pill, the patch and the ring, increase the risk of developing blood clots.
- Progestin-only pill or “mini-pill” only has progestin and is prescribed by a doctor. It has to be taken daily at the same time. It may be a good option for women who can’t take estrogen. Its typical failure rate is 7%.
- Opill is the first over-the-counter daily oral contraceptive in the U.S., approved by the Food and Drug Administration in 2023. Opill only has progestin and like other birth control pills, it has to be taken at the same time every day. It should not be used by those who have or have had breast cancer. Its failure rate is 7%.
- Side effects: The most common side effect of progestin-only pills is irregular bleeding, although the bleeding tends to be light.
Non-hormonal birth control methods include using barriers such as a diaphragm or sponge, condoms and spermicides, withdrawal, and menstrual cycle tracking. Emergency contraception, including emergency contraception pills (the morning-after pill), is not a regular method of birth control.
Additional research studies to consider
Population Attitudes Toward Contraceptive Methods Over Time on a Social Media Platform
Allison A. Merz, et al. American Journal of Obstetrics & Gynecology, December 2020.Social Media and the Intrauterine Device: A YouTube Content Analysis
Brian T. Nguyen and Allison J. Allen. BMJ Sexual and Reproductive Health, November 2017.This article first appeared on The Journalist’s Resource and is republished here under a Creative Commons license.

Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How we can prepare for future public health emergencies
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
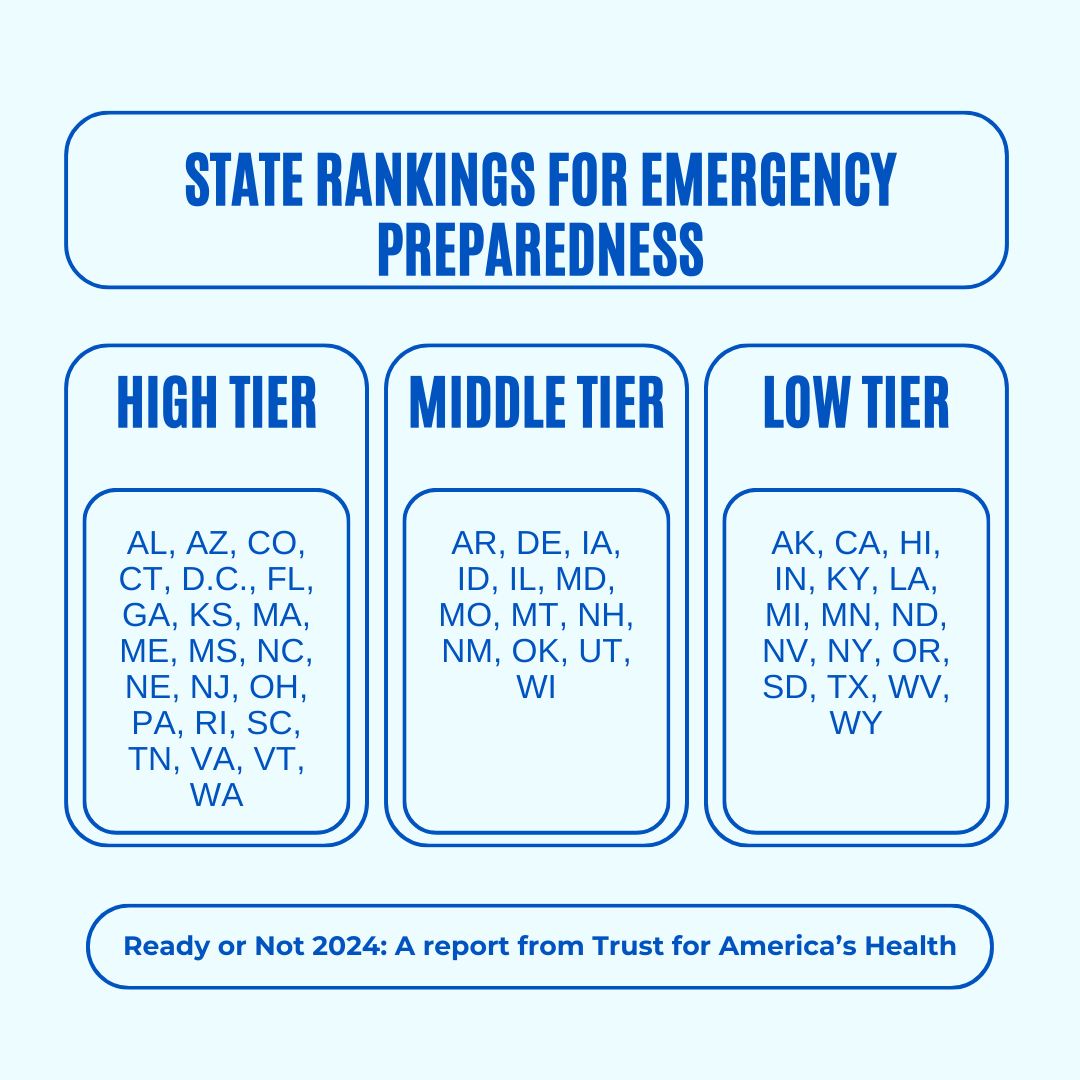
The U.S. is experiencing an increasing number of disease outbreaks and extreme weather events. While state and national preparedness for public health emergencies has improved in some areas, dangerous gaps remain, says a recent report from Trust for America’s Health.
Titled, “Ready or Not 2024: Protecting the Public’s Health from Diseases, Disasters, and Bioterrorism,” the report identifies gaps in national and state preparedness for public health emergencies and provides recommendations for improvement.
Using nine key indicators, the report categorizes all U.S. states and the District of Columbia into three readiness levels: high, medium, and low. The writers hope the report will help policymakers in under-performing states improve public health infrastructure.
Read on to learn more about what the research found and how we can individually prepare for future public health emergencies.
There’s work to be done
The report highlights areas with strong performance as well as those that need improvement.
Some areas with strong performance:
- State public health funding: Most states and the District of Columbia either maintained or increased their public health funding during the 2023 fiscal year.
- Health care labor force preparedness: Most states have started expanding the health care labor force for improved emergency response. As of 2023, 39 states participated in the Nurse Licensure Compact, which allows nurses to work in multiple member states without the need for additional state licenses.
Some areas that need improvement:
- Hospital safety scores: Only 25 percent of acute care hospitals earned the highest patient safety grade in fall 2023. These scores measure health care-associated infection rates, intensive care unit capacity, and other metrics. More high-scoring hospitals would improve preparedness for future public health emergencies.
- Access to paid time off: From March 2018 to March 2023, only 55 percent of U.S. workers used paid time off. Access to paid time off is important for reducing the spread of infectious diseases.
We can all do our part by staying up to date on vaccines
While the report focuses on policy changes that would improve emergency preparedness, Trust for America’s Health’s research identifies one way that we can individually prepare for future public health emergencies: staying up to date on vaccines.
The report found that during the 2022-2023 flu season, only 49 percent of those eligible for the flu vaccine received it. Public health experts are concerned that false claims about COVID-19 vaccines have resulted in overall vaccine hesitancy.
A decline in vaccination rates has led to an uptick in life-threatening, vaccine-preventable diseases, such as measles. Increasing vaccine uptake would prevent the spread of vaccine-preventable diseases and reduce strain on hospital systems during public health crises.
Make sure that you and your children have received all recommended vaccines to prevent severe illness, hospitalization, and death. Learn more about recommended vaccines for adults and children from the CDC.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: