Strawberries vs Raspberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing strawberries to raspberries, we picked the raspberries.
Why?
They’re both very respectable fruits, of course! But it’s not even close, and there is a clear winner here…
In terms of macros, the biggest difference is that raspberries have moderately more carbs, and more than 3x the fiber. Technically they also have 2x the protein, but that’s a case of “two times almost nothing is still almost nothing”. All in all, and especially for the “more than 3x the fiber” (6.5g/100g to strawberries’ 2g/100g), this one’s an easy win for raspberries.
When it comes to vitamins, strawberries have more vitamin C, while raspberries have more of vitamins A, B1, B2, B3, B5, B6, E, K, and choline. Another clear and easy win for raspberries.
In the category of minerals, guess what, raspberries win this hands-down, too: strawberries are higher in selenium, while raspberries have more calcium, copper, iron, magnesium, manganese, phosphorus, and zinc.
Adding up all the individual wins (all for raspberries), it’s not hard to say that raspberries win the day. Still, of course, enjoy either or both; diversity is good!
Want to learn more?
You might like to read:
From Apples to Bees, and High-Fructose Cs: Which Sugars Are Healthier, And Which Are Just The Same?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Want To Age More Slowly? These 4 Social Factors Count The Most

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You probably know that social connection is vital for good health, and perhaps even that loneliness and isolation literally kill.
Indeed, “a lonely lifestyle” vs “family visit frequency” made it into the list of The Lifestyle Factors That Matter >8 Times More Than Genes
In the case of social connection, it:
- Maintains the parts of our brains needed for language and processing social cues
- Brings us social support in a way that will generally be protective against depression
- Means that when all goes wrong, we more likely have material support too
In the case of loneliness and isolation, it:
- Allows important parts of our brain to atrophy
- Will tend towards promoting depression, which can lead to suicidality (and at the very least a decline of physical health, even without suicidality)
- Means that if we slip in the shower, someone will find our body a month later
We wrote about some of these things, here: How To Beat Loneliness & Isolation
Cumulative social advantages
Researchers (Dr. Laura Kubzansky et al.) looked into biomarkers of epigenetic aging and systemic inflammation (which latter thing promotes many kinds of biological aging), and how they are affected by social factors.
Four key areas stood out:
- The warmth and support you received from your parents growing up
- How connected you feel to your community and neighborhood
- Your involvement in religious or faith-based communities
- The reliability of ongoing emotional support from friends and family
They hypothesized—correctly—that these factors would be inversely associated with the pro-aging epigenetic pathways and inflammatory biomarkers for which they were testing.
However, what surprised them was that this effect was cumulative over time, and had no significant associations with short-term stress markers (like cortisol, for example).
Now, some of these things are not modifiable—we can’t do much about our childhoods (alas).
Others are much more attainable for most people, like community involvement.
Religiousness… Well, we are a health science publication and don’t cover theology here, but it’s well-established that faith generally has benefits for social and mental health. It may or may not be something that a person can choose whether to have or not (any more than we can decide whether to believe the sky is green), but if you have some faith, there’s a fair argument for leaning into that rather than away from it, and by making your religious practice communal rather than solitary, if your circumstances allow.
As for that last item, the ongoing emotional support from friends and family, sometimes it can be difficult, for example, we wrote about Family Estrangement & How To Fix It.
But even without family, friends should be an option for anyone. Even if we are physically isolated, for example: Human Connection In An All-Too-Busy World ← this covers, amongst other things, how to get the most out of the options afforded to us by technology, allowing tech to enhance, rather than detract from, our social lives.
And while we’re at it, you might also want to Make Social Media Work For Your Mental Health, Rather Than Against It ← spoiler: no, it’s not about setting app timers!
Anyway, to read the paper in full, enjoy: Cumulative social advantage is associated with slower epigenetic aging and lower systemic inflammation
Want to learn more?
Check out this excellent book that we reviewed a while back:
…and, for that matter, for those of us who are for one reason or another unpartnered and for one reason or another intend to stay that way now:
The Other Significant Others: Reimagining Life with Friendship at the Center by Rhaina Cohen
…and for anyone who wants/needs it, do also check out our main feature: Singledom & Healthy Longevity
Enjoy!
Share This Post
-

The Wim Hof Method – by Wim Hof
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In Wednesday’s main feature, we wrote about the Wim Hof Method, and/but only scratched the surface. Such is the downside of being a super-condensed newsletter! However, it does give us the opportunity to feature the book:
The Wim Hof Method is definitely loudly trumpeted as “up there” with Atomic Habits or How Not To Die in the category of “life-changing” books. Why?
Firstly, it’s a very motivational book. Hof is a big proponent of the notion “if you think you can or you think you can’t, you’re right” idea, practises what he preaches, and makes clear he’s not special.
Secondly, it’s backed up with science. While it’s not a science-heavy book and that’s not the main focus, there are references to studies. Where physiological explanations are given for how certain things work, those explanations are sound. There’s no pseudoscience here, which is especially important for a book of this genre!
What does the book have that our article didn’t? A good few things:
- More about Hof’s own background and where it’s taken him. This is generally not a reason people buy books (unless they are biographies), but it’s interesting nonetheless.
- A lot more advice, data, and information about Cold Therapy and how it can (and, he argues convincingly, should) be built into your life.
- A lot about breathing exercises that we just didn’t cover at all in our article, but is actually an important part of the Wim Hof Method.
- More about stepping through the psychological barriers that can hold us back.
Bottom line: this book offers benefits that stretch into many areas of life, from some simple habits that can be built.
Share This Post
-
7 Fruits Every Senior Should Eat Today (And Why)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What will you prioritize in the new year?
Fruits to enjoy regularly
The 7 fruits recommended for seniors in this video are:
Apples
- Rich in soluble fiber (pectin) for lowering LDL cholesterol.
- Contains phytochemicals such as quercetin and other polyphenols that reduce inflammation and support heart health.
- High in vitamin C for immunity, skin elasticity, and joint health.
Bananas
- Natural energy boost from carbohydrates.
- High in potassium for regulating blood pressure, fluid balance, and preventing muscle cramps.
- Supports cardiovascular health and muscle function.
Avocados
- Rich in monounsaturated fats to improve cholesterol levels.
- High in potassium for blood pressure regulation.
- Contains vitamins E and K for brain health and bone density.
Grapes
- Hydrating and rich in antioxidants like resveratrol, which supports circulation and reduces inflammation.
- Contain vitamins C and K for immunity and bone health.
Plums
- Natural laxative with high fiber and sorbitol for digestive health.
- Rich in potassium and vitamin K for bone density and reducing osteoporosis risk.
- Contain polyphenols for reducing inflammation and supporting cognitive health.
Pomegranates
- Anti-inflammatory and antioxidant-rich (especially punicalagins and anthocyanins).
- Supports heart health, improves cholesterol levels, and promotes brain health.
- May help inhibit cancer cell growth in specific types.
Kiwi
- High in vitamin C to boost immunity.
- Rich in fiber and enzymes for digestive health.
- Low glycemic index, suitable for blood sugar management.
10almonds note: a lot of those statements can go for a lot of fruits, but those are definitely high on the list for the qualities mentioned!
For more on all the above, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Top 8 Fruits That Prevent & Kill Cancer ← there are two fruits that appear on both lists!
Take care!
Share This Post

Related Posts
-

Getting to Neutral – by Trevor Moawad
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We all know that a pessimistic outlook is self-defeating… And yet, toxic positivity can also be a set-up for failure! At some point, reckless faith in the kindly nature of the universe will get crushed, badly. Sometimes that point is a low point in life… sometimes it’s six times a day. But one thing’s for sure: we can’t “just decide everything will go great!” because the world just doesn’t work that way.
That’s where Trevor Moawad comes in. “Getting to neutral” is not a popular selling point. Everyone wants joy, abundance, and high after high. And neutrality itself is often associated with boredom and soullessness. But, Moawad argues, it doesn’t have to be that way.
This book’s goal—which it accomplishes well—is to provide a framework for being a genuine realist. What does that mean?
“I’m not a pessimist; I’m a realist” – every pessimist ever.
^Not that. That’s not what it means. What it means instead is:
- Hope for the best
- Prepare for the worst
- Adapt as you go
…taking care to use past experiences to inform future decisions, but without falling into the trap of thinking that because something happened a certain way before, it always will in the future.
To be rational, in short. Consciously and actively rational.
Feel the highs! Feel the lows! But keep your baseline when actually making decisions.
Bottom line: this book is as much an antidote to pessimism and self-defeat, as it is to reckless optimism and resultant fragility. Highly recommendable.
Click here to check out “Getting to Neutral” and start creating your best, most reason-based life!
PS: in this book, Moawad draws heavily from his own experiences of battling adversity in the form of cancer—of which he died, before this book’s publication. A poignant reminder that he was right: we won’t always get the most positive outcome of any given situation, so what matters the most is making the best use of the time we have.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Some women’s breasts can’t make enough milk, and the effects can be devastating
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many new mothers worry about their milk supply. For some, support from a breastfeeding counsellor or lactation consultant helps.
Others cannot make enough milk no matter how hard they try. These are women whose breasts are not physically capable of producing enough milk.
Our recently published research gives us clues about breast features that might make it difficult for some women to produce enough milk. Another of our studies shows the devastating consequences for women who dream of breastfeeding but find they cannot.
Some breasts just don’t develop
Unlike other organs, breasts are not fully developed at birth. There are key developmental stages as an embryo, then again during puberty and pregnancy.
At birth, the breast consists of a simple network of ducts. Usually during puberty, the glandular (milk-making) tissue part of the breast begins to develop and the ductal network expands. Then typically, further growth of the ductal network and glandular tissue during pregnancy prepares the breast for lactation.
But our online survey of women who report low milk supply gives us clues to anomalies in how some women’s breasts develop.
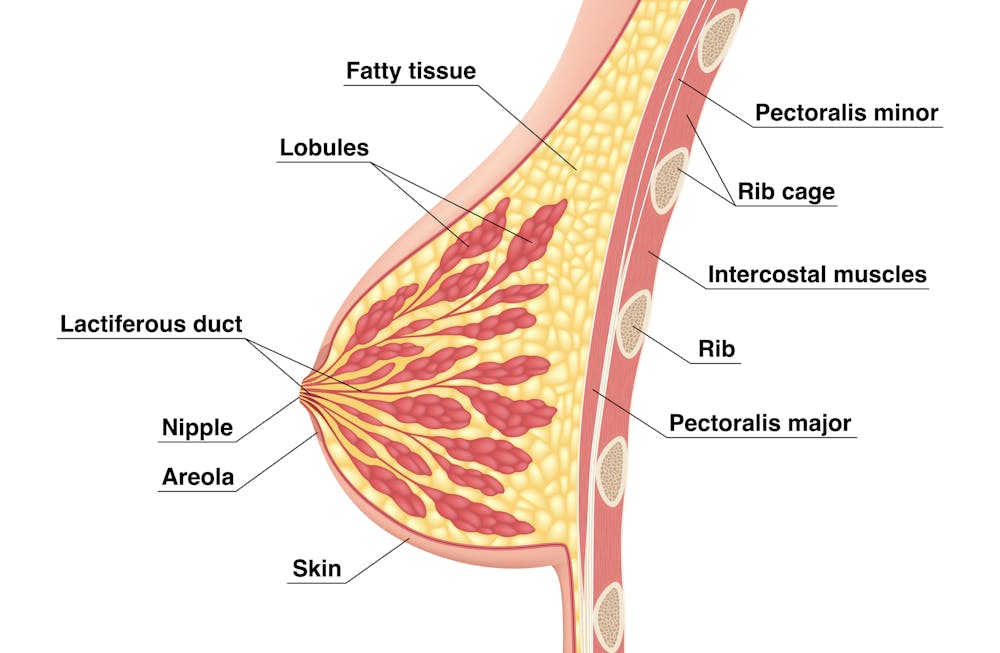
We’re not talking about women with small breasts, but women whose glandular tissue (shown in this diagram as “lobules”) is underdeveloped and have a condition called breast hypoplasia.

Sometimes not enough glandular tissue, shown here as lobules, develop.
Tsuyna/ShutterstockWe don’t know how common this is. But it has been linked with lower rates of exclusive breastfeeding.
We also don’t know what causes it, with much of the research conducted in animals and not humans.
However, certain health conditions have been associated with it, including polycystic ovary syndrome and other endocrine (hormonal) conditions. A high body-mass index around the time of puberty may be another indicator.
Could I have breast hypoplasia?
Our survey and other research give clues about who may have breast hypoplasia.
But it’s important to note these characteristics are indicators and do not mean women exhibiting them will definitely be unable to exclusively breastfeed.
Indicators include:
- a wider than usual gap between the breasts
- tubular-shaped (rather than round) breasts
- asymmetric breasts (where the breasts are different sizes or shapes)
- lack of breast growth in pregnancy
- a delay in or absence of breast fullness in the days after giving birth
In our survey, 72% of women with low milk supply had breasts that did not change appearance during pregnancy, and about 70% reported at least one irregular-shaped breast.
The effects
Mothers with low milk supply – whether or not they have breast hyoplasia or some other condition that limits their ability to produce enough milk – report a range of emotions.
Research, including our own, shows this ranges from frustration, confusion and surprise to intense or profound feelings of failure, guilt, grief and despair.
Some mothers describe “breastfeeding grief” – a prolonged sense of loss or failure, due to being unable to connect with and nourish their baby through breastfeeding in the way they had hoped.
These feelings of failure, guilt, grief and despair can trigger symptoms of anxiety and depression for some women.
Feelings of failure, guilt, grief and despair were common.
Bricolage/ShutterstockOne woman told us:
[I became] so angry and upset with my body for not being able to produce enough milk.
Many women’s emotions intensified when they discovered that despite all their hard work, they were still unable to breastfeed their babies as planned. A few women described reaching their “breaking point”, and their experience felt “like death”, “the worst day of [my] life” or “hell”.
One participant told us:
I finally learned that ‘all women make enough milk’ was a lie. No amount of education or determination would make my breasts work. I felt deceived and let down by all my medical providers. How dare they have no answers for me when I desperately just wanted to feed my child naturally.
Others told us how they learned to accept their situation. Some women said they were relieved their infant was “finally satisfied” when they began supplementing with formula. One resolved to:
prioritise time with [my] baby over pumping for such little amounts.
Where to go for help
If you are struggling with low milk supply, it can help to see a lactation consultant for support and to determine the possible cause.
This will involve helping you try different strategies, such as optimising positioning and attachment during breastfeeding, or breastfeeding/expressing more frequently. You may need to consider taking a medication, such as domperidone, to see if your supply increases.
If these strategies do not help, there may be an underlying reason why you can’t make enough milk, such as insufficient glandular tissue (a confirmed inability to make a full supply due to breast hypoplasia).
Even if you have breast hypoplasia, you can still breastfeed by giving your baby extra milk (donor milk or formula) via a bottle or using a supplementer (which involves delivering milk at the breast via a tube linked to a bottle).
More resources
The following websites offer further information and support:
- Australian Breastfeeding Association
- Lactation Consultants of Australia and New Zealand
- Royal Women’s Hospital, Melbourne
- Supply Line Breastfeeders Support Group of Australia Facebook support group
- IGT And Low Milk Supply Support Group Facebook support group
- Breastfeeding Medicine Network Australia/New Zealand
- Supporting breastfeeding grief (a collection of resources).
Shannon Bennetts, a research fellow at La Trobe University, contributed to this article.

Renee Kam, PhD candidate and research officer, La Trobe University and Lisa Amir, Professor in Breastfeeding Research, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Cancer patients from migrant backgrounds have a 1 in 3 chance of something going wrong in their care
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
More than 7 million people in Australia were born overseas. Some 5.8 million people report speaking a language other than English at home.
But how well are we looking after culturally and linguistically diverse (CALD) Australians?
In countries around the world, evidence suggests people from CALD backgrounds are at increased risk of harm as a result of the health care they receive when compared to the general population. Common problems include a higher risk of contracting a hospital-acquired infection or medication errors.
People receiving cancer care are at particularly high risk of harm associated with their health care.
In a recent study, we found CALD cancer patients in Australia had roughly a one-in-three risk of something going wrong during their cancer care. This is unacceptably high.
SeventyFour/Shutterstock We reviewed medical records
We worked with four cancer services (two in New South Wales and two in Victoria) that provide care to high proportions of people from CALD backgrounds. These four cancer services offer a combination of care to patients in hospitals, clinics and in their homes.
We analysed de-identified medical records of people from CALD backgrounds who received care at any of the four cancer services during 2018. To identify CALD patients, we used information from their medical records including “country of birth”, “preferred language”, “language spoken at home” and “interpreter required”.
We reviewed a total of 628 medical records of CALD cancer patients. We found roughly one in three medical records (212 out of 628) had at least one patient safety event recorded. We defined a patient safety event as any event that could have or did result in harm to the patient as a result of the health care they receive. We also found 44 patient records had three or more safety events recorded over a 12-month period.
Medication-related safety events were common, such as the wrong medication type or dose being given to a patient. Sometimes the patients themselves took the wrong type or dose of a medication or stopped medication all together. We also observed a variety of other patient safety events such as falls, pressure ulcers and infections after surgery.
The number of incidents could even be higher than what we observed. We know from other research that not all patient safety events are documented.
Our research looked at patient safety incidents among CALD patients at four Australian cancer services in 2018. Monkey Business Images/Shutterstock We didn’t have a control group, which is the main limitation of our study. In other words, we didn’t examine medical records of patients from non-CALD backgrounds to compare how common patient safety events were between groups.
But looking at other data suggests the rate of incidents is much higher in CALD patients.
Studies over many years indicate around one in ten patients admitted to hospital experience a safety event.
One study from Norway found cancer patients have a 39% greater risk of experiencing adverse events in hospital when compared to other patients (24.2% compared to 17.4%).
Why is the risk of incidents so high for CALD patients?
We identified miscommunication as a key factor that put cancer patients from CALD backgrounds at risk.
For example, we observed from one patient’s notes that the patient didn’t take their medication because they were confused by the instructions given by different clinicians. This confusion might have stemmed from language barriers or health literacy issues.
In some medical records, we also saw interpreter requirements were unmet. For example, at the time of admission, assessment for language needs noted an interpreter was not required. However, later notes mentioned the patient had poor English or needed an interpreter.
Also, with the limited availability of interpreters, they’re often reserved for specialist appointments, and not used for “routine” tasks, such as during chemotherapy treatment. This may result in side effects from cancer medications not being properly identified and responded to, potentially leading to patient harm.
Risks may increase if a patient needs an interpreter but doesn’t have one. THICHA SATAPITANON/Shutterstock What can we do to improve things?
To make care safer, patients, their families and the clinicians who care for them should come together so that any solutions developed are practical, relevant, and informed by their combined experiences.
As an example, we developed a tool with consumers from CALD backgrounds and their clinicians that seeks to ensure that when patient medications are changed, there is common understanding between the clinician and the patient of their medication and care instructions. This includes recognising the side effects of the medications and who to contact if they have concerns.
This tool uses images and simple language to support common understanding of medication and care instructions. It takes into account specific cultural expectations and is available in different languages. It’s currently being evaluated in two cancer clinics.
To make cancer care safer for patients from CALD backgrounds, health systems and services will need to support and invest in strategies that are specifically targeted towards people from these backgrounds. This will ensure more equitable health solutions that improve the health of all Australians.
Ashfaq Chauhan, Research Fellow, Australian Institute of Health Innovation, Macquarie University; Melvin Chin, Senior Lecturer, School of Clinical Medicine, UNSW Sydney; Meron Pitcher, Honorary, Medicine, Dentistry and Health Sciences, The University of Melbourne, and Reema Harrison, Professor, Australian Institute of Health Innovation, Macquarie University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: