Self-Compassion In A Relationship (Positives & Pitfalls)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Practise Self-Compassion In Your Relationship (But Watch Out!)
Let’s make clear up-front: this is not about “…but not too much”.
With that in mind…
Now let’s set the scene: you, a happily-partnered person, have inadvertently erred and upset your partner. They may or may not have already forgiven you, but you are still angry at yourself.
Likely next steps include all or any of:
- continuing to apologise and try to explain
- self-deprecatory diatribes
- self-flagellation, probably not literally but in the sense of “I don’t deserve…” and acting on that feeling
- self-removal, because you don’t want to further inflict your bad self on your partner
As you might guess, these are quite varied in their degree of healthiness:
- apologising is good, as even is explaining, but once it’s done, it’s done; let it go
- self-deprecation is pretty much never useful, let alone healthy
- self-flagellation likewise; it is not only inherently self-destructive, but will likely create an additional problem for your partner too
- self-removal can be good or bad depending on the manner of that removal: there’s a difference between just going cold and distant on your partner, and saying “I’m sorry; this is my fault not yours, I don’t want to take it out on you, so please give me half an hour by myself to regain my composure, and I will come back with love then if that’s ok with you”
About that last: mentioning the specific timeframe e.g. “half an hour” is critical, by the way—don’t leave your partner hanging! And then do also follow through on that; come back with love after the half-hour elapses. We suggest mindfulness meditation in the interim (here’s our guide to how), if you’re not sure what to do to get you there.
To Err Is Human; To Forgive, Healthy (Here’s How To Do It) ← this goes for when the forgiveness in question is for yourself, too—and we do write about that there (and how)!
This is important, by the way; not forgiving yourself can cause more serious issues down the line:
If, by the way, you’re hand-wringing over “but was my apology good enough really, or should I…” then here is how to do it. Basically, do this, and then draw a line under it and consider it done:
The Apology Checklist ← you’ll want to keep a copy of this, perhaps in the notes app on your phone, or a screenshot if you prefer
(the checklist is at the bottom of that page)
The catch
It’s you, you’re the catch 👈👈😎
Ok, that being said, there is actually a catch in the less cheery sense of the word, and it is:
“It is important to be compassionate about one’s occasional failings in a relationship” does not mean “It is healthy to be neglectful of one’s partner’s emotional needs; that’s self-care, looking after #1; let them take care of themself too”
…because that’s simply not being a couple at all.
Think about it this way: the famous airline advice,
“Put on your own oxygen mask before helping others with theirs”
…does not mean “Put on your own oxygen mask and then watch those kids suffocate; it’s everyone for themself”
So, the same goes in relationships too. And, as ever, we have science for this. There was a recent (2024) study, involving hundreds of heterosexual couples aged 18–73, which looked at two things, each measured with a scaled questionnaire:
- Subjective levels of self-compassion
- Subjective levels of relationship satisfaction
For example, questions included asking participants to rate, from 1–5 depending on how much they felt the statements described them, e.g:
In my relationship with my partner, I:
- treat myself kindly when I experience sorrow and suffering.
- accept my faults and weaknesses.
- try to see my mistakes as part of human nature.
- see difficulties as part of every relationship that everyone goes through once.
- try to get a balanced view of the situation when something unpleasant happens.
- try to keep my feelings in balance when something upsets me.
Note: that’s not multiple choice! It’s asking participants to rate each response as applicable or not to them, on a scale of 1–5.
And…
❝Women’s self-compassion was also positively linked with men’s total relationship satisfaction. Thus, men seem to experience overall satisfaction with the relationship when their female partner is self-kind and self-caring in difficult situations.
Unexpectedly, however, we found that men’s relationship-specific self-compassion was negatively associated with women’s fulfillment.
Baker and McNulty (2011) reported that, only for men, a Self-Compassion x Conscientiousness interaction explained whether the positive effects of self-compassion on the relationship emerged, but such an interaction was not found for women.
Highly self-compassionate men who were low in conscientiousness were less motivated than others to remedy interpersonal mistakes in their romantic relationships, and this tendency was in turn related to lower relationship satisfaction❞
~ Dr. Astrid Schütz et al. (2024)
And if you’d like to read the cited older paper from 2011, here it is:
Read in full: Self-compassion and relationship maintenance: the moderating roles of conscientiousness and gender
The take-away here is not: “men should not practice self-compassion”
(rather, they absolutely should)
The take-away is: we must each take responsibility for managing our own mood as best we are able; practice self-forgiveness where applicable and forgive our partner where applicable (and communicate that!)…. And then go consciously back to the mutual care on which the relationship is hopefully founded.
Which doesn’t just mean love-bombing, by the way, it also means listening:
The Problem With Active Listening (And How To Do Better)
To close… We say this often, but we mean it every time: take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Whole-Body Approach to Osteoporosis – by Keith McCormick

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You probably already know to get enough calcium and vitamin D, and do some resistance training. What does this book offer beyond that advice?
It’s pretty comprehensive, as it turns out. It covers the above, plus the wide range of medications available, what supplements help or harm or just don’t have enough evidence either way yet, things like that.
Amongst the most important offerings are the signs and symptoms that can help monitor your bone health (things you can do at home! Like examinations of your fingernails, hair, skin, tongue, and so forth, that will reveal information about your internal biochemical make-up), as well as what lab tests to ask for. Which is important, as osteoporosis is one of those things whereby we often don’t learn something is wrong until it’s too late.
The author is a chiropractor, which doesn’t always have a reputation as the most robustly science-based of physical therapy options, but he…
- doesn’t talk about chiropractic
- did confer with a flock of experts (osteopaths, nutritionists, etc) to inform/check his work
- does refer consistently to good science, and explains it well
- includes 16 pages of academic references, and yes, they are very reputable publications
Bottom line: this one really does give what the subtitle promises: a whole body approach to avoiding (or reversing) osteoporosis.
Click here to check out The Whole Body Approach To Osteoporosis; sooner is better than later!
Share This Post
-

Are You Stuck Playing These Three Roles in Love?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The psychology of Transactional Analysis holds that our interpersonal dynamics can be modelled in the following fashion:
The roles
- Child: vulnerable, trusting, weak, and support-seeking
- Parent: strong, dominant, responsible—but also often exhausted and critical
- Adult: balanced, thoughtful, creative, and kind
Ideally we’d be able to spend most of our time in “Adult” mode, and occasionally go into “Child” or “Parent” mode when required, e.g. child when circumstances have rendered us vulnerable and we need help; parent when we need to go “above and beyond” in the pursuit of looking after others. That’s all well and good and healthy.
However, in relationships, often it happens that partners polarize themselves and/or each other, with one shouldering all of the responsibility, and the other willfully losing their own agency.
The problem lies in that either role can be seductive—on the one hand, it’s nice to be admired and powerful and it’s a good feeling to look after one’s partner; on the other hand, it’s nice to have someone who will meet your every need. What love and trust!
Only, it becomes toxic when these roles stagnate, and each forgets how to step out of them. Each can become resentful of the other (for not pulling their weight, on one side, and for not being able to effortlessly solve all life problems unilaterally and provide endlessly in both time and substance, on the other), digging in to their own side and exacerbating the less healthy qualities.
As to the way out? It’s about self-exploration and mutual honesty—and mutual support:
Click Here If The Embedded Video Doesn’t Load Automatically!
Further reading
While we haven’t (before today) written about TA per se, we have previously written about AT (Attachment Theory), and on this matter, the two can overlap, where certain attachment styles can result in recreating parent/child/adult dynamics:
How To Leverage Attachment Theory In Your Relationship ← this is about understanding and recognizing attachment styles, and then making sure that both you and your partner(s) are armed with the necessary knowledge and understanding to meet each other’s needs.
Take care!
Share This Post
-

The Brain-Skin Doctor
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Of Brains And Breakouts
Today’s spotlight is on Dr. Claudia Aguirre. She’s a molecular neuroscientist, and today she’s going to be educating us about skin.
What? Why?
When we say “neuroscience”, we generally think of the brain. And indeed, that’s a very important part of it.
We might think about eyes, which are basically an extension of the brain.
We don’t usually think about skin, which (just like our eyes) is constantly feeding us a lot of information about our surroundings, via a little under three million nerve endings. Guess where the other ends of those nerves lead!
There’s a constant two-way communication going on between our brain and our skin.
What does she want us to know?
Psychodermatology
The brain and the skin talk to each other, and maladies of one can impact the other:
- Directly, e.g. stress prompting skin breakouts (actually this is a several-step process physiologically, but for the sake of brevity we’ll call this direct)
- Indirectly, e.g. nervous disorders that result in people scratching or picking at their skin, which prompts a whole vicious cycle of one thing making the other worse
Read more: Psychodermatology: The Brain-Skin Connection
To address both kinds of problems, clearly something beyond moisturizer is needed!
Mindfulness (meditation and beyond)
Mindfulness is a well-evidenced healthful practice for many reasons, and Dr. Aguirra argues the case for it being good for our skin too.
As she points out,
❝Cultural stress and anxiety can trigger or aggravate many skin conditions—from acne to eczema to herpes, psoriasis, and rosacea.
Conversely, a disfiguring skin condition can trigger stress, anxiety, depression, and even suicide.
Chronic, generalized anxiety can create chronic inflammation and exacerbate inflammatory skin conditions, such as those I mentioned previously.
Chronic stress can result in chronic anxiety, hypervigilance, poor sleep, and a whole cascade of effects resulting in a constant breakdown of tissues and organs, including the skin.❞
So, she recommends mindfulness-based stress reduction (MBSR), for the above reasons, along with others!
Read more: Mind Matters
How to do it: No-Frills, Evidence-Based Mindfulness
And as for “and beyond?”
Do you remember in the beginning of the pandemic, when people were briefly much more consciously trying to avoid touching their faces so much? That, too, is mindfulness. It may have been a stressed and anxious mindfulness for many*, but mindfulness nonetheless.
*which is why “mindfulness-based stress reduction” is not a redundant tautology repeated more than once unnecessarily, one time after another 😉
So: do try to keep aware of what you are doing to your skin, and so far as is reasonably practicable, only do the things that are good for it!
The skin as an endocrine organ
Nerves are not the only messengers in the body; hormones do a lot of our body’s internal communication too. And not just the ones everyone remembers are hormones (e.g. estrogen, testosterone, although yes, they do both have a big impact on skin too), but also many more, including some made in the skin itself!
Dr. Aguirra gives us a rundown of common conditions, the hormones behind them, and what we can do if we don’t want them:
Read more: Rethinking The Skin As An Endocrine Organ
Take-away advice:
For healthy skin, we need to do more than just hydrate, get good sleep, have good nutrition, and get a little sun (but not too much).
- We should also practice mindfulness-based stress reduction, and seek help for more serious mental health issues.
- We should also remember the part our hormones play in our skin, and not just the obvious ones.
Did you know that vitamin D is also a hormone, by the way? It’s not the only hormone at play in your skin by a long way, but it is an important one:
Society for Endocrinology | Vitamin D
Want to know more?
You might like this interview with Dr. Aguirre:
The Brain in Our Skin: An Interview with Dr. Claudia Aguirre
Take care!
Share This Post

Related Posts
-

What’s the difference between miscarriage and stillbirth?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
Former US First Lady Michelle Obama revealed in her memoir she had a miscarriage. UK singer-songwriter and actor Lily Allen has gone on the record about her stillbirth.
Both miscarriage and stillbirth are sadly familiar terms for pregnancy loss. They can be traumatic life events for the prospective parents and family, and their impacts can be long-lasting. But the terms can be confused.
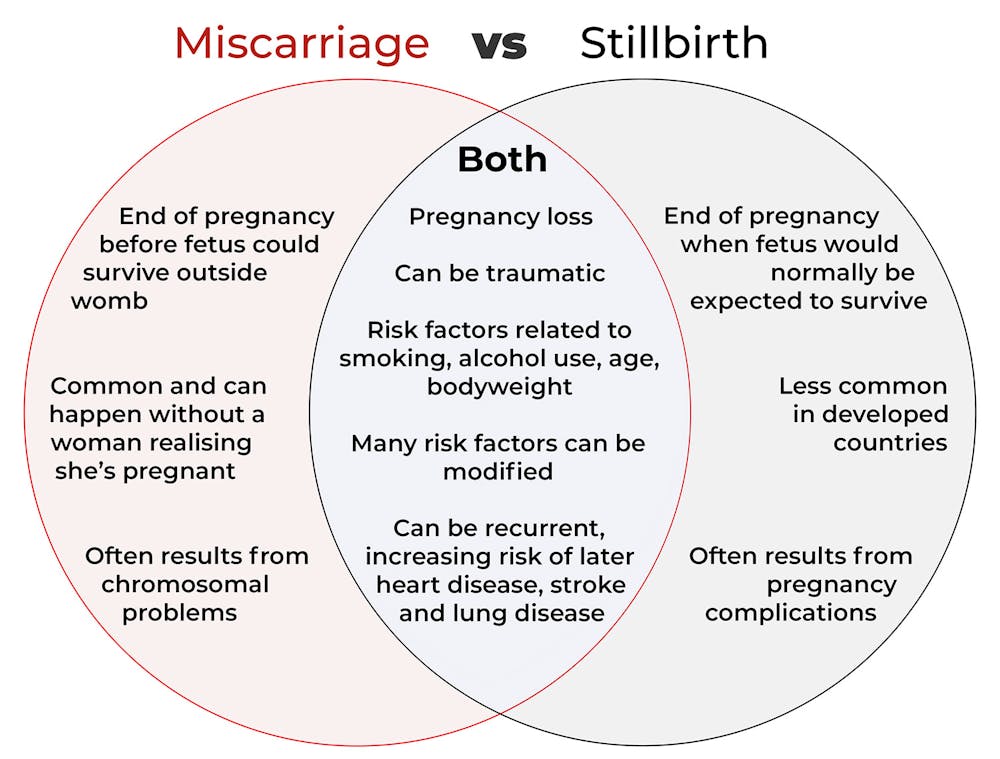
Here are some similarities and differences between miscarriage and stillbirth, and why they matter.

christinarosepix/Shutterstock Let’s start with some definitions
In broad terms, a miscarriage is when a pregnancy ends while the fetus is not yet viable (before it could survive outside the womb).
This is the loss of an “intra-uterine” pregnancy, when an embryo is implanted in the womb to then develop into a fetus. The term miscarriage excludes ectopic pregnancies, where the embryo is implanted outside the womb.
However, stillbirth refers to the end of a pregnancy when the fetus is normally viable. There may have been sufficient time into the pregnancy. Alternatively, the fetus may have grown large enough to be normally expected to survive, but it dies in the womb or during delivery.
The Australian Institute of Health and Welfare defines stillbirth as a fetal death of at least 20 completed weeks of gestation or with a birthweight of at least 400 grams.
Internationally, definitions of stillbirth vary depending on the jurisdiction.
How common are they?
It is difficult to know how common miscarriages are as they can happen when a woman doesn’t know she is pregnant. There may be no obvious symptoms or something that looks like a heavier-than-normal period. So miscarriages are likely to be more common than reported.
Studies from Europe and North America suggest a miscarriage occurs in about one in seven pregnancies (15%). More than one in eight women (13%) will have a miscarriage at some time in her life.
Around 1–2% of women have recurrent miscarriages. In Australia this is when someone has three or more miscarriages with no pregnancy in between.
Australia has one of the lowest rates of stillbirth in the world. The rate has been relatively steady over the past 20 years at 0.7% or around seven per 1,000 pregnancies.
Who’s at risk?
Someone who has already had a miscarriage or stillbirth has an increased risk of that outcome again in a subsequent pregnancy.
Compared with women who have had a live birth, those who have had a stillbirth have double the risk of another. For those who have had recurrent miscarriages, the risk of another miscarriage is four-fold higher.
Some factors have a u-shaped relationship, with the risk of miscarriage and stillbirth lowest in the middle.
For instance, maternal age is a risk factor for both miscarriage and stillbirth, especially if under 20 years old or older than 35. Increasing age of the male is only a risk factor for stillbirth, especially for fathers over 40.
An older dad can be a risk factor for stillbirth, but not miscarriage. Elizaveta Galitckaia/Shutterstock Similarly for maternal bodyweight, women with a body mass index or BMI in the normal range have the lowest risk of miscarriage and stillbirth compared with those in the obese or underweight categories.
Lifestyle factors such as smoking and heavy alcohol drinking while pregnant are also risk factors for both miscarriage and stillbirth.
So it’s important to not only avoid smoking and alcohol while pregnant, but before getting pregnant. This is because early in the pregnancy, women may not know they have conceived and could unwittingly expose the developing fetus.
Why do they happen?
Miscarriage often results from chromosomal problems in the developing fetus. However, genetic conditions or birth defects account for only 7-14% of stillbirths.
Instead, stillbirths often relate directly to pregnancy complications, such as a prolonged pregnancy or problems with the umbilical cord.
Maternal health at the time of pregnancy is another contributing factor in the risk of both miscarriage and stillbirths.
Chronic diseases, such as high blood pressure, diabetes, hypothyroidism (underactive thyroid), polycystic ovary syndrome, problems with the immune system (such as an autoimmune disorder), and some bacterial and viral infections are among factors that can increase the risk of miscarriage.
Similarly mothers with diabetes, high blood pressure, and untreated infections, such as malaria or syphilis, face an increased risk of stillbirth.
In many cases, however, the specific cause of pregnancy loss is not known.
How about the long-term health risks?
Miscarriage and stillbirth can be early indicators of health issues later in life.
For instance, women who have had recurrent miscarriages or recurrent stillbirths are at higher risk of cardiovascular disease (such as heart disease or stroke).
Our research has also looked at the increased risk of stroke. Compared with women who had never miscarried, we found women with a history of three or more miscarriages had a 35% higher risk of non-fatal stroke and 82% higher risk of fatal stroke.
Women who had a stillbirth had a 31% higher risk of a non-fatal stroke, and those who had had two or more stillbirths were at a 26% higher risk of a fatal stroke.
We saw similar patterns in chronic obstructive pulmonary disease or COPD, a progressive lung disease with respiratory symptoms such as breathlessness and coughing.
Our data showed women with a history of recurrent miscarriages or stillbirths were at a 36% or 67% higher risk of COPD, respectively, even after accounting for a history of asthma.
Long-term health risks of recurrent miscarriages or stillbirths include developing lung disease later in life. PRPicturesProduction/Shutterstock Why is all this important?
Being well-informed about the similarities and differences between these two traumatic life events may help explain what has happened to you or a loved one.
Where risk factors can be modified, such as smoking and obesity, this information can be empowering for individuals who wish to reduce their risk of miscarriage and stillbirth and make lifestyle changes before they become pregnant.
More information and support about miscarriage and stillbirth is available from SANDS and Pink Elephants.
Gita Mishra, Professor of Life Course Epidemiology, Faculty of Medicine, The University of Queensland; Chen Liang, PhD student, reproductive history and non-communicable diseases in women, The University of Queensland, and Jenny Doust, Clinical Professorial Research Fellow, School of Public Health, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Breast Milk’s Benefits That Are (So Far) Not Replicable
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Simply The Breast 🎶

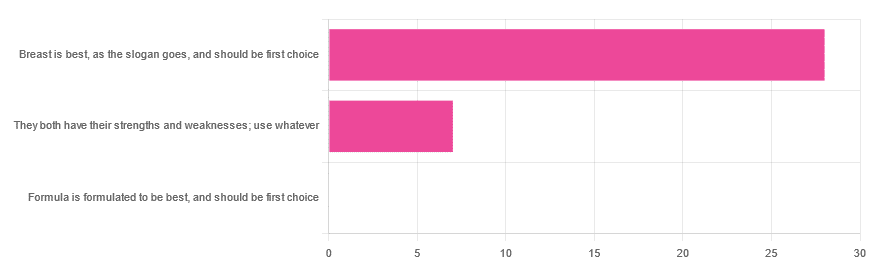
In Wednesday’s newsletter, we asked you for your opinion on breast vs formula milk (for babies!), and got the above-depicted, below-described, set of responses:
- 80% said “Breast is best, as the slogan goes, and should be first choice”
- 20% said “They both have their strengths and weaknesses; use whatever”
- 0% said “Formula is formulated to be best, and should be first choice”
That’s the first time we’ve ever had a possible poll option come back with zero votes whatsoever! It seems this topic is relatively uncontentious amongst our readership, so we’ll keep things brief today, but there is still a little mythbusting to be done.
So, what does the science say?
[Breast milk should be the first choice] at least for the few few weeks and months for the benefit of baby’s health as breast milk has protective factors formula does not: True or False?
True! The wording here was taken from one of our readers’ responses, by the way (thank you, Robin). There are a good number of those protective factors, the most well-known of which is passing on immune cells and cell-like things; in other words, immune-related information being passed from parent* to child.
*usually the mother, though in principle it could be someone else and in practice sometimes it is; the only real requirements are that the other person be healthy, lactating, and willing.
As for immune benefits, see for example:
Perspectives on Immunoglobulins in Colostrum and Milk
And for that matter, also:
(Colostrum is simply the milk that is produced for a short period after giving birth; the composition of milk will tend to change later)
In any case, immunoglobulin A is a very important component in breast milk (colostrum and later), as well as lactoferrin (has an important antimicrobial effect and is good for the newborn’s gut), and a plethora of cytokines:
As for that about the gut, lactoferrin isn’t the only breast milk component that benefits this, by far, and there’s a lot that can’t be replicated yet:
Human Breast Milk and the Gastrointestinal Innate Immune System
As long as your infant/child is nutritiously fed, it shouldn’t matter if it comes from breast or formula: True or False?
False! Formula milk will not convey those immune benefits.
This doesn’t mean that formula-feeding is neglectful; as several people who commented mentioned*, there are many reasons a person may not be able to breastfeed, and they certainly should not be shamed for that.
*(including the reader whose words we borrowed for this True/False item; the words we quoted above were prefaced with: “Not everyone is able to breastfeed for many different reasons”)
But, while formula milk is a very good second choice, and absolutely a respectable choice if breast milk isn’t an option (or an acceptable option) for whatever reason, it still does not convey all the health benefits of breast milk—yet! The day may come when they’ll find a way to replicate the immune benefits, but today is not that day.
They both have their strengths and weaknesses: True or False?
True! But formula’s strengths are only in the category of convenience and sometimes necessity—formula conveys no health benefits that breast milk could not do better, if available.
For many babies, formula means they get to eat, when without it they would starve due to non-availability of breast milk. That’s a pretty important role!
Note also: this is a health science publication, not a philosophical publication, but we’d be remiss not to mention one thing; let’s bring it in under the umbrella of sociology:
The right to bodily autonomy continues to be the right to bodily autonomy even if somebody else wants/needs something from your body.
Therefore, while there are indeed many good reasons for not being able to breastfeed, or even just not being safely* able to breastfeed, it is at the very least this writer’s opinion that nobody should be pressed to give their reason for not breastfeeding; “no” is already a sufficient answer.
*Writer’s example re safety: when I was born, my mother was on such drugs that it would have been a very bad idea for her to breastfeed me. There are plenty of other possible reasons why it might be unsafe for someone one way or another, but “on drugs that have a clear ‘do not take while pregnant or nursing’ warning” is a relatively common one.
All that said, for those who are willing and safely able, the science is clear: breast is best.
Want to read more?
The World Health Organization has a wealth of information (including explanations of its recommendations of, where possible, exclusive breastfeeding for the first 6 months, ideally continuing some breastfeeding for the first 2 years), here:
World Health Organization | Breastfeeding
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Stop Overthinking – by Nick Trenton
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book is exactly what it says on the tin. We are given twenty-three techniques to relieve stress, stop negative spirals, declutter your mind, and focus on the present, in the calm pursuit of good mental health and productivity.
The techniques are things like the RAIN technique above, so if you liked that, you’ll love this. Being a book rather than a newsletter, it also takes the liberty of going into much more detail—hence the 200 pages for 23 techniques. Unlike many books, it’s not packed in fluff either. It’s that perfect combination of “to the point” and “very readable”.
If you’ve read this far into the review and you’re of two minds about whether or not this book could be useful to you, then you just might be overthinking it
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: