Red Light Therapy for 927 Days (Guess What Happened When One Side Broke?)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve talked about the technology before, but this is a very good illustration of its effectiveness:
Shining a light on the science
Robin, from the Science of Self-Care, gives her review. She tried it because research shows improved collagen and elastin production, wound healing, reduced inflammation, pain relief, muscle recovery, sleep quality, mood, and cognitive function.
She originally began using it daily two and a half years years ago to improve skin clarity, brightness, and firmness—but now, her main reason for consistent use is mood enhancement—she feels more energized, positive, and mentally clear after morning sessions. On which note, she wears the mask first thing in the morning for 20–30 minutes, even while travelling; she uses it as a meditative or creative time.
In terms of results for her skin, she enjoyed subtle but noticeable improvements—firmer, smoother skin. However, this was hard to attribute solely to the mask due to other skincare treatments… Until one side of her mask broke.
Because one side of the mask wasn’t working for two weeks, she noticed rougher, redder skin on that side.
You can see her results for yourself, here:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Casting Yourself In A Healthier Light ← our main feature about the science of this
And if you’d like to get one for yourself, then here’s an example product on Amazon 😎
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Sweet Dreams Are Made Of Cheese (Or Are They?)

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝In order to lose a little weight I have cut out cheese from my diet – and am finding that I am sleeping better. Would be interested in your views on cheese and sleep, and whether some types of cheese are worse for sleep than others. I don’t want to give up cheese entirely!❞
In principle, there’s nothing in cheese that, biochemically, should impair sleep. If anything, its tryptophan content could aid good sleep.
Tryptophan is found in many foods, including cheese, which (of common foods, anyway), for example cheddar cheese ranks second only to pumpkin seeds in tryptophan content.
Tryptophan can be converted by the body into 5-HTP, which you’ve maybe seen sold as a supplement. Its full name is 5-hydroxytryptophan.
5-HTP can, in turn, be used to make melatonin and/or serotonin. Which of those you will get more of, depends on what your body is being cued to do by ambient light/darkness, and other environmental cues.
If you are having cheese and then checking your phone, for instance, or otherwise hanging out where there are white/blue lights, then your body may dutifully convert the tryptophan into serotonin (calm wakefulness) instead of melatonin (drowsiness and sleep).
In short: the cheese will (in terms of this biochemical pathway, anyway) augment some sleep-inducing or wakefulness-inducing cues, depending on which are available.
You may be wondering: what about casein?
Casein is oft-touted as producing deep sleep, or disturbed sleep, or vivid dreams, or bad dreams. There’s no science to back any of this up, though the following research review is fascinating:
Dreams of the Rarebit Fiend: food and diet as instigators of bizarre and disturbing dreams
(it largely supports the null hypothesis of “not a causal factor” but does look at the many more likely alternative explanations, ranging from associated actually casual factors (such as alcohol and caffeine) and placebo/nocebo effect)
Finally, simple digestive issues may be the real thing at hand:
Worth noting that around two thirds of all people, including those who regularly enjoy dairy products, have some degree of lactose intolerance:
Lactose Intolerance in Adults: Biological Mechanism and Dietary Management
So, in terms of what cheese may be better/worse for you in this context, you might try experimenting with lactose-free cheese, which will help you identify whether that was the issue!
Share This Post
-

Fat’s Real Barriers To Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Fat Justice In Healthcare

This is Aubrey Gordon, an author, podcaster, and fat justice activist. What does that mean?
When it comes to healthcare, we previously covered some ideas very similar to her work, such as how…
There’s a lot of discrimination in healthcare settings
In this case, it often happens that a thin person goes in with a medical problem and gets treated for that, while a fat person can go in with the same medical problem and be told “you should try losing some weight”.
Top tip if this happens to you… Ask: “what would you advise/prescribe to a thin person with my same symptoms?”
Other things may be more systemic, for example:
When a thin person goes to get their blood pressure taken, and that goes smoothly, while a fat person goes to get their blood pressure taken, and there’s not a blood pressure cuff to fit them, is the problem the size of the person or the size of the cuff? It all depends on perspective, in a world built around thin people.
That’s a trivial-seeming example, but the same principle has far-reaching (and harmful) implications in healthcare in general, e.g:
- Surgeons being untrained (and/or unwilling) to operate on fat people
- Getting a one-size-fits-all dose that was calculated using average weight, and now doesn’t work
- MRI machines are famously claustrophobia-inducing for thin people; now try not fitting in it in the first place
…and so forth. So oftentimes, obesity will be correlated with a poor healthcare outcome, where the problem is not actually the obesity itself, but rather the system having been set up with thin people in mind.
It would be like saying “Having O- blood type results in higher risks when receiving blood transfusions”, while omitting to add “…because we didn’t stock O- blood”.
Read more on this topic: Shedding Some Obesity Myths
Does she have practical advice about this?
If she could have you understand one thing, it would be:
You deserve better.
Or if you are not fat: your fat friends deserve better.
How this becomes useful is: do not accept being treated as the problem!
Demand better!
If you meekly accept that you “just need to lose weight” and that thus you are the problem, you take away any responsibility from your healthcare provider(s) to actually do their jobs and provide healthcare.
See also Gordon’s book, which we’ve reviewed:
“You Just Need to Lose Weight”: And 19 Other Myths About Fat People – by Aubrey Gordon
Are you saying fat people don’t need to lose weight?
That’s a little like asking “would you say office workers don’t need to exercise more?”; there are implicit assumptions built into the question that are going unaddressed.
Rather: some people might benefit healthwise from losing weight, some might not.
In fact, over the age of 65, being what is nominally considered “overweight” reduces all-cause mortality risk.
For details of that and more, see: When BMI Doesn’t Measure Up
But what if I do want/need to lose weight?
Gordon’s not interested in helping with that, but we at 10almonds are, so…
Check out: Lose Weight, But Healthily
Where can I find more from Aubrey Gordon?
You might enjoy her blog:
Aubrey Gordon | Your Fat Friend
Or her other book:
What We Don’t Talk About When We Talk About Fat – by Aubrey Gordon
Enjoy!
Share This Post
-

Artichoke vs Bell Pepper – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing artichoke to bell pepper, we picked the artichoke.
Why?
First, you might remember that different color bell peppers have different nutritional profiles. So, you might be wondering why we didn’t specify the color. The reason is: the things that differ from one color to another are important differences between the respective bell peppers, but they make no difference to this comparison, as for any given nutrient that changes from one color to another, it doesn’t change the outcome.
Now, with that in mind, today’s comparison is pretty straightforward:
In terms of macros, artichoke has more than 3x the fiber for 2x the carbs, and nearly 4x the protein, making it the clear winner in this category.
In the category of vitamins, artichoke has more of vitamins B1, B2, B3, B5, B7, B9, K, and choline, while bell pepper has more of vitamins A, B6, C, and E. Another win for artichoke.
When it comes to minerals, artichoke has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while bell pepper is not higher in any minerals. One more win for artichoke.
In other news, artichoke has a lot more polyphenols; mostly flavones like apigenin and luteolin and phenolic acids like caffeoylquinic acid.
Adding up the sections makes for an overall win for artichokes, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
- 21 Most Beneficial Polyphenols & What Foods Have Them
- Which Bell Peppers To Pick? A Spectrum Of Specialties ← for the differences between the different colors
Enjoy!
Share This Post


-
A new treatment for Huntington’s disease is genuinely promising – but here’s why we still need caution
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Imagine knowing in your 20s or 30s that you carry a gene which will cause your mind and body to slowly unravel. Huntington’s disease is inherited, relentless and fatal, and there is no cure. Families live with the certainty of decline stretching across generations.
Now, a new treatment is being widely reported as a breakthrough.
Last week, gene therapy company uniQure announced that a one-time brain infusion appeared to slow the disease in a small clinical study.
If confirmed, this would not only be a landmark for Huntington’s disease but potentially the first time a gene therapy has shown promise in any adult-onset neurodegenerative disorder.
But the results, which were announced in a press release, are early, unreviewed and based on external comparisons. So, while these findings offer families hope after decades of failure, we need to remain cautious.

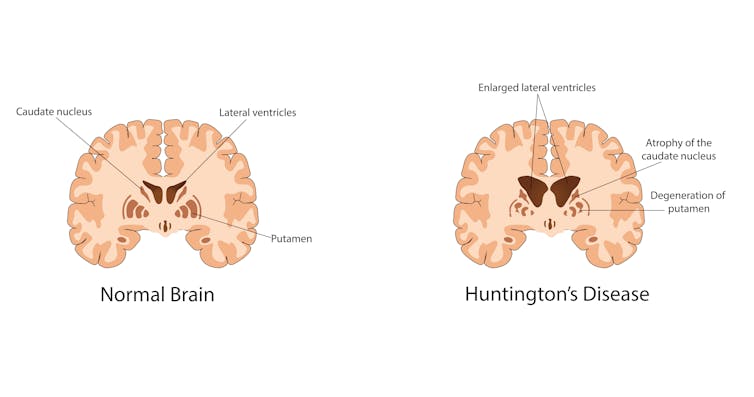
Krisada tepkulmanont/Getty What is Huntington’s disease?
Huntington’s is a rare but devastating disease, affecting around five to ten people in 100,000 in Western countries. That means thousands in Australia and hundreds of thousands worldwide.
Symptoms usually start in mid-life. They include involuntary movements, depression, irritability and progressive decline in thinking and memory. People lose the ability to work, manage money, live independently and eventually care for themselves. Most die ten to 20 years after onset.
The disease is caused by an expanded stretch of certain DNA repeats (CAG) in the huntingtin gene. The number of repeats strongly influences when symptoms begin, with longer expansions usually linked to earlier onset.
While rare, Huntington’s disease is inherited and fatal. Izuchukwu Onyeka/Getty Looking for a treatment
The gene that causes Huntington’s disease was identified in 1993, 32 years ago. Soon afterwards, mouse studies showed that switching off the mutant huntingtin protein even after symptoms had begun could reverse signs and improve behaviour.
This suggested lowering the toxic protein might slow or even partly reverse the disease. Yet for three decades, every attempt to develop a therapy for people has failed to show convincing clinical benefit. Trials of huntingtin-lowering drugs and other approaches did not slow progression.
What is the new treatment?
The one-time gene therapy, called AMT-130, involves brain surgery guided by MRI. Surgeons infuse an engineered virus directly into the caudate and putamen brain regions, which are heavily affected in Huntington’s.
The virus carries a short genetic “microRNA” designed to reduce production of the affected huntingtin protein.
By delivering it straight into the brain, the treatment bypasses the blood–brain barrier. This natural wall usually prevents medicines from entering the central nervous system. That barrier helps explain why so many brain-targeted drugs have failed.
What did they find?
Some 29 patients received treatment, with 12 in each group (one low-dose, and one high-dose) followed for three years. According to uniQure, those given the higher dose declined much slower than expected.
The study compared how much participants’ movement, thinking and daily function declined, compared to a matched external group from a global Huntington’s registry (meaning they weren’t part of the study). The company claimed those given the higher dose had a 75% slowing in their decline.
On a functional scale focused on independence, the company reported a 60% slowing in decline for the higher dose group.
Other tests of movement and thinking also favoured treatment. Nerve-cell damage in spinal fluid was lower for study participants than would be expected for untreated patients.
Why should we be cautious?
These findings are an early snapshot of results reported by the company, not yet peer-reviewed. The study compared treated patients to an external matched control group, not people randomised to placebo at the same time. This design can introduce bias. The numbers are also small – only 12 patients at the three-year mark – so we can’t draw solid conclusions.
The company reports the therapy was generally well tolerated, with no new serious adverse events related to the drug since late 2022. Most problems were related to the neurosurgical infusion itself, and resolved. But in a disease that already causes such severe symptoms, it is often hard to know what counts as a side effect.
The company uniQure has said it plans to seek regulatory approval in 2026 on the basis of this dataset.
Regulators will face difficult decisions: whether to allow access sooner before all the questions and uncertainties are addressed – based on the needs of a community with no effective options – and wait for further data while people are being treated, or to insist on larger trials that confirm results before approval.
What does it mean?
If upheld, these results represent the first convincing signs that a gene-targeted therapy can slow Huntington’s disease. They may also be the first evidence of benefit from a gene therapy in any adult-onset neurodegenerative disorder. That would be a milestone after decades of failure.
But these results do not prove success. Only larger, longer and fully peer-reviewed studies will show whether this treatment truly changes lives. Even if approved, a complex neurosurgical gene therapy may not be easily accessible to all patients.
The company has said the drug’s price would be similar to other gene therapies – which can cost over A$3 million per patient – and will have the added cost of brain surgery.
The takeaway
For families who carry this gene, the hope is profound. But caution is just as important.
We may be witnessing the first credible step toward slowing an inherited adult-onset neurodegenerative disease, or just an early signal that may not hold up.
Ultimately, only time and rigorous science will show whether this treatment delivers the benefits so urgently needed.
Bryce Vissel, Cojoint Professor, School of Clinical Medicine, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Cabbage vs Spinach – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cabbage to spinach, we picked the spinach.
Why?
Why, oh why indeed? ← lamentations of this cabbage-loving writer
But more seriously:
In terms of macros, these are very similar: mostly water, small amounts of carbs and protein, and enough fiber to hold them together. The only notable point of distinction here is that cabbage higher in soluble fiber, while spinach has more insoluble fiber, however these are both important, just different, and ultimately balanced in any case, so we’ll call this round a tie.
In the category of vitamins, cabbage has more of vitamins B5 and C, while spinach has more of vitamins A, B1, B2, B3, B6, B7, B9, E, K, and choline; a clear win for spinach.
When it comes to minerals, cabbage is not higher in any minerals, and spinach has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. Another easy win for spinach.
With regard to phytochemicals, spinach has a much higher polyphenol content (mostly flavonols), and on the flipside, spinach has a much higher oxalate content (that’s not a problem for most people, but bad if you have certain kidney issues). So this category could be swung any which way depending on the state of your kidneys. For simplicity, we’ll record this round as a tie, but its constituent parts are worth bearing in mind.
Adding up the sections makes for an overall win for spinach, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
What Do The Different Kinds Of Fiber Do? 30 Foods That Rank Highest
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Do therapies like EMDR affect memories of traumatic events?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
To recover from abuse or another traumatic experience, some people turn to a therapy called eye-movement desensitisation and reprocessing, or EMDR.
But this may present problems if these people pursue justice in the courts. In New South Wales, for instance, evidence obtained using EMDR can’t be used in a case unless it has been approved by the director (or deputy) of public prosecutions.
Prosecutors are concerned that after EMDR, trauma memories can’t be relied on as valid testimony. This has resulted in court cases not proceeding.
But what does the evidence say?
microgen/Getty Images What is EMDR?
EMDR is one of the common exposure-based treatments for post-traumatic stress disorder (PTSD).
This group of therapies – which encompass prolonged exposure, cognitive processing therapy, EMDR and other variants – all ask a patient to recall their trauma. The therapists integrates this information and aims to correct unhelpful thought patterns that may be prolonging their distress.
Each of these treatments is recommended in most international guidelines for treating PTSD.
EMDR is different from the other exposure-based therapies because the therapist also asks the patient to move their eyes in a rapid side-to-side movement. This will typically involve following the therapist’s fingers move back and forth.
Proponents of EMDR initially proposed eye movements triggered neural processes that help people better adjust to or process trauma memories. However, the actual role of eye movements has been subject to much debate.
Although the mechanism isn’t yet fully understood, the weight of evidence suggests eye movements may reduce distress while recounting trauma memories because it depletes our working memory capacity. This results in less focus on the negative emotions associated with the memory.
Where did concerns about EMDR affecting memories come from?
EMDR has been criticised for potentially distorting people’s memories of traumatic events dates since the 1990s when the treatment increased in popularity.
This was also a period when when a controversial movement of “recovered memory therapies” emerged. These were used to guide people to reconstruct memories that were purportedly “hidden” or “repressed”.
This involved therapists directing patients to focus attention on internal states, suspend reality and allow themselves to be guided by the therapist to recover so-called “repressed memories”, often of satanic or ritual abuse.
In the wake of this movement, many studies showed this sort of guided intervention could lead to false, or even implanted, memories.
At the same time, researchers were concerned about hypnotic techniques. During hypnosis, people could reconstruct false memories. They were particularly susceptible to misleading information and had stronger confidence in these memories.
For this reason, authorities around the world cautioned against using hypnosis in cases that may involve the person subsequently needing to give testimony in legal proceedings.
Some likened EMDR to hypnosis, others were sceptical of its claims
Some agencies and experts considered EMDR a hypnosis-like intervention because it focused the person’s attention on their internal state, promoted increased absorption in memories and actively guided memories.
Many also likened the finger waving in front of the patient’s face as inducing a hypnotic state.
Because EMDR guided patients to process memories in a way that made them less distressing, some concluded EMDR-elicited memories were comparably susceptible to distortion as hypnotically-induced memories.
This perception of EMDR at the time may also have been influenced by much initial scepticism of the therapy.
In the early period of its popularity, EMDR proponents made excessive claims of its success, such as being able to completely resolve trauma memories in a single session, despite the lack of evidence.
What does the evidence actually say?
It’s difficult to test the claim that EMDR increases the likelihood of false memories because you can’t readily study this in clinical settings.
Instead, researchers have used experimental designs in people without PTSD to determine if eye movements themselves are likely to lead to false memories. The results are mixed.
Multiple studies have shown eye movements can lead to false memories. One study showed healthy research participants a video of a car accident. Half the sample then used eye movements. Then all participants were read an eye-witness narrative that involved false information about the video.
This study found those who used eye movements were more susceptible to the misinformation. It seems this effect may occur because eye movements reduce the vividness and intensity of emotions in memories, thereby making them more susceptible to false memories.
However, other laboratory-based studies have not replicated this effect. One study using the same design found using eye movements didn’t make memory more likely, reduce correct memory details, or affect the vividness or emotional intensity of the memory.
What does this all mean?
EMDR is one of a suite of exposure-based treatments for PTSD that involve recounting trauma memories and integrating new information about the trauma. These appear to be key in helping people resolve their traumatic stress. Although EMDR is not better than other exposure-based treatment, it is as effective as the others.
Although some evidence points to eye movements making a person more susceptible to false memories, other studies do not find this. Importantly, these studies are not actually testing EMDR.
There is no direct evidence that EMDR leads to false memories, just as there is no evidence that prolonged exposure or other exposure-based treatments do. Singling EMDR out as being particularly susceptible to memory distortion doesn’t appear to be supported by the scientific evidence.
The position of legal authorities to not accept testimony following EMDR is therefore not justified and may deny trauma survivors the right to legal proceedings.
If this article has raised issues for you, or if you’re concerned about someone you know, call Lifeline on 13 11 14. The National Sexual Assault, Family and Domestic Violence Counselling Line – 1800 RESPECT (1800 737 732) – is also available 24/7 for any Australian who has experienced family violence or sexual assault.
Richard Bryant, Professor & Director of Traumatic Stress Clinic, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: