Maca Root’s Benefits For The Mood And The Ability
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Maca Root: What It Does And Doesn’t Do
Maca root, or Lepidium meyenii, gets thought of as a root vegetable, though it’s in fact a cruciferous vegetable and more closely related to cabbage—notwithstanding that it also gets called “Peruvian ginseng”.
- Nutritionally, it’s full of all manner of nutrients (vitamins, minerals, fiber, and a wide array of phytochemicals)
- Medicinally, it’s long enjoyed traditional use against a wide variety of illnesses, including respiratory infections and inflammatory diseases.
It’s also traditionally an aphrodisiac.
Is it really anti-inflammatory?
Probably not… Unless fermented. This hasn’t been studied deeply, but a 2023 study found that non-fermented and fermented maca root extracts had opposite effects in this regard:
However, this was an in vitro study, so we can’t say for sure that the results will carry over to humans.
Is it really an aphrodisiac?
Actually yes, it seems so. Here’s a study in which 45 women with antidepressant-induced sexual dysfunction found it significantly improved both libido and sexual function:
❝In summary, maca root may alleviate antidepressant-induced sexual dysfunction as women age, particularly in the domain of orgasm❞
~ Dr. Christina Dording et al.
Read in full: A Double-Blind Placebo-Controlled Trial of Maca Root as Treatment for Antidepressant-Induced Sexual Dysfunction in Women
As for men, well these mice (not technically men) found it beneficial too:
Effects of combined extracts of Lepidium meyenii and Allium tuberosum Rottl. on [e-word] dysfunction
(pardon the censorship; we’re trying to avoid people’s spam filters)
It did also improve fertility (and, actually in real men this time):
Does Lepidium meyenii (Maca) improve seminal quality?
Oh, to be in the mood
Here’s an interesting study in which 3g/day yielded significant mood improvement in these 175 (human) subjects:
And yes, it was found to be “well-tolerated” which is scientist-speak for “this appears to be completely safe, but we don’t want to commit ourselves to an absolutist statement and we can’t prove a negative”.
Oh, to have the energy
As it turns out, maca root does also offer benefits in this regard too:
(that’s not an added ingredient; it’s just a relevant chemical that the root naturally contains)
Want to try some?
We don’t sell it, but here for your convenience is an example product on Amazon 😎
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Ayurveda’s Contributions To Science

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Ayurveda’s Contributions To Science (Without Being Itself Rooted in Scientific Method)

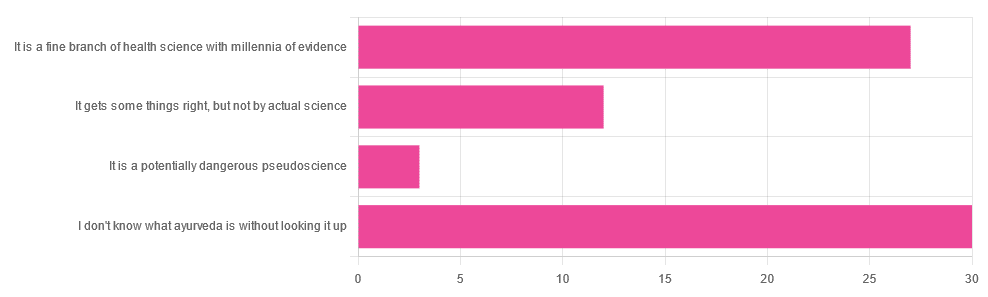
Yesterday, we asked you for your opinions on ayurveda, and got the above-depicted, below-described, set of responses. Of those who responded…
- A little over 41% said “I don’t know what ayurveda is without looking it up”
- A little over 37% said “It is a fine branch of health science with millennia of evidence”
- A little over 16% said “It gets some things right, but not by actual science”
- A little over 4% said “It is a potentially dangerous pseudoscience”
So, what does the science say?
Ayurveda is scientific: True or False?
False, simply. Let’s just rip the band-aid off in this case. That doesn’t mean it’s necessarily without merit, though!
Let’s put it this way:
- If you drink coffee to feel more awake because scientific method has discerned that caffeine has vasoconstrictive and adenosine-blocking effects while also promoting dopaminergic activity, then your consumption of coffee is evidence-based and scientific. Great!
- If you drink coffee to feel more awake because somebody told you that that somebody told them that it energizes you by balancing the elements fire (the heat of the coffee), air (the little bubbles on top), earth (the coffee grinds), water (the water), and ether (steam), then that is neither evidence-based nor scientific, but it will still work exactly the same.
Ayurveda is a little like that. It’s an ancient traditional Indian medicine, based on a combination of anecdotal evidence and supposition.
- The anecdotal evidence from ayurveda has often resulted in herbal remedies that, in modern scientific trials, have been found to have merit.
- Ayurvedic meditative practices also have a large overlap with modern mindfulness practices, and have also been found to have merit
- Ayurveda also promotes the practice of yoga, which is indeed a very healthful activity
- The supposition from ayurveda is based largely in those five elements we mentioned above, as well as a “balancing of humors” comparable to medieval European medicine, and from a scientific perspective, is simply a hypothesis with no evidence to support it.
Note: while ayurveda is commonly described as a science by its practitioners in the modern age, it did not originally claim to be scientific, but rather, wisdom handed down directly by the god Dhanvantari.
Ayurveda gets some things right: True or False?
True! Indeed, we covered some before in 10almonds; you may remember:
Bacopa Monnieri: A Well-Evidenced Cognitive Enhancer
(Bacopa monnieri is also known by its name in ayurveda, brahmi)
There are many other herbs that have made their way from ayurveda into modern science, but the above is a stand-out example. Others include:
- Ashwagandha: The Root of All Even-Mindedness?
- Boswellia serrata (Frankincense) Against Pain and Depression/Anxiety
Yoga and meditation are also great, and not only that, but great by science, for example:
- NCCIH | Yoga for Health: Clinical Guidelines, Scientific Literature, Info for Patients
- The Neuroscience of Mindfulness: How Mindfulness Alters the Brain and Facilitates Emotion Regulation
Ayurveda is a potentially dangerous pseudoscience: True or False?
Also True! We covered why it’s a pseudoscience above, but that doesn’t make it potentially dangerous, per se (you’ll remember our coffee example).
What does, however, make it potentially dangerous (dose-dependent) is its use of heavy metals such as lead, mercury, and arsenic:
Heavy Metal Content of Ayurvedic Herbal Medicine Products
Some final thoughts…
Want to learn more about the sometimes beneficial, sometimes uneasy relationship between ayurveda and modern science?
A lot of scholarly articles trying to bridge (or further separate) the two were very biased one way or the other.
Instead, here’s one that’s reasonably optimistic with regard to ayurveda’s potential for good, while being realistic about how it currently stands:
Development of Ayurveda—Tradition to trend
Take care!
Share This Post
-

Heart Healthy Diet Plan – by Stephen William
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve covered heart-healthy cooking books before, but variety is good, and boredom is an enemy of health, so let’s shake it up with a fresh stack of recipes!
After a brief overview of the relevant science (which if you’re a regular 10almonds reader, probably won’t be new to you), the author takes the reader on a 28-day journey. Yes, we know the subtitle says 30 days, but unless they carefully hid the other two days somewhere we didn’t find, there are “only” 28 inside. Perhaps the publisher heard it was a month and took creative license. Or maybe there’s a different edition. Either way…
Rather than merely giving a diet plan (though yes, he also does that), he gives a wide range of “spotlight ingredients”, such that many of the recipes, while great in and of themselves, can also be jumping-off points for those of us who like to take recipes and immediately do our own things to them.
Each day gets a breakfast, lunch, dinner, and he also covers drinks, desserts, and such like.
Notwithstanding the cover art being a lot of plants, the recipes are not entirely plant-based; there are a selection of fish dishes (and other seafood, e.g. shrimp) and also some dairy products (e.g. Greek yoghurt). The recipes are certainly very “plant-forward” though and many are just plants. If you’re a strict vegan though, this probably isn’t the book for you.
Bottom line: if you’d like to cook heart-healthy but are often stuck wondering “aaah, what to cook again today?”, then this is the book to get you out of any culinary creative block!
Click here to check out the Heart Healthy Diet Plan, and widen your heart-healthy repertoire!
Share This Post
-

Anti-Inflammatory Diet 101 (What to Eat to Fight Inflammation)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Chronic inflammation is a cause and/or exacerbating factor in very many diseases. Arthritis, diabetes, and heart disease are probably top of the list, but there are lots more where they came from. And, it’s good to avoid those things. So, how to eat to avoid inflammation?
Let food be thy medicine
The key things to keep in mind, the “guiding principles” are to prioritize whole, minimally-processed foods, and enjoy foods with plenty of antioxidants. Getting a healthy balance of omega fatty acids is also important, which for most people means getting more omega-3 and less omega-6.
Shopping list (foods to prioritize) includes:
- fruits and vegetables in a variety of colors (e.g. berries, leafy greens, beats)
- whole grains, going for the most fiber-rich options (e.g. quinoa, brown rice, oats)
- healthy fats (e.g. avocados, nuts, seeds)
- fatty fish (e.g. salmon, mackerel, sardines) ← don’t worry about this if you’re vegetarian/vegan though, as the previous category can already cover it
- herbs and spices (e.g. turmeric, garlic, ginger)
Noping list (foods to avoid) includes:
- refined carbohydrates
- highly processed and/or fried foods
- red meats and/or processed meats (yes, that does mean that organic grass-fed farmers’ pinky-promise-certified holistically-raised beef is also off the menu)
- dairy products, especially if unfermented
For more information on each of these, plus advice on transitioning away from an inflammatory diet, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
How to Prevent (or Reduce) Inflammation
Take care!
Share This Post

Related Posts
-

Long COVID is real—here’s how patients can get treatment and support
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What you need to know
- There is still no single, FDA-approved treatment for long COVID, but doctors can help patients manage individual symptoms.
- Long COVID patients may be eligible for government benefits that can ease financial burdens.
- Getting reinfected with COVID-19 can worsen existing long COVID symptoms, but patients can take steps to stay protected.
On March 15—Long COVID Awareness Day—patients shared their stories and demanded more funding for long COVID research. Nearly one in five U.S. adults who contract COVID-19 suffer from long COVID, and up to 5.8 million children have the disease.
Anyone who contracts COVID-19 is at risk of developing long-term illness. Long COVID has been deemed by some a “mass-disabling event,” as its symptoms can significantly disrupt patients’ lives.
Fortunately, there’s hope. New treatment options are in development, and there are resources available that may ease the physical, mental, and financial burdens that long COVID patients face.
Read on to learn more about resources for long COVID patients and how you can support the long COVID patients in your life.
What is long COVID, and who is at risk?
Long COVID is a cluster of symptoms that can occur after a COVID-19 infection and last for weeks, months, or years, potentially affecting almost every organ. Symptoms range from mild to debilitating and may include fatigue, chest pain, brain fog, dizziness, abdominal pain, joint pain, and changes in taste or smell.
Anyone who gets infected with COVID-19 is at risk of developing long COVID, but some groups are at greater risk, including unvaccinated people, women, people over 40, and people who face health inequities.
What types of support are available for long COVID patients?
Currently, there is still no single, FDA-approved treatment for long COVID, but doctors can help patients manage individual symptoms. Some options for long COVID treatment include therapies to improve lung function and retrain your sense of smell, as well as medications for pain and blood pressure regulation. Staying up to date on COVID-19 vaccines may also improve symptoms and reduce inflammation.
Long COVID patients are eligible for disability benefits under the Americans with Disabilities Act. The Pandemic Legal Assistance Network provides pro bono support for long COVID patients applying for these benefits.
Long COVID patients may also be eligible for other forms of government assistance, such as Supplemental Nutrition Assistance Program (SNAP), Temporary Assistance for Needy Families (TANF), Medicaid, and rental and utility assistance programs.
How can friends and family of long COVID patients provide support?
Getting reinfected with COVID-19 can worsen existing long COVID symptoms. Wearing a high-quality, well-fitting mask will reduce your risk of contracting COVID-19 and spreading it to long COVID patients and others. At indoor gatherings, improving ventilation by opening doors and windows, using high-efficiency particulate air (HEPA) filters, and building your own Corsi-Rosenthal box can also reduce the spread of the COVID-19 virus.
Long COVID patients may also benefit from emotional and financial support as they manage symptoms, navigate barriers to treatment, and go through the months-long process of applying for and receiving disability benefits.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.

Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Power Foods Diet – by Dr. Neal Barnard
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what this is not: it’s not a cookbook. There are recipes, more than a hundred if we consider such things as “barbecue sauce” as a standalone recipe, and if we overlook such things as how “perfect hot oatmeal” is followed on the next page by a recipe for “perfect hot oatmeal with berries”.
However, as we say, it’s not a cookbook; it’s first and foremost an educational text on the topic of nutrition.
Here we will learn about good eating for general health, which foods are natural appetite-suppressants, which foods reduce our body’s absorption of sugars from foods (not merely slowing, but flushing them away so they cannot be absorbed at all), and which foods actually boost metabolism for a few hours after the meal.
Dr. Barnard also talks about some foods that are more healthy, or less healthy, than popularly believed, and how to use all this information to craft a good, optimized, dietary plan for you.
Bottom line: there’s a lot of good information here, and the recipes are simply a bonus.
Click here to check out The Power Foods Diet, and optimize yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Glucose Goddess Method – by Jessie Inchausspé
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve previously reviewed Inchausspé’s excellent book “Glucose Revolution”. So what does this book add?
This book is for those who found that book a little dense. While this one still gives the same ten “hacks”, she focuses on the four that have the biggest effect, and walks the reader by the hand through a four-week programme of implementing them.
The claim of 100+ recipes is a little bold, as some of the recipes are things like vinegar, vinegar+water, vinegar+water but now we’re it’s in a restaurant, lemon+water, lemon+water but now it’s in a bottle, etc. However, there are legitimately a lot of actual recipes too.
Where this book’s greatest strength lies is in making everything super easy, and motivating. It’s a fine choice for being up-and-running quickly and easily without wading through the 300-odd pages of science in her previous book.
Bottom line: if you’ve already happily and sustainably implemented everything from her previous book, you can probably skip this one. However, if you’d like an easier method to implement the changes that have the biggest effect, then this is the book for you.
Click here to check out The Glucose Goddess Method, and build it into your life the easy way!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: