The Easiest Way To Take Up Journaling
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dear Diary…
It’s well-established that journaling is generally good for mental health. It’s not a magical panacea, as evidenced by The Diaries of Franz Kafka for example (that man was not in good mental health). But for most of us, putting our thoughts and feelings down on paper (or the digital equivalent) is a good step for tidying our mind.
And as it can be said: mental health is also just health.
But…
What to write about?
It’s about self-expression (even if only you will read it), and…
❝Writing about traumatic, stressful or emotional events has been found to result in improvements in both physical and psychological health, in non-clinical and clinical populations.
In the expressive writing paradigm, participants are asked to write about such events for 15–20 minutes on 3–5 occasions.
Those who do so generally have significantly better physical and psychological outcomes compared with those who write about neutral topics.❞
Source: Emotional and physical health benefits of expressive writing
In other words, write about whatever moves you.
Working from prompts
If you read the advice above and thought “but I don’t know what moves me”, then fear not. It’s perfectly respectable to work from prompts, such as:
- What last made you cry?
- What last made you laugh?
- What was a recent meaningful moment with family?
- What is a serious mistake that you made and learned from?
- If you could be remembered for just one thing, what would you want it to be?
In fact, sometimes working from prompts has extra benefits, precisely because it challenges us to examine things we might not otherwise think about.
If a prompt asks “What tends to bring you most joy recently?” and the question stumps you, then a) you now are prompted to look at what you can change to find more joy b) you probably wouldn’t have thought of this question—most depressed people don’t, and if you cannot remember recent joy, then well, we’re not here to diagnose, but let’s just say that’s a symptom.
A quick aside: if you or a loved oneare prone to depressive episodes, here’s a good resource, by the way:
The Mental Health First-Aid That You’ll Hopefully Never Need
And in the event of the mental health worst case scenario:
The six prompts we gave earlier are just ideas that came to this writer’s mind, but they’re (ok, some bias here) very good ones. If you’d like more though, here’s a good resource:
550+ Journal Prompts: The Ultimate List
The Good, The Bad, and The Ugly
While it’s not good to get stuck in ruminative negative thought spirals, it is good to have a safe outlet to express one’s negative thoughts/feelings:
Remember, your journal is (or ideally, should be) a place without censure. If you fear social consequences should your journal be read, then using an app with a good security policy and encryption options can be a good idea for journaling
Finch App is a good free option if it’s not too cutesy for your taste, because in terms of security:
- It can’t leak your data because your data never leaves your phone (unless you manually back up your data and then you choose to put it somewhere unsafe)
- It has an option to require passcode/biometrics etc to open the app
As a bonus, it also has very many optional journaling prompts, and also (optional) behavioral activation prompts, amongst more other offerings that we don’t have room to list here.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Top Micronutrient Deficiency In High Blood Pressure

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
High blood pressure is often considered a matter of too much sodium, but there’s another micronutrient that’s critical, and a lot of people have too little of it:
The Other Special K
Potassium helps regulate blood pressure by doing the opposite of what sodium does: high sodium intake increases blood volume and pressure by retaining fluid, while potassium promotes sodium excretion through urine, reducing fluid retention and lowering blood pressure.
Clinical studies (which you can find beneath the video, if you click through to YouTube) have shown that increasing potassium intake can reduce systolic blood pressure by an average of 3.49 units, with even greater reductions (up to 7 units) at higher potassium intakes of 3,500–4,700 mg/day.
Potassium-rich foods include most fruit*, leafy greens, broccoli, lentils, and beans.
*because of some popular mentions in TV shows, people get hung up on bananas being a good source of potassium. Which they are, but they’re not even in the top 10 of fruits for potassium. Here’s a non-exhaustive list of fruits that have more potassium than bananas, portion for portion:
- Honeydew melon
- Papaya
- Mango
- Prunes
- Figs
- Dates
- Nectarine
- Cantaloupe melon
- Kiwi
- Orange
These foods also provide fiber, which aids in weight management and further lowers risks for cardiovascular disease. Increasing fiber intake by just 14g a day has been shown not only to reduce calorie consumption and promote weight loss, but also (more importantly) lower blood pressure, cholesterol, and overall health risks.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
What Matters Most For Your Heart? Eat More (Of This) For Lower Blood Pressure ← this is about fiber; while potassium is the most common micronutrient deficiency in people with high blood pressure, fiber is the most common macronutrient deficiency, and arguably the most critical in this regard.
Take care!
Share This Post
-
Traveling To Die: The Latest Form of Medical Tourism
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In the 18 months after Francine Milano was diagnosed with a recurrence of the ovarian cancer she thought she’d beaten 20 years ago, she traveled twice from her home in Pennsylvania to Vermont. She went not to ski, hike, or leaf-peep, but to arrange to die.
“I really wanted to take control over how I left this world,” said the 61-year-old who lives in Lancaster. “I decided that this was an option for me.”
Dying with medical assistance wasn’t an option when Milano learned in early 2023 that her disease was incurable. At that point, she would have had to travel to Switzerland — or live in the District of Columbia or one of the 10 states where medical aid in dying was legal.
But Vermont lifted its residency requirement in May 2023, followed by Oregon two months later. (Montana effectively allows aid in dying through a 2009 court decision, but that ruling doesn’t spell out rules around residency. And though New York and California recently considered legislation that would allow out-of-staters to secure aid in dying, neither provision passed.)
Despite the limited options and the challenges — such as finding doctors in a new state, figuring out where to die, and traveling when too sick to walk to the next room, let alone climb into a car — dozens have made the trek to the two states that have opened their doors to terminally ill nonresidents seeking aid in dying.
At least 26 people have traveled to Vermont to die, representing nearly 25% of the reported assisted deaths in the state from May 2023 through this June, according to the Vermont Department of Health. In Oregon, 23 out-of-state residents died using medical assistance in 2023, just over 6% of the state total, according to the Oregon Health Authority.
Oncologist Charles Blanke, whose clinic in Portland is devoted to end-of-life care, said he thinks that Oregon’s total is likely an undercount and he expects the numbers to grow. Over the past year, he said, he’s seen two to four out-of-state patients a week — about one-quarter of his practice — and fielded calls from across the U.S., including New York, the Carolinas, Florida, and “tons from Texas.” But just because patients are willing to travel doesn’t mean it’s easy or that they get their desired outcome.
“The law is pretty strict about what has to be done,” Blanke said.
As in other states that allow what some call physician-assisted death or assisted suicide, Oregon and Vermont require patients to be assessed by two doctors. Patients must have less than six months to live, be mentally and cognitively sound, and be physically able to ingest the drugs to end their lives. Charts and records must be reviewed in the state; neglecting to do so constitutes practicing medicine out of state, which violates medical licensing requirements. For the same reason, the patients must be in the state for the initial exam, when they request the drugs, and when they ingest them.
State legislatures impose those restrictions as safeguards — to balance the rights of patients seeking aid in dying with a legislative imperative not to pass laws that are harmful to anyone, said Peg Sandeen, CEO of the group Death With Dignity. Like many aid-in-dying advocates, however, she said such rules create undue burdens for people who are already suffering.
Diana Barnard, a Vermont palliative care physician, said some patients cannot even come for their appointments. “They end up being sick or not feeling like traveling, so there’s rescheduling involved,” she said. “It’s asking people to use a significant part of their energy to come here when they really deserve to have the option closer to home.”
Those opposed to aid in dying include religious groups that say taking a life is immoral, and medical practitioners who argue their job is to make people more comfortable at the end of life, not to end the life itself.
Anthropologist Anita Hannig, who interviewed dozens of terminally ill patients while researching her 2022 book, “The Day I Die: The Untold Story of Assisted Dying in America,” said she doesn’t expect federal legislation to settle the issue anytime soon. As the Supreme Court did with abortion in 2022, it ruled assisted dying to be a states’ rights issue in 1997.
During the 2023-24 legislative sessions, 19 states (including Milano’s home state of Pennsylvania) considered aid-in-dying legislation, according to the advocacy group Compassion & Choices. Delaware was the sole state to pass it, but the governor has yet to act on it.
Sandeen said that many states initially pass restrictive laws — requiring 21-day wait times and psychiatric evaluations, for instance — only to eventually repeal provisions that prove unduly onerous. That makes her optimistic that more states will eventually follow Vermont and Oregon, she said.
Milano would have preferred to travel to neighboring New Jersey, where aid in dying has been legal since 2019, but its residency requirement made that a nonstarter. And though Oregon has more providers than the largely rural state of Vermont, Milano opted for the nine-hour car ride to Burlington because it was less physically and financially draining than a cross-country trip.
The logistics were key because Milano knew she’d have to return. When she traveled to Vermont in May 2023 with her husband and her brother, she wasn’t near death. She figured that the next time she was in Vermont, it would be to request the medication. Then she’d have to wait 15 days to receive it.
The waiting period is standard to ensure that a person has what Barnard calls “thoughtful time to contemplate the decision,” although she said most have done that long before. Some states have shortened the period or, like Oregon, have a waiver option.
That waiting period can be hard on patients, on top of being away from their health care team, home, and family. Blanke said he has seen as many as 25 relatives attend the death of an Oregon resident, but out-of-staters usually bring only one person. And while finding a place to die can be a problem for Oregonians who are in care homes or hospitals that prohibit aid in dying, it’s especially challenging for nonresidents.
When Oregon lifted its residency requirement, Blanke advertised on Craigslist and used the results to compile a list of short-term accommodations, including Airbnbs, willing to allow patients to die there. Nonprofits in states with aid-in-dying laws also maintain such lists, Sandeen said.
Milano hasn’t gotten to the point where she needs to find a place to take the meds and end her life. In fact, because she had a relatively healthy year after her first trip to Vermont, she let her six-month approval period lapse.
In June, though, she headed back to open another six-month window. This time, she went with a girlfriend who has a camper van. They drove six hours to cross the state border, stopping at a playground and gift shop before sitting in a parking lot where Milano had a Zoom appointment with her doctors rather than driving three more hours to Burlington to meet in person.
“I don’t know if they do GPS tracking or IP address kind of stuff, but I would have been afraid not to be honest,” she said.
That’s not all that scares her. She worries she’ll be too sick to return to Vermont when she is ready to die. And, even if she can get there, she wonders whether she’ll have the courage to take the medication. About one-third of people approved for assisted death don’t follow through, Blanke said. For them, it’s often enough to know they have the meds — the control — to end their lives when they want.
Milano said she is grateful she has that power now while she’s still healthy enough to travel and enjoy life. “I just wish more people had the option,” she said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-

The End of Heart Disease – by Dr. Joel Fuhrman
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve previously reviewed another of Dr. Fuhrman’s books, “Eat To Live”, and this time, he’s focusing specifically on preventing/reversing heart disease.
Dr. Fuhrman takes the stance that our food can either kill or heal us, and we get to choose which. As such, nutrition is central to his heart-healthy plan; he mostly leaves matters of exercise, sleep, etc to other sources.
His dietary approach is mostly uncontroversial: for example, advices include: enjoy nutritionally dense foods, skip processed foods, eat at least mostly plants, skip the added salt. A slightly more controversial aspect is that he advocates for avoiding cooking oils, including the healthiest oils, including olive and avocado, which are by current scientific consensus considered heart-healthy in moderation. As in, not even just heart-neutral, but rather, they actively improve triglycerides.
He compares different cardioprotective diets, and while he’s not unbiased, he does provide 40 pages of scholarly references, so we may understand that at the very least, his approach is sound.
There are also recipes—94 pages of them—for any who might wonder “how do I cook without…?” and some ingredient he would rather you omit.
The style is information-dense (and this is a 448-page book) but still very readable.
Bottom line: if you’re serious about improving your heart health, this book can help a lot with that.
Click here to check out The End Of Heart Disease, and end heart disease for yourself!
Share This Post


Related Posts
-

100 Ways to Change Your Life – by Liz Moody
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sometimes we crave changing things up, just to feel something new. This can result in anything from bad haircut decisions or impulsive purchases, to crashing and burning-out of a job, project, or relationship. It doesn’t have to be that way, though!
This book brings us (as the title suggest) 100 evidence-based ways of changing things up in a good way—small things that can make a big difference in many areas of life.
In terms of format, these are presented in 100 tiny chapters, each approximately 2 pages long (obviously it depends on the edition, but you get the idea). Great to read in any of at least three ways:
- Cover-to-cover
- One per day for 100 days
- Look up what you need on an ad hoc basis
Bottom line: even if you already do half of these things, the other half will each compound your health happiness one-by-one as you add them. This is a very enjoyable and practical book!
Click here to check out 100 Ways to Change Your Life, and level-up yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The Joy Of Missing Out
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What this is not going to be: a sour grapes thing.
What this is going to be: an exploration of how the grass is greener
on the other side of the fencewherever you water itIt’s easy to feel lonely and isolated, even in today’s increasingly-connected world. We’ve tackled that topic before:
How To Beat Loneliness & Isolation
One of the more passive (but still reasonable) ways of reducing isolation is to simply say “yes” more, which we discussed (along with other more active strategies) here:
When The World Moves Without Us… Can We Side-Step Age-Related Alienation?
But, is there any benefit to be gained from not being in the thick of things?
Sometimes some things associated with isolation are not, in reality, necessarily isolating. See for example:
But, the implications of embracing the “joy of missing out” are much more wide-reaching:
Wherever you are, there you are
You’ve probably read before the phrase “wherever you go, there you are”, but this phrasing brings attention to the fact that you already are where you are.
There are quite possibly aspects of your current life/situation that are not ideal, but take a moment to appreciate where you are in life. At the very least, you are probably in a safe warm dry house with plenty of food available; chances are you have plenty of luxuries too.
See also: How To Get Your Brain On A More Positive Track (Without Toxic Positivity)
And yet, it’s easy to have a fear of missing out. Even billionaires fear they do not have enough and must acquire more in order to be truly secure and fulfilled.
As it goes for material wealth, so it also goes for social wealth—in other words, we may worry about such questions as: on whom can we rely, and who will be there for us if we need them? Do we, ultimately, have enough social capital to be secure?
- For social media influencers, it’ll be follower counts and engagement.
- For the family-oriented, it might be the question of whose house a given holiday gets celebrated at, and who attends, and who does it best.
- In more somber matters, think about funerals, and those where “there was such a huge turnout” vs “almost nobody attended”.
It sure sounds a lot like a dog-eat-dog world in which missing out sucks! But it doesn’t have to.
So let’s recap: your current situation is probably, all things considered, not bad. There is probably much in life to enjoy. If people do not come to your holiday event, then those are not people who would have improved things for you. If people do not attend your funeral even, then well, you yourself will be late, so hey.
Right now though, you are alive, so…
Enjoy the moment; enjoy your life for you.
Invest in yourself. Better yourself. Improve your environment for yourself little by little.
We spend a lot of time in life living up to everyone’s expectations, often without stopping to question whether it is what we want, or sometimes putting aside what we want in favor of what is wanted of us.
- Sometimes, such ostensible altruism is laudable and good (the point of today’s article is not “be a selfish jerk”; sometimes we should indeed shelve our self-interest in favour of doing something for the common good)
- Sometimes, it’s just pointless sacrifice that benefits nobody (the point of today’s article is “there is no point in playing stressful, stacked games when you could have a better time not doing that”)
If you are about to embark on an endeavor that you don’t really want to, take a moment to seriously consider which of the above two situations this is, and then act accordingly.
For a deeper dive into that, you might like this book that we reviewed a while back:
The Joy of Saying No – by Natalie Lue
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Antidepressants: Personalization Is Key!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Antidepressants: Personalization Is Key!

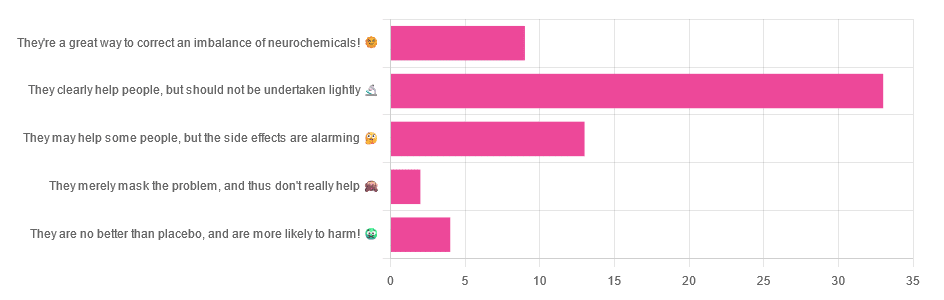
Yesterday, we asked you for your opinions on antidepressants, and got the above-depicted, below-described, set of responses:
- Just over half of respondents said “They clearly help people, but should not be undertaken lightly”
- Just over a fifth of respondents said “They may help some people, but the side effects are alarming”
- Just under a sixth of respondents said “They’re a great way to correct an imbalance of neurochemicals”
- Four respondents said “They are no better than placebo, and are more likely to harm”
- Two respondents said “They merely mask the problem, and thus don’t really help”
So what does the science say?
❝They are no better than placebo, and are more likely to harm? True or False?❞
True or False depending on who you are and what you’re taking. Different antidepressants can work on many different systems with different mechanisms of action. This means if and only if you’re not taking the “right” antidepressant for you, then yes, you will get only placebo benefits:
- Placebo Effect in the Treatment of Depression and Anxiety ← randomly assigned antidepressants are, shockingly, luck of the draw in usefulness
- Antidepressants versus placebo in major depression: an overview ← “wow this science is messy”
- Comparative efficacy and acceptability of 21 antidepressant drugs: a systematic review and network meta-analysis ← “oh look, it makes a difference which antidepressant we give to people”
Rather than dismissing antidepressants as worthless, therefore, it is a good idea to find out (by examination or trial and error) what kind of antidepressant you need, if you indeed do need such.
Otherwise it is like getting a flu shot and being surprised when you still catch a cold!
❝They merely mask the problem, and thus don’t really help: True or False?❞
False, categorically.
The problem in depressed people is the depressed mood. This may be influenced by other factors, and antidepressants indeed won’t help directly with those, but they can enable the person to better tackle them (more on this later).
❝They may help some people, but the side-effects are alarming: True or False?❞
True or False depending on more factors than we can cover here.
Side-effects vary from drug to drug and person to person, of course. As does tolerability and acceptability, since to some extent these things are subjective.
One person’s dealbreaker may be another person’s shrugworthy minor inconvenience at most.
❝They’re a great way to correct an imbalance of neurochemicals: True or False?❞
True! Contingently.
That is to say: they’re a great way to correct an imbalance of neurochemicals if and only if your problem is (at least partly) an imbalance of neurochemicals. If it’s not, then your brain can have all the neurotransmitters it needs, and you will still be depressed, because (for example) the other factors* influencing your depression have not changed.
*common examples include low self-esteem, poor physical health, socioeconomic adversity, and ostensibly bleak prospects for the future.
For those for whom the problem is/was partly a neurochemical imbalance and partly other factors, the greatest help the antidepressants give is getting the brain into sufficient working order to be able to tackle those other factors.
Want to know more about the different kinds?
Here’s a helpful side-by-side comparison of common antidepressants, what type they are, and other considerations:
Mind | Comparing Antidepressants
Want a drug-free approach?
You might like our previous main feature:
The Mental Health First-Aid That You’ll Hopefully Never Need
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: