How we can prepare for future public health emergencies
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
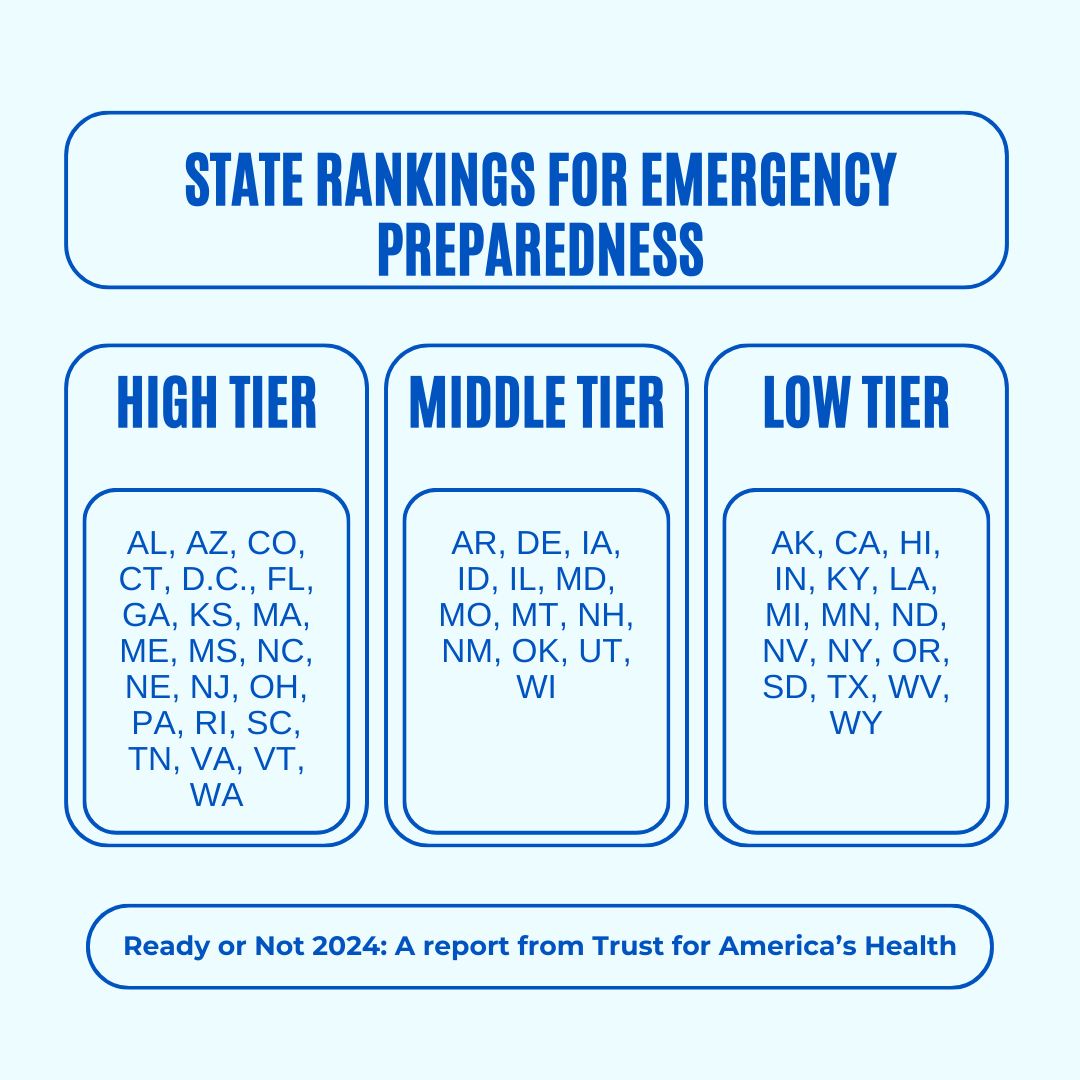
The U.S. is experiencing an increasing number of disease outbreaks and extreme weather events. While state and national preparedness for public health emergencies has improved in some areas, dangerous gaps remain, says a recent report from Trust for America’s Health.
Titled, “Ready or Not 2024: Protecting the Public’s Health from Diseases, Disasters, and Bioterrorism,” the report identifies gaps in national and state preparedness for public health emergencies and provides recommendations for improvement.
Using nine key indicators, the report categorizes all U.S. states and the District of Columbia into three readiness levels: high, medium, and low. The writers hope the report will help policymakers in under-performing states improve public health infrastructure.
Read on to learn more about what the research found and how we can individually prepare for future public health emergencies.
There’s work to be done
The report highlights areas with strong performance as well as those that need improvement.
Some areas with strong performance:
- State public health funding: Most states and the District of Columbia either maintained or increased their public health funding during the 2023 fiscal year.
- Health care labor force preparedness: Most states have started expanding the health care labor force for improved emergency response. As of 2023, 39 states participated in the Nurse Licensure Compact, which allows nurses to work in multiple member states without the need for additional state licenses.
Some areas that need improvement:
- Hospital safety scores: Only 25 percent of acute care hospitals earned the highest patient safety grade in fall 2023. These scores measure health care-associated infection rates, intensive care unit capacity, and other metrics. More high-scoring hospitals would improve preparedness for future public health emergencies.
- Access to paid time off: From March 2018 to March 2023, only 55 percent of U.S. workers used paid time off. Access to paid time off is important for reducing the spread of infectious diseases.
We can all do our part by staying up to date on vaccines
While the report focuses on policy changes that would improve emergency preparedness, Trust for America’s Health’s research identifies one way that we can individually prepare for future public health emergencies: staying up to date on vaccines.
The report found that during the 2022-2023 flu season, only 49 percent of those eligible for the flu vaccine received it. Public health experts are concerned that false claims about COVID-19 vaccines have resulted in overall vaccine hesitancy.
A decline in vaccination rates has led to an uptick in life-threatening, vaccine-preventable diseases, such as measles. Increasing vaccine uptake would prevent the spread of vaccine-preventable diseases and reduce strain on hospital systems during public health crises.
Make sure that you and your children have received all recommended vaccines to prevent severe illness, hospitalization, and death. Learn more about recommended vaccines for adults and children from the CDC.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.

Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Heal Your Stressed Brain

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Rochelle Walsh, therapist, explains the problem and how to fix it:
Not all brain damage is from the outside
Long-term stress and burnout cause brain damage; it’s not just a mindset issue—it impacts the brain physiologically. To compound matters, it also increases the risk of neurodegenerative diseases. While the brain can indeed grow new neurons and regenerate itself, chronic stress damages specific regions, and inhibits that.
There are some effects of chronic stress that can seem positive—the amygdalae and hypothalamus are seen to grow larger and stronger, for instance—but this is, unfortunately, “all the better to stress you with”. In compensation for this, chronic stress deprioritizes the pre-frontal cortex and hippocampi, so there goes your reasoning and memory.
This often results in people not managing chronic stress well. Just like a weak heart and lungs might impede the exercise that could make them stronger, the stressed brain is not good at permitting you to do the things that would heal it—preferring to keep you on edge all day, worrying and twitchy, mind racing and body tense. It also tends to lead to autoimmune diseases, due to the increased inflammation (because the body’s threat-detection system as at “jumping at own shadow” levels so it’s deploying every defense it has, including completely inappropriate ones).
Notwithstanding the “Heal Your Stressed Brain” thumbnail, she doesn’t actually go into this in detail and bids us sign up for her masterclass. We at 10almonds however like to deliver, so you can find useful advice and free resources in our links-drop at the bottom of this article.
Meanwhile, if you’d like to hear more about the neurological woes described above, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Meditation That You’ll Actually Enjoy
- How To Manage/Reduce Chronic Stress
- Lower Your Cortisol! (Here’s Why & How)
- How Healthy People Regulate Their Emotions
- Sleep: Yes, You Really Do Still Need It!
- Give Your Adrenal Glands A Chance
- The Stress Prescription (Against Aging!)
Take care!
Share This Post
-
Mung Beans vs Red Lentils – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing mung beans to red lentils, we picked the lentils.
Why?
Both are great! But the lentils win on overall nutritional density.
In terms of macros, they have approximately the same carbs and fiber, and are both low glycemic index foods. The deciding factor is that the lentils have slightly more protein—but it’s not a huge difference; both are very good sources of protein.
In the category of vitamins, mung beans have more of vitamins A, E, and K, while red lentils have more of vitamins B1, B2, B3, B5, B6, B9, C, and choline. An easy win for lentils.
When it comes to minerals, again both are great, but mung beans have more calcium and magnesium (hence the green color) while red lentils have more copper, iron, manganese, phosphorus, potassium, selenium, and zinc. Another clear win for lentils.
Polyphenols are also a worthy category to note here; both have plenty, but red lentils have more, especially flavonols, anthocyanidins, proanthocyanidins, and anthocyanins (whence the red color).
In short: enjoy both, because diversity is almost always best. But if you’re picking one, red lentils are the most nutritious of the two.
Want to learn more?
You might like to read:
Sprout Your Seeds, Grains, Beans, Etc
Take care!
Share This Post
-

How Ibogaine Can Beat Buprenorphine For Beating Addictions
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Questions?❞
It seems that this week, everyone was so satisfied with our information, that we received no questions! (If you sent one and we somehow missed it, please accept our apologies and do bring our attention to it)
However, we did receive some expert feedback that we wanted to share because it’s so informative:
❝I work at a detox rehab in Mexico, where we can use methods not legal in the United States. Therefore, while much of the linked articles had useful information, I’m in the “trenches” every day, and there’s some information I’d like to share that you may wish to share, with additional information:
- Buprenorphine is widely used and ineffective for addiction because it’s synthetic and has many adverse side effects. For heavy drug users it isn’t enough and they still hit the streets for more opioid, resulting in fentanyl deaths. Depending on length of usage and dose, it can take WEEKS to get off of, and it’s extremely difficult.
- Ibogaine is the medicine we use to detox people off opiates, alcohol, meth as well as my own specialty, bulimia. It’s psychoactive and it temporarily “resets” the brain to a pre-addictive state. Supplemented by behavior and lifestyle changes, as well as addressing the traumas that led to the addiction is extremely effective.
Our results are about 50%, meaning the client is free of the substance or behavior 1 year later. Ibogaine isn’t a “magic pill” or cure, it’s an opening tool that makes the difficult work of reclaiming one’s life easier.
Ibogaine is not something that should be done outside a medical setting. It requires an EKG to ensure the heart is healthy and doesn’t have prolonged QT intervals; also blood testing to ensure organs are functioning (especially the liver) and mineral levels such as magnetic and potassium are where they should be. It is important that this treatment be conducted by experienced doctors or practitioners, and monitoring vital signs constantly is imperative.
I’m taking time to compose this information because it needs to be shared that there is an option available most people have not heard about.❞
~ 10almonds reader (slightly edited for formatting and privacy)
Thank you for that! Definitely valuable information for people to know, and (if applicable for oneself or perhaps a loved one) ask about when it comes to local options.
We see it’s also being studied for its potential against other neurological conditions, too:
❝The combination of ibogaine and antidepressants produces a synergistic effect in reducing symptoms of psychiatric disorders such as bipolar disorder, depression, schizophrenia, paranoia, anxiety, panic disorder, mania, post-traumatic stress disorder (PTSD), and obsessive–compulsive disorder. Though ibogaine and the antidepressant act in different pathways, together they provide highly efficient therapeutic responses compared to when each of the active agents is used alone.❞
Read more: Ibogaine and Their Analogs as Therapeutics for Neurological and Psychiatric Disorders
For those who missed it, today’s information about ibogaine was in response to our article:
Let’s Get Letting Go (Of These Three Things)
…which in turn referenced our previous main feature:
Which Addiction-Quitting Methods Work Best?
Take care!
Share This Post
-

Lycopene’s Benefits For The Gut, Heart, Brain, & More
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What Doesn’t Lycopene Do?
Lycopene is an antioxidant carotenoid famously found in tomatoes; it actually appears in even higher levels in watermelon, though. If you are going to get it from tomato, know that cooking improves the lycopene content rather than removing it (watermelon, on the other hand, can be enjoyed as-is and already has the higher lycopene content).
Antioxidant properties
Let’s reiterate the obvious first, for the sake of being methodical and adding a source. Lycopene is a potent antioxidant with multiple health benefits:
Lycopene: A Potent Antioxidant with Multiple Health Benefits
…and as such, it does all the things you might reasonably expect and antioxidant to do. For example…
Anti-inflammatory properties
In particular, it regulates macrophage activity, reducing inflammation while improving immune response:
Lycopene Regulates Macrophage Immune Response through the Autophagy Pathway Mediated by RIPK1
As can be expected of most antioxidants and anti-inflammatory agents, it also has…
Anticancer properties
Scientific papers tend to be “per cancer type”, so we’re just going to give one example, but there’s pretty much evidence for its utility against most if not all types of cancer. We’re picking prostate cancer though, as it’s one that’s been studied the most in the context of lycopene intake—in this study, for example, it was found that men who enjoyed at least two servings of lycopene-rich tomato sauce per week were 30% less likely to develop prostate cancer than those who didn’t:
Dietary lycopene intake and risk of prostate cancer defined by ERG protein expression
If you’d like to see something more general, however, then check out:
Potential Use of Tomato Peel, a Rich Source of Lycopene, for Cancer Treatment
It also fights Candida albicans
Ok, this is not (usually) so life-and-death as cancer, but reducing our C. albicans content (specifically: in our gut) has a lot of knock-on effects for other aspects of our health, so this isn’t one to overlook:
The title does not make this clear, but yes: this does mean it has an antifungal effect. We mention this because often cellular apoptosis is good for an overall organism, but in this case, it simply kills the Candida.
It’s good for the heart
A lot of studies focus just on triglyceride markers (which lycopene improves), but more tellingly, here’s a 10-year observational study in which diets rich in lycopene were associated to a 17–26% lower risk of heart disease:
Relationship of lycopene intake and consumption of tomato products to incident CVD
…and a 39% overall reduced mortality in, well, we’ll let the study title tell it:
…which means also:
It’s good for the brain
As a general rule of thumb, what’s good for the heart is good for the brain (because the brain needs healthy blood flow to stay healthy, and is especially vulnerable when it doesn’t get that), and in this case that rule of thumb is also borne out by the post hoc evidence, specifically yielding a 31% decreased incidence of stroke:
Dietary and circulating lycopene and stroke risk: a meta-analysis of prospective studies
Is it safe?
As a common food product, it is considered very safe.
If you drink nothing but tomato juice all day for a long time, your skin will take on a reddish hue, which will go away if you stop getting all your daily water intake in tomato juice.
In all likelihood, even if you went to extremes, you would get sick from the excess of vitamin A (generally present in the same foods) sooner than you’d get sick from the excess of lycopene.
Want to try some?
We don’t sell it, and also we recommend simply enjoying tomatoes, watermelons, etc, but if you do want a supplement, here’s an example product on Amazon
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Age of Scientific Wellness – by Dr. Leroy Hood & Dr. Nathan Price
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We don’t usually do an author bio beyond mentioning their professional background, but in this case it’s worth mentioning that the first-listed author, Dr. Leroy Hood, is the one who invented the automated gene sequencing technology that made the Human Genome Project possible. In terms of awards, he’s won everything short of a Nobel Prize, and that’s probably less a snub and more a matter of how there isn’t a Nobel Prize for Engineering—his field is molecular biotechnology, but what he solved was an engineering problem.
In this book, the authors set out to make the case that “find it and fix it” medicine has done a respectable job of getting us where we are, but what we need now is P4 medicine:
- Predict
- Prevent
- Personalize
- Participate
The idea is that with adequate data (genomic, phenomic, and digital), we can predict the course of health sufficiently well to interrupt the process of disease at its actual (previously unseen) starting point, instead of waiting for symptoms to show up, thus preventing it proactively. The personalization is because this will not be a “one size fits all” approach, since our physiologies are different, our markers of health and disease will be somewhat too. And the participatory aspect? That’s because the only way to get enough data to do this for an entire population is with—more or less—an entire population’s involvement.
This is what happens when, for example, your fitness tracker asks if it can share anonymized health metrics for research purposes and you allow it—you are becoming part of the science (a noble and worthy act!).
You may be wondering whether this book has health advice, or is more about the big picture. And, the answer is both. It’s mostly about the big picture but it does have a lot of (data-driven!) health advice too, especially towards the end.
The style is largely narrative, talking the reader through the progresses (and setbacks) that have marked the path so far, and projecting the next part of the journey, in the hope that we can avoid being part of a generation born just too late to take advantage of this revolutionary approach to health.
Bottom line: this isn’t a very light read, but it is a worthwhile one, and it’ll surely inspire you to increase the extent to which you are proactive about your health!
Click here to check out The Age Of Scientific Wellness, and be part of it!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What’s the difference between a food allergy and an intolerance?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
At one time or another, you’ve probably come across someone who is lactose intolerant and might experience some unpleasant gut symptoms if they have dairy. Maybe it’s you – food intolerances are estimated to affect up to 25% of Australians.
Meanwhile, cow’s milk allergy is one of the most common food allergies in infants and young children, affecting around one in 100 infants.
But what’s the difference between food allergies and food intolerances? While they might seem alike, there are some fundamental differences between the two.
Feel good studio/Shutterstock What is an allergy?
Australia has one of the highest rates of food allergies in the world. Food allergies can develop at any age but are more common in children, affecting more than 10% of one-year-olds and 6% of children at age ten.
A food allergy happens when the body’s immune system mistakenly reacts to certain foods as if they were dangerous. The most common foods that trigger allergies include eggs, peanuts and other nuts, milk, shellfish, fish, soy and wheat.
Mild to moderate signs of food allergy include a swollen face, lips or eyes; hives or welts on your skin; or vomiting. A severe allergic reaction (called anaphylaxis) can cause trouble breathing, persistent dizziness or collapse.
What is an intolerance?
Food intolerances (sometimes called non-allergic reactions) are also reactions to food, but they don’t involve your immune system.
For example, lactose intolerance is a metabolic condition that happens when the body doesn’t produce enough lactase. This enzyme is needed to break down the lactose (a type of sugar) in dairy products.
Food intolerances can also include reactions to natural chemicals in foods (such as salicylates, found in some fruits, vegetables, herbs and spices) and problems with artificial preservatives or flavour enhancers.
Lactose intolerance is caused by a problem with breaking down lactose in milk. Pormezz/Shutterstock Symptoms of food intolerances can include an upset stomach, headaches and fatigue, among others.
Food intolerances don’t cause life-threatening reactions (anaphylaxis) so are less dangerous than allergies in the short term, although they can cause problems in the longer term such as malnutrition.
We don’t know a lot about how common food intolerances are, but they appear to be more commonly reported than allergies. They can develop at any age.
It can be confusing
Some foods, such as peanuts and tree nuts, are more often associated with allergy. Other foods or ingredients, such as caffeine, are more often associated with intolerance.
Meanwhile, certain foods, such as cow’s milk and wheat or gluten (a protein found in wheat, rye and barley), can cause both allergic and non-allergic reactions in different people. But these reactions, even when they’re caused by the same foods, are quite different.
For example, children with a cow’s milk allergy can react to very small amounts of milk, and serious reactions (such as throat swelling or difficulty breathing) can happen within minutes. Conversely, many people with lactose intolerance can tolerate small amounts of lactose without symptoms.
There are other differences too. Cow’s milk allergy is more common in children, though many infants will grow out of this allergy during childhood.
Lactose intolerance is more common in adults, but can also sometimes be temporary. One type of lactose intolerance, secondary lactase deficiency, can be caused by damage to the gut after infection or with medication use (such as antibiotics or cancer treatment). This can go away by itself when the underlying condition resolves or the person stops using the relevant medication.
Whether an allergy or intolerance is likely to be lifelong depends on the food and the reason that the child or adult is reacting to it.
Allergies to some foods, such as milk, egg, wheat and soy, often resolve during childhood, whereas allergies to nuts, fish or shellfish, often (but not always) persist into adulthood. We don’t know much about how likely children are to grow out of different types of food intolerances.
How do you find out what’s wrong?
If you think you may have a food allergy or intolerance, see a doctor.
Allergy tests help doctors find out which foods might be causing your allergic reactions (but can’t diagnose food intolerances). There are two common types: skin prick tests and blood tests.
In a skin prick test, doctors put tiny amounts of allergens (the things that can cause allergies) on your skin and make small pricks to see if your body reacts.
A blood test checks for allergen-specific immunoglobulin E (IgE) antibodies in your blood that show if you might be allergic to a particular food.
Blood tests can help diagnose allergies. RossHelen/Shutterstock Food intolerances can be tricky to figure out because the symptoms depend on what foods you eat and how much. To diagnose them, doctors look at your health history, and may do some tests (such as a breath test). They may ask you to keep a record of foods you eat and timing of symptoms.
A temporary elimination diet, where you stop eating certain foods, can also help to work out which foods you might be intolerant to. But this should only be done with the help of a doctor or dietitian, because eliminating particular foods can lead to nutritional deficiencies, especially in children.
Is there a cure?
There’s currently no cure for food allergies or intolerances. For allergies in particular, it’s important to strictly avoid allergens. This means reading food labels carefully and being vigilant when eating out.
However, researchers are studying a treatment called oral immunotherapy, which may help some people with food allergies become less sensitive to certain foods.
Whether you have a food allergy or intolerance, your doctor or dietitian can help you to make sure you’re eating the right foods.
Victoria Gibson, a Higher Degree by Research student and Research Officer at the School of Nursing, Midwifery and Social Work at the University of Queensland, and Rani Scott-Farmer, a Senior Research Assistant at the University of Queensland, contributed to this article.
Jennifer Koplin, Group Leader, Childhood Allergy & Epidemiology, The University of Queensland and Desalegn Markos Shifti, Postdoctoral Research Fellow, Child Health Research Centre, Faculty of Medicine, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: