How old’s too old to be a doctor? Why GPs and surgeons over 70 may need a health check to practise
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A growing number of complaints against older doctors has prompted the Medical Board of Australia to announce today that it’s reviewing how doctors aged 70 or older are regulated. Two new options are on the table.
The first would require doctors over 70 to undergo a detailed health assessment to determine their current and future “fitness to practise” in their particular area of medicine.
The second would require only general health checks for doctors over 70.
A third option acknowledges existing rules requiring doctors to maintain their health and competence. As part of their professional code of conduct, doctors must seek independent medical and psychological care to prevent harming themselves and their patients. So, this third option would maintain the status quo.

Haven’t we moved on from set retirement ages?
It might be surprising that stricter oversight of older doctors’ performance is proposed now. Critics of mandatory retirement ages in other fields – for judges, for instance – have long questioned whether these rules are “still valid in a modern society”.
However, unlike judges, doctors are already required to renew their registration annually to practise. This allows the Medical Board of Australia not only to access sound data about the prevalence and activity of older practitioners, but to assess their eligibility regularly and to conduct performance assessments if and when they are needed.
What has prompted these proposals?
This latest proposal identifies several emerging concerns about older doctors. These are grounded in external research about the effect of age on doctors’ competence as well as the regulator’s internal data showing surges of complaints about older doctors in recent years.
Studies of medical competence in ageing doctors show variable results. However, the Medical Board of Australia’s consultation document emphasises studies of neurocognitive loss. It explains how physical and cognitive impairment can lead to poor record-keeping, improper prescribing, as well as disruptive behaviour.
The other issue is the number of patient complaints against older doctors. These “notifications” have surged in recent years, as have the number of disciplinary actions against older doctors.
In 2022–2023, the Medical Board of Australia took disciplinary action against older doctors about 1.7 times more often than for doctors under 70.
In 2023, notifications against doctors over 70 were 81% higher than for the under 70s. In that year, patients sent 485 notifications to the Medical Board of Australia about older doctors – up from 189 in 2015.
While older doctors make up only about 5.3% of the doctor workforce in Australia (less than 1% over 80), this only makes the high numbers of complaints more starkly disproportionate.
It’s for these reasons that the Medical Board of Australia has determined it should take further regulatory action to safeguard the health of patients.
So what distinguishes the two new proposed options?
The “fitness to practise” assessment option would entail a rigorous assessment of doctors over 70 based on their specialisation. It would be required every three years after the age of 70 and every year after 80.
Surgeons, for example, would be assessed by an independent occupational physician for dexterity, sight and the ability to give clinical instructions.
Importantly, the results of these assessments would usually be confidential between the assessor and the doctor. Only doctors who were found to pose a substantial risk to the public, which was not being managed, would be obliged to report their health condition to the Medical Board of Australia.
The second option would be a more general health check not linked to the doctor’s specific role. It would occur at the same intervals as the “fitness to practise” assessment. However, its purpose would be merely to promote good health-care decision-making among health practitioners. There would be no general obligation on a doctor to report the results to the Medical Board of Australia.
In practice, both of these proposals appear to allow doctors to manage their own general health confidentially.

The law tends to prioritise patient safety
All state versions of the legal regime regulating doctors, known as the National Accreditation and Registration Scheme, include a “paramountcy” provision. That provision basically says patient safety is paramount and trumps all other considerations.
As with legal regimes regulating childcare, health practitioner regulation prioritises the health and safety of the person receiving the care over the rights of the licensed professional.
Complicating this further, is the fact that a longstanding principle of health practitioner regulation has been that doctors should not be “punished” for errors in practice.
All of this means that reforms of this nature can be difficult to introduce and that the balance between patient safety and professional entitlements must be handled with care.
Could these proposals amount to age discrimination?
It is premature to analyse the legal implications of these proposals. So it’s difficult to say how these proposals interact with Commonwealth age- and other anti-discrimination laws.
For instance, one complication is that the federal age discrimination statute includes an exemption to allow “qualifying bodies” such as the Medical Board of Australia to discriminate against older professionals who are “unable to carry out the inherent requirements of the profession, trade or occupation because of his or her age”.
In broader terms, a licence to practise medicine is often compared to a licence to drive or pilot an aircraft. Despite claims of discrimination, New South Wales law requires older drivers to undergo a medical assessment every year; and similar requirements affect older pilots and air traffic controllers.
Where to from here?
When changes are proposed to health practitioner regulation, there is typically much media attention followed by a consultation and behind-the-scenes negotiation process. This issue is no different.
How will doctors respond to the proposed changes? It’s too soon to say. If the proposals are implemented, it’s possible some older doctors might retire rather than undergo these mandatory health assessments. Some may argue that encouraging more older doctors to retire is precisely the point of these proposals. However, others have suggested this would only exacerbate shortages in the health-care workforce.
The proposals are open for public comment until October 4.
Christopher Rudge, Law lecturer, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How Beneficial Is MCT Oil, Really?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Often derived from coconuts (though it doesn’t have to be), medium-chain triglycerides (MCTs) are trendy… But does the science back the hype?
First, the principle
MCTs are commonly enjoyed because unlike short- or long-chain fatty acids, they can be quickly broken down and either immediately converted quickly and easily into energy, or turned into ketones in the case of a surplus (in the case of true excess, however, it’ll simply be stored as fat).
Most of that involves the liver, so for anyone who wants a refresher on liver health:
How To Unfatty A Fatty Liver ← notwithstanding the title, this is also important knowledge even if your liver is healthy now—if you’d like it to stay healthy, anyway!
You can also read about the ins and outs of glycogen metabolism and the body’s energy-based metabolic processes in general (including the body’s energy processes that go on in the liver), here:
From Apples to Bees, and High-Fructose Cs: Which Sugars Are Healthier, And Which Are Just The Same?
If the liver turns the MCTs into ketones, those ketones will then be used for energy if there is insufficient glucose available (as the body will always use glucose from the blood first, if available, before moving to alternative energy sources such as ketones and/or fat reserves.)
Thus, many people look to ketones as a solution for having enough energy to function while on a very low-carb diet such as the ketogenic diet:
Ketogenic Diet: Burning Fat Or Burning Out?
…which as you’ll recall, does work for short-term weight loss, but brings long-term health risks, so should not be undertaken for long periods of time.
So, does MCT Oil help?
With regard to weight loss, the research is weak and mixed:
- Weak, because often the methodology was shoddy, often there are many factors not controlled-for, and often the sample sizes were small (and also, RCTs by their very nature tend to be quite short-term (often 6, 8, or 12 weeks), whereas heavy reliance on ketones from MCTs may fall into the same long-term problems as the ketogenic diet in general).
- Mixed, because the results varied widely (probably because of the aforementioned problems).
Rather than pick at individual studies, let’s look at this review and meta-analysis of 13 studies, with a combined sample size of 749 people (so you can imagine how small the individual RCTs were):
❝Compared with LCTs, MCTs decreased body weight (-0.51 kg [95% CI-0.80 to -0.23 kg]; P<0.001; I(2)=35%); waist circumference (-1.46 cm [95% CI -2.04 to -0.87 cm]; P<0.001; I(2)=0%), hip circumference (-0.79 cm [95% CI -1.27 to -0.30 cm]; P=0.002; I(2)=0%), total body fat (standard mean difference -0.39 [95% CI -0.57 to -0.22]; P<0.001; I(2)=0%), total subcutaneous fat (standard mean difference -0.46 [95% CI -0.64 to -0.27]; P<0.001; I(2)=20%), and visceral fat (standard mean difference -0.55 [95% CI -0.75 to -0.34]; P<0.001; I(2)=0%).
No differences were seen in blood lipid levels.
Many trials lacked sufficient information for a complete quality assessment, and commercial bias was detected.❞
So, if we’re going to take those numbers at face value, that means a net weight loss, over the course of the trial period, was…
*drumroll*
0.51kg (that’s about 1 lb).
To put that into perspective, if you did nothing else but pee 1 cup of urine before getting weighed, you’d register as having lost 0.25kg (or about ½ lb) by virtue of the bathroom trip alone.
Here’s the paper:
What about cholesterol and heart health?
With regard to cholesterol, MCT oil is touted as improving blood lipids, which means lowering LDL and increasing HDL (within a safe range, anyway).
You’ll remember that the above review concluded “No differences were seen in blood lipid levels”.
It may again be a case of individual studies cancelling each other out. For example…
This study found that it improved lipids in 40 young women as part of a calorie-controlled interventional diet:
This study found that it worsened lipids in 17 young men, worse even than taking an equivalent amount of sunflower oil:
In short, it’s a gamble.
It may be good for insulin sensitivity, though
This one seems to be specific to people with type 2 diabetes. The paper heading says it all, but we include the link in case you want to know the details (the short version is, it improved insulin sensitivity in diabetic subjects only (not others), and didn’t affect anything else that was measured:
The sample size was small (20 people total, of whom 10 had diabetes), and the next study was with 40 people, this time moderately overweight and all with type 2 diabetes:
Want to try some?
We don’t sell it, but here for your convenience is an example product on Amazon 😎
Enjoy!
Share This Post
-
Kidney Beans vs Red Lentils – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing kidney beans to red lentils, we picked the lentils.
Why?
Both are excellent! But…
In terms of macros, kidney beans have more carbs, while the lentils have more fiber and protein; an easy first-round win for lentils.
In the category of vitamins, kidney beans have more vitamin K (appropriately enough), while lentils have more of vitamins B1, B2, B3, B5, B6, B7, B9, C, and E, winning this round too.
Looking at minerals, kidney beans have more calcium and magnesium, while lentils have more copper, iron, manganese, phosphorus, selenium, and zinc, winning their third round in a row.
Adding up the sections makes for a clear overall win for red lentils, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
What Do The Different Kinds Of Fiber Do? 30 Foods That Rank Highest
Enjoy!
Share This Post
-
I have a stuffy nose, how can I tell if it’s hay fever, COVID or something else?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hay fever (also called allergic rhinitis) affects 24% of Australians. Symptoms include sneezing, a runny nose (which may feel blocked or stuffy) and itchy eyes. People can also experience an itchy nose, throat or ears.
But COVID is still spreading, and other viruses can cause cold-like symptoms. So how do you know which one you’ve got?

Lysenko Andrii/Shutterstock Remind me, how does hay fever cause symptoms?
Hay fever happens when a person has become “sensitised” to an allergen trigger. This means a person’s body is always primed to react to this trigger.
Triggers can include allergens in the air (such as pollen from trees, grasses and flowers), mould spores, animals or house dust mites which mostly live in people’s mattresses and bedding, and feed on shed skin.
When the body is exposed to the trigger, it produces IgE (immunoglobulin E) antibodies. These cause the release of many of the body’s own chemicals, including histamine, which result in hay fever symptoms.
People who have asthma may find their asthma symptoms (cough, wheeze, tight chest or trouble breathing) worsen when exposed to airborne allergens. Spring and sometimes into summer can be the worst time for people with grass, tree or flower allergies.
However, animal and house dust mite symptoms usually happen year-round.
Ryegrass pollen is a common culprit. bangku ceria/Shutterstock What else might be causing my symptoms?
Hay fever does not cause a fever, sore throat, muscle aches and pains, weakness, loss of taste or smell, nor does it cause you to cough up mucus.
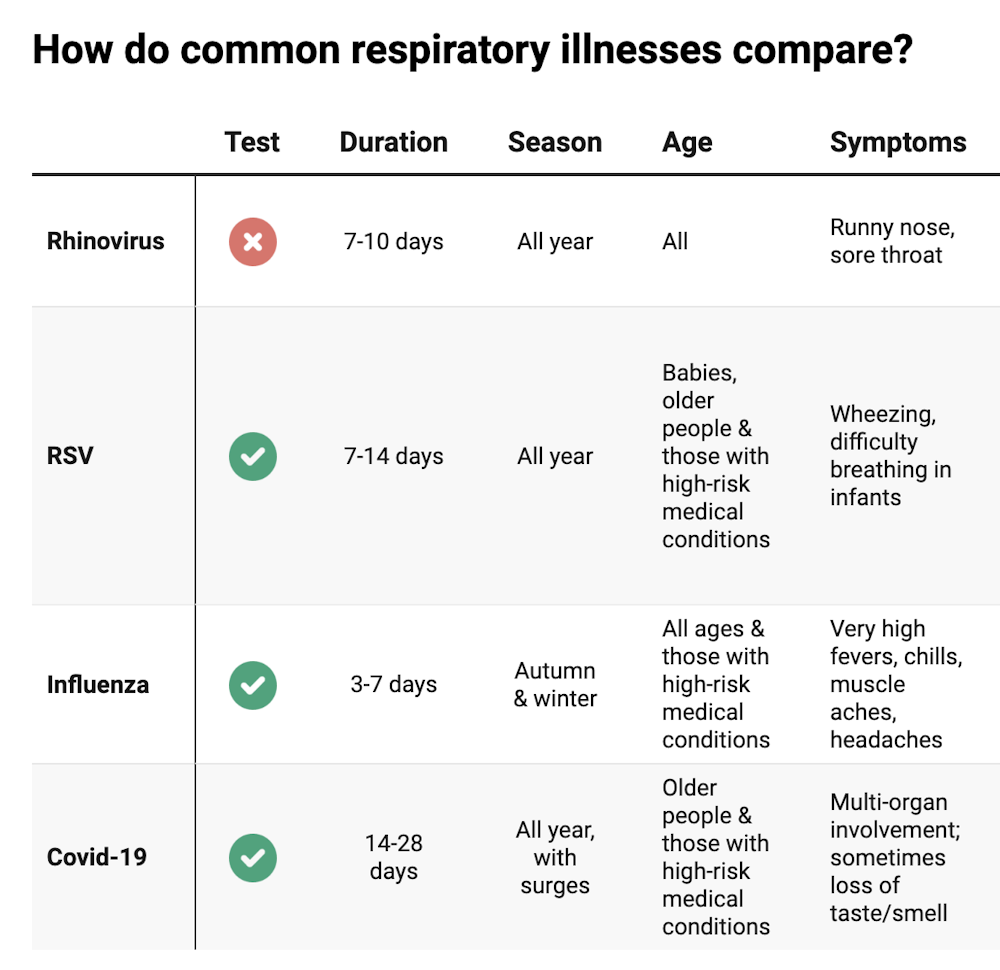
These symptoms are likely to be caused by a virus, such as COVID, influenza, respiratory syncytial virus (RSV) or a “cold” (often caused by rhinoviruses). These conditions can occur all year round, with some overlap of symptoms:
Natasha Yates/The Conversation COVID still surrounds us. RSV and influenza rates appear higher than before the COVID pandemic, but it may be due to more testing.
So if you have a fever, sore throat, muscle aches/pains, weakness, fatigue, or are coughing up mucus, stay home and avoid mixing with others to limit transmission.
People with COVID symptoms can take a rapid antigen test (RAT), ideally when symptoms start, then isolate until symptoms disappear. One negative RAT alone can’t rule out COVID if symptoms are still present, so test again 24–48 hours after your initial test if symptoms persist.
You can now test yourself for COVID, RSV and influenza in a combined RAT. But again, a negative test doesn’t rule out the virus. If your symptoms continue, test again 24–48 hours after the previous test.
If it’s hay fever, how do I treat it?
Treatment involves blocking the body’s histamine release, by taking antihistamine medication which helps reduce the symptoms.
Doctors, nurse practitioners and pharmacists can develop a hay fever care plan. This may include using a nasal spray containing a topical corticosteroid to help reduce the swelling inside the nose, which causes stuffiness or blockage.
Nasal sprays need to delivered using correct technique and used over several weeks to work properly. Often these sprays can also help lessen the itchy eyes of hay fever.
Drying bed linen and pyjamas inside during spring can lessen symptoms, as can putting a smear of Vaseline in the nostrils when going outside. Pollen sticks to the Vaseline, and gently blowing your nose later removes it.
People with asthma should also have an asthma plan, created by their doctor or nurse practitioner, explaining how to adjust their asthma reliever and preventer medications in hay fever seasons or on allergen exposure.
People with asthma also need to be alert for thunderstorms, where pollens can burst into tinier particles, be inhaled deeper in the lungs and cause a severe asthma attack, and even death.
What if it’s COVID, RSV or the flu?
Australians aged 70 and over and others with underlying health conditions who test positive for COVID are eligible for antivirals to reduce their chance of severe illness.
Most other people with COVID, RSV and influenza will recover at home with rest, fluids and paracetamol to relieve symptoms. However some groups are at greater risk of serious illness and may require additional treatment or hospitalisation.
For RSV, this includes premature infants, babies 12 months and younger, children under two who have other medical conditions, adults over 75, people with heart and lung conditions, or health conditions that lessens the immune system response.
For influenza, people at higher risk of severe illness are pregnant women, Aboriginal people, people under five or over 65 years, or people with long-term medical conditions, such as kidney, heart, lung or liver disease, diabetes and decreased immunity.
If you’re concerned about severe symptoms of COVID, RSV or influenza, consult your doctor or call 000 in an emergency.
If your symptoms are mild but persist, and you’re not sure what’s causing them, book an appointment with your doctor or nurse practitioner. Although hay fever season is here, we need to avoid spreading other serious infectious.
For more information, you can call the healthdirect helpline on 1800 022 222 (known as NURSE-ON-CALL in Victoria); use the online Symptom Checker; or visit healthdirect.gov.au or the Australian Society of Clinical Immunology and Allergy.
Deryn Thompson, Eczema and Allergy Nurse; Lecturer, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



-
Creatine’s Brain Benefits Increase With Age
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Creatine is generally thought of as a body-building supplement, and for most young people, that’s all it is. But with extra years come extra advantages, and creatine starts to confer cognitive benefits. Dr. Brad Stanfield shares the science:
What the science says
Although 95% of creatine is stored in muscles, 5% is found in the brain, where it helps produce energy needed for brain processes (and that’s a lot of energy—about 20% of our body’s metabolic base rate is accounted for by our brain).
In this video, Dr. Stanfield shares studies showing creatine improving memory, especially in older adults—and also in vegetarians/vegans, since creatine is found in meat (just like in our own bodies, which are also made of meat) and not in plants. On the meta-analysis level, a systematic review concluded that creatine supplementation indeed improves memory, with stronger effects observed in older adults.
Dr. Stanfield also addresses the safety concerns about creatine, which, on balance, are not actually supported by the science (of course, always consult your own doctor to be sure, as your case could vary).
As for dosage, 5g/day is recommended. For more on all of this plus links to the studies cited, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Creatine: Very Different For Young & Old People
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Think Again – by Adam Grant
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Warning: this book may cause some feelings of self-doubt! Ride them out and see where they go, though.
It was Socrates who famously (allegedly) said “ἓν οἶδα ὅτι οὐδὲν οἶδα”—”I know that I know nothing”.
Adam Grant wants us to take this philosophy and apply it usefully to modern life. How?
The main premise is that rethinking our plans, answers and decisions is a good thing… Not a weakness. In contrast, he says, a fixed mindset closes us to opportunities—and better alternatives.
He wants us to be sure that we don’t fall into the trap of the Dunning-Kruger Effect (overestimating our abilities because of being unaware of how little we know), but he also wants us to rethink whole strategies, too. For example:
Grant’s approach to interpersonal conflict is very remniscent of another book we might review sometime, “Aikido in Everyday Life“. The idea here is to not give in to our knee-jerk responses to simply retaliate in kind, but rather to sidestep, pivot, redirect. This is, admittedly, the kind of “rethinking” that one usually has to rethink in advance—it’s too late in the moment! Hence the value of a book.
Nor is the book unduly subjective. “Wishy-washiness” has a bad rep, but Grant gives us plenty in the way of data and examples of how we can, for example, avoid losses by not doubling down on a mistake.
What, then, of strongly-held core principles? Rethinking doesn’t mean we must change our mind—it simply means being open to the possibility in contexts where such makes sense.
Grant borrows, in effect, from:
❝Do the best you can until you know better. Then when you know better… do better!❞
So, not so much undercutting the principles we hold dear, and instead rather making sure they stand on firm foundations.
All in all, a thought-provokingly inspiring read!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Feel-Good Productivity – by Dr. Ali Abdaal
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Rise and grind” is not a sustainable way to live. Yet for most of us, there are things we do have to do every day that we don’t necessarily do for fun. So, how to be productive with those things, and not feel like we are constantly compromising and sacrificing our time on this earth for some intrinsically trivial but extrinsically required activity that’ll be forgotten tomorrow?
And most of us do also have dreams and ambitions (and if you don’t, then what were they before life snatched them away from you?), things to work towards. So there is “carrot” for us as well as “stick”. But how to break the cycle and get more carrot and less stick, while being more productive than before?
Dr. Abdaal frames this principally in terms of neurology first, psychology next.
That when we are bored, we simply do not have the neurochemicals required to work well anyway, so addressing that first needs to be a priority. He lays out many ways of doing this, gives lots of practical tips, and brings attention to the ways it’s easy to go wrong (and how to fix those too).
The writing style isdeceptively relaxed and casual, leading the reader smoothly into understanding of each topic before moving on.
Bottom line: if you want to get more done while feeling better about it (not a tired wreck), then this is the book for you!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: