How Not To Die – by Dr. Michael Greger
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We previously reviewed this book some years ago, but we’re revisiting it now because:
- It really is a book that should be in every healthspan-enjoyer’s collection
- Our book reviews back then were not as comprehensive as now (though we still generally try to fit into the “it takes about one minute to read this review” idea, sometimes we’ll spend a little extra time).
Dr. Greger (of “Dr. Greger’s Daily Dozen” fame) outlines for us in cold hard facts and stats what’s most likely to be our cause of death. While this is not a cheery premise for a book, he then sets out to work back from there—what could have prevented those specific things?
Thus, while the book doesn’t confer immortality (the title is not “how to not die”, after all), it does teach us how not to die—i.e, from heart disease, lung diseases, brain diseases, digestive cancers, infections, diabetes, high blood pressure, liver disease, blood cancers, kidney disease, breast cancer, suicidal depression, prostate cancer, Parkinson’s disease, and even iatrogenic causes.
This it does with a lot of solid science, explained for the layperson, and/but without holding back when it comes to big words, and a lot of them, at that. If you want to add in daily exercises, just lifting the book could be a start; weighing in at 678 pages, it’s an information-dense tome that’s more likely to be sifted through than read cover-to-cover.
The style is thus dense science somewhat editorialized for lay readability, and well-evidenced with around 3,000 citations. That’s not a typo; there are 178 pages of bibliography at the back with about 15–20 scientific references per page.
In terms of practical use, he does also devote chapters to that, it’s not just all textbook. Indeed, he discusses the reasonings behind the items, portion sizes, and quantities of his “daily dozen” foods, so that the reader will understand how much bang-for-buck they deliver, and then it’ll seem a lot less like an arbitrary list, and more likely to be adopted and maintained.
Bottom line: if you care about not getting life-threatening illnesses (which at the end of the day, come to most people at some point), then this book is a must-read.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Taking prescription opioids for too long can be harmful. Here’s how to cut back and stop

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Opioids, such as oxycodone, morphine, codeine, tramadol and fentanyl, are commonly prescribed to manage pain. You might be given a prescription when experiencing pain, or after surgery or an injury.
But while opioids may relieve pain in the short term, they provide little to no lasting improvement in pain or function beyond a few weeks for people whose pain isn’t caused by cancer.
Opioids can also cause side effects such as nausea, constipation and drowsiness, as well as serious risks such as dependence and overdose.
Over the past decade, Australia has introduced initiatives to reduce opioid use and related harm. This includes new guidelines that recommend reducing the dose or stopping opioids when the risks of continuing outweigh the benefits.
Many people can reduce or stop opioids without their pain worsening. Some people even experience less pain. However, for some people, reducing or stopping opioids can result in worse pain, mental health crises and even suicide.
Our new research, published today in the New England Journal of Medicine, explains how to safely reduce and stop taking prescription opioids.

Maskot/Getty Images How do you know when it’s time to stop? Then what?
Determining whether it is appropriate to reduce or stop opioids depends on several factors unique to each person. These include:
- why opioids were prescribed
- how long they’ve been used
- what other treatments you’ve tried
- how the medication affects your pain, function and quality of life
- your life circumstances.
If it’s appropriate to trial reducing or stopping opioids, guidelines from Australia, the United Kingdom and the United States emphasise the following principles:
1) Shared decision-making
Shared decision-making is where health-care professionals and patients work together to set goals, weigh risks and benefits, and make informed choices.
This means collaboratively designing an opioid reduction plan that reflects the person’s needs, preferences and circumstances, rather than imposing a one-size-fits-all approach.
Research shows shared decision-making may lead to better outcomes, and patients value this process.
2) Reduce gradually
Stopping opioids suddenly can cause withdrawal symptoms such as anxiety, insomnia, and stomach upset. Rapid dose reductions can also increase the risk of overdose, mental distress and suicide.
To avoid these risks, opioids should be reduced gradually over weeks, months or even longer. The process should be flexible, allowing for pauses or adjustments to the reduction plan if needed.
When someone takes lower doses of opioids over time, their body’s tolerance decreases. If they return to a higher dose, there is a risk of overdose. For this reason, health-care professionals may recommend having naloxone available. This is a medication that can reverse an opioid overdose.
3) Set up other supports
Supportive strategies should be used before, during and after reducing opioids. These can include:
- physical therapies such as physiotherapy
- psychological approaches such as mindfulness
- non-opioid medications
- mental health support from health-care professionals, friends and family
- education about pain self-management.
The evidence supporting specific interventions is often limited or uncertain. Choosing a strategy will depend on your individual preferences and access. The best approach is likely a combination of several different supports.
4) See your health-care provider for ongoing monitoring
Regular monitoring from a health-care professional is recommended during and after opioid reduction to assess pain, function, withdrawal symptoms and wellbeing.
This can help to ensure that any issues are identified early and are addressed.
If someone experiences a clear decline in their quality of life, for example, it may be necessary to pause or stop the taper and revisit it later, provide extra supports or implement strategies to manage withdrawal symptoms.
We need a health system that supports this process
Making opioid reduction safer and more effective requires putting these principles into practice. But many patients and health-care professionals still face challenges when doing so.
It’s best practice to access a team-based pain management program with support from a doctor, physiotherapist and psychologist, among other providers, to manage pain and reduce the use of opioids. But access to these services remains limited in many parts of Australia.
Not everyone has access to team-based pain management. Hispanolistic/Getty Images Consumer organisations and professional bodies have called for greater access to team-based pain services so more people, especially those living in rural and under-served areas, can access support.
Australian health-care professionals have also requested more education and training in pain management, prescribing and opioid reduction, as well as stronger evidence about what works, for whom and why. This is so they’re better able to tailor their care to each person’s needs.
Other strategies such as reducing the amount of opioids prescribed – including after surgery – have also been proposed to help prevent long-term opioid use and the need for reduction plans later on.
Aili Langford, Pharmacist, Lecturer, NHMRC Emerging Leadership Fellow, Sydney Pharmacy School, The University of Sydney, University of Sydney and Christine Lin, Professor, Institute for Musculoskeletal Health, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

7 Kinds Of Rest When Sleep Is Not Enough
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Taking Rest Seriously (More Than Just Sleep)
This is Dr. Matthew Edlund. He has 44 years experience as a psychiatrist, and is also a sleep specialist. He has a holistic view of health, which is reflected in his practice; he advocates for “a more complete health: physical, mental, social, and spiritual well-being”.
What does he want us to know?
Sleep, yes
Sleep cannot do all things for us in terms of rest, but it can do a lot, and it is critical. It is, in short, a necessary-but-not-sufficient condition for being well-rested.
See also: Why You Probably Need More Sleep
Rest actively
Rest is generally thought of as a passive activity, if you’ll pardon the oxymoron. Popular thinking is that it’s not something defined by what we do, so much what we stop doing.
In contrast, Dr. Edlund argues that to take rest seriously, we need do restful things.
Rest is as important as eating, and we wouldn’t want for that to “just happen”, would we?
Dr. Edlund advocates for restful activities such as going to the garden (or a nearby park) to relax. He also suggests we not underestimate the power of sex as an actively restful activity—this one is generally safer in the privacy of one’s home, though!
Rest physically
This is about actively relaxing our body—yoga is a great option here, practised in a way that is not physically taxing, but is physically rejuvenating; gentle stretches are key. Without such things, our body will keep tension, and that is not restful.
For the absolute most restful yogic practice? Check out:
Non-Sleep Deep Rest: A Neurobiologist’s Take
this is about yoga nidra!
Rest mentally
The flipside of the above is that we do need to rest our mind also. When we try to rest from a mental activity by taking on a different mental activity that uses the same faculties of the brain, it is not restful.
Writer’s example: as a writer, I could not rest from my writing by writing recreationally, or even by reading. An accountant, however, could absolutely rest from accounting by picking up a good book, should they feel so inclined.
Rest socially
While we all have our preferences when it comes to how much or how little social interaction we like in our lives, humans are fundamentally social creatures, and it is hardwired into us by evolution to function at our best in a community.
This doesn’t mean you have to go out partying every night, but it does mean you should take care to spend at least a little time with friends, even if just once or twice per week, and yes, even if it’s just a videocall (in person is best, but not everyone lives close by!)
If your social life is feeling a little thin on the ground these days, that’s a very common thing—not only as we get older, but also as many social institutions took a dive in functionality on account of the pandemic, and many are still floundering. Nevertheless, there are more options than you probably realize; yes, even for the naturally reclusive:
How To Beat Loneliness & Isolation
Rest spiritually
Be we religious or not, there are scientifically well-evidenced benefits to religious practices—some are because of the social aspect, and follow on from what we talked about just above. Other benefits come from activities such as prayer or meditation (which means that having some kind of faith, while beneficial, is not actually a requirement for spiritual rest—comparable practices without faith are fine too).
We discussed the overlapping practices of prayer and meditation, here:
The Science Of Mantra Meditation
Rest at home
Obviously, most people sleep at home. But…
Busy family homes can sometimes need a bit of conscious effort to create a restful environment, even if just for a while. A family dinner together is one great way to achieve this, and also ties in with the social element we mentioned before!
A different challenge faced by a lot of older people without live-in families, on the other hand, is the feeling of too much opportunity for rest—and then a feeling of shame for taking it. The view is commonly held that, for example, taking an afternoon nap is a sign of weakness.
On the contrary: taking an afternoon nap can be a good source of strength! Check out:
How To Nap Like A Pro (No More “Sleep Hangovers”!)
Rest at work
Our readership has a lot of retirees, but we know that’s not the case for everyone. How then, to rest while at work? Ideally we have breaks, of course, but most workplaces do not exactly have an amusement arcade in the break room. Nevertheless, there are some quick resets that can be done easily, anywhere, and (almost) any time:
Meditation Games: Meditation That You’ll Actually Enjoy
Want to know more?
You might also like:
How To Rest More Efficiently (Yes, Really)
Take care!
Share This Post
-

Parsley vs Watercress – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing parsley to watercress, we picked the parsley.
Why?
It wasn’t close:
In terms of macros, parsley has more than 6x the fiber, more than 4x the carbs, and slightly more protein, winning this round.
In the category of vitamins, parsley has much more of vitamins A, B3, B5, B7, B9, C, K, and choline, while watercress has slightly more of vitamins B2, B6, and E, making a compelling win for parsley.
Looking at minerals, parsley has more calcium, copper, iron, magnesium, potassium, and zinc, while watercress has more manganese and selenium, meaning another easy win for parsley.
In other considerations, parsley scores higher on polyphenols, winning this round too.
Adding up the sections makes for a clear overall win for parsley, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Share This Post




Related Posts
-
How To Reduce Or Quit Alcohol
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Rethinking Drinking
When we’re looking at certain health risks, there are often five key lifestyle factors that have a big impact; they are:
- Have a good diet
- Get good exercise
- Get good sleep
- Reduce (or eliminate) alcohol
- Don’t smoke
Today, we’re focussing the alcohol bit. Maybe you’d like to quit, maybe just cut down, maybe the topic just interests you… So, here’s a quick rundown of some things that will help make that a lot easier:
With a big enough “why”, you can overcome any “how”
Research and understand the harm done by drinking, including:
And especially as we get older, memory problems:
Alcohol-related dementia: an update of the evidence
And as for fear of missing out, or perhaps even of no longer being relaxed/fun… Did you ever, while sober, have a very drunk person try to converse with you, and you thought “I wish that were me”?
Probably not
Know your triggers
Why do you drink? If your knee-jerk response is “because I like it”, dig deeper. What events prompt you to have a drink?
- Some will be pure habit born of convention—perhaps with a meal, for example
- Others may be stress-management—after work, perhaps
- Others may be pseudo-medicinal—a nightcap for better* sleep, for instance
*this will not work. Alcohol may make us sleepy but it will then proceed to disrupt that very sleep and make it less restorative
Become mindful
Now that you know why you’d like to drink less (or quit entirely), and you know what triggers you to drink, you can circumvent that a little, by making deals with yourself, for example
- “I can drink alcohol, if and only if I have consumed a large glass of water first” (cuts out being thirsty as a trigger to drink)
- “I can drink alcohol, if and only if I meditate for at least 5 minutes first” (reduces likelihood of stress-drinking)
- “I can drink alcohol, if and only if it is with the largest meal of the day” (minimizes total alcohol consumption)
Note that these things also work around any FOMO, “Fear Of Missing Out”. It’s easier to say “no” when you know you can have it later if you still want it.
Get a good replacement drink
There are a lot of alcohol-free alcohol-like drinks around these days, and many of them are very good. Experiment and see. But!
It doesn’t even have to be that. Sometimes what we need is not even an alcohol-like drink, but rather, drinkable culinary entertainment.
If you like “punch-in-the-face” flavors (as this writer does), maybe strong black coffee is the answer. If you like “crisp and clear refreshment” (again, same), maybe your favorite herbal tea will do it for you. Or maybe for you it’ll be lemon-water. Or homemade ginger ale.
Whatever it is… make it fun, and make it yours!
Bonus item: find replacement coping strategies
This one goes if you’ve been using alcohol to cope with something. Stress, depression, anxiety, whatever it may be for you.
The thing is, it feels like it helps briefly in the moment, but it makes each of those things progressively worse in the long-run, so it’s not sustainable.
Consider instead things like therapy, exercise, and/or a new hobby to get immersed in; whatever works for you!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What To Do If Having A Stroke Alone?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝Thank you for the video about what to do if you have a heart attack alone, what about what to do if you have a stroke alone?❞
(for anyone who missed that video, here it is)
That’s a good question, especially as stroke risk is rising in the industrialized world in general, and the US in particular.
However, let’s start with the caveat that if you are having a stroke, there’s a good chance you will forget what we are about to say, what with the immediate effects it has on the brain. That said…
The general advice when it comes to looking after someone else who is experiencing a stroke, is, “don’t”.
In other words, call emergency services, and don’t do anything else, e.g:
- don’t give them anything to eat or drink
- don’t give them any medications
- don’t let them go to sleep
- don’t let them talk you out of calling emergency services
- don’t let them drive themselves to hospital
- don’t drive them to hospital yourself either*
*This is for two reasons:
- an ambulance crew has skills and resources that you don’t, and can begin treatment en-route, and also,
- not all hospitals have appropriate resources to treat stroke, so the ambulance crew will know to drive to one that does, instead of driving to a random hospital and hoping for the best
So, flipping this for if it’s you having the stroke, and you’re cognizant enough to remember this:
- do call an ambulance; stay on the line and don’t do anything else unless instructed by the emergency services.
In order to do that, of course it’s important to recognize the symptoms; you probably know these but just in case, the mnemonic is “FAST”:
- Face: is there weakness on one side of their face?
- Arms: if they raise both arms, does one drift downwards?
- Speech: if they speak, is their speech slurred or otherwise unusual?
- Time: to call emergency services
It’s great to not get caught out by surprise, so you might also want to check out:
6 Signs Of Stroke (One Month In Advance)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Spit or swallow? What’s the best way to deal with phlegm?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A spitting pot I consider as an essential part of the bed-room apparatus.
That’s what French physician René Laennec wrote in 1821. Laennec, who invented the stethoscope, spent his days gazing at his patients’ phlegm. In the days before x-rays and blood tests, phlegm was considered a valuable diagnostic tool.
Today, most of us don’t carry around a spitting pot. But a persistent question remains, especially during winter, when noses are dripping and chests are rattling.
When you have a cough, should you spit out phlegm or is it better to swallow it?
It might feel like an odd or even slightly stomach-churning topic, but it’s a remarkably common question patients ask doctors.
Pop Paul-Catalin/Shutterstock What is phlegm?
Phlegm, also known as sputum, is the thick, sticky mucus your lungs and windpipe make. This acts as a defensive barrier to protect them.
Its main ingredients are mucins – large, sugar-coated proteins that trap viruses, bacteria, allergens and dust. These mucins also regulate inflammation and the body’s immune response to bacteria and viruses.
We most commonly see phlegm with viral illness during winter. But phlegm is also evident in other medical conditions including asthma and allergies, bacterial infections, such as sinusitis, or with smoking or exposure to air pollution.
In fact, we’re always making phlegm, even when we are healthy. Cells in the lungs secrete mucus to keep surfaces moist and trap irritants. When we encounter something potentially harmful, such as a virus or allergen, immune cells detect the threat and release signals that tell mucus-producing cells to step up their game.
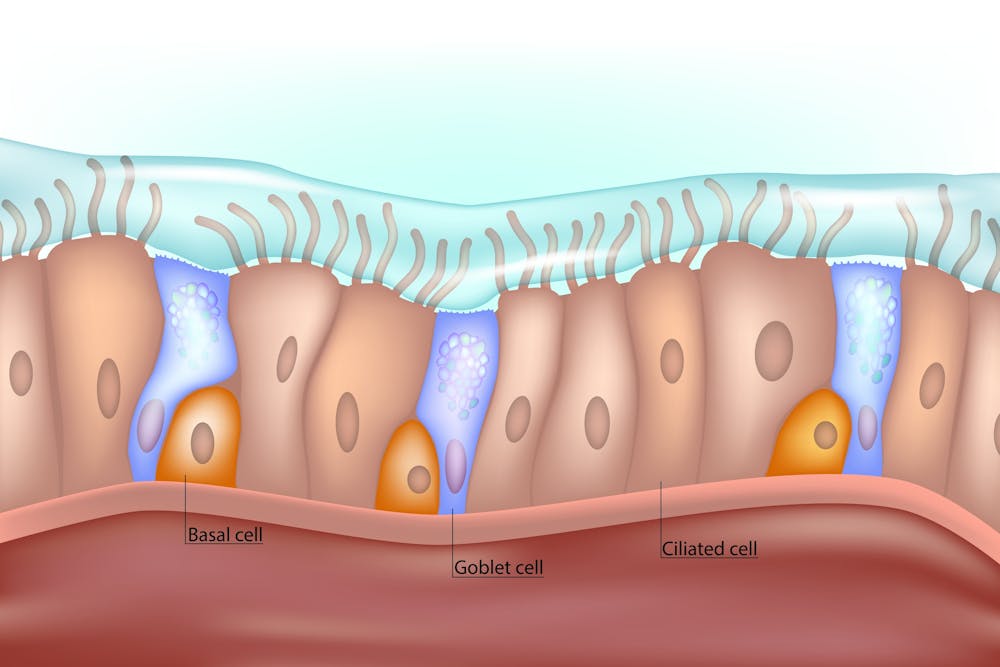
This extra mucus helps trap the invader and move it out of the lungs. Tiny hairs lining the airways (called cilia) then sweep the mucus up to the throat, where we cough it out or swallow it.
These tiny hairs, or cilia, sweep phlegm up to your throat. Sakurra/Shutterstock The case for spitting
Some people feel better if they spit out phlegm, especially if the phlegm is thick, sticky or irritates the throat.
Spitting also lets you see what’s coming up. If phlegm contains blood, for example, it is important to see a doctor to exclude a more serious underlying illness, such as tuberculosis or cancer.
If you do spit out, do so into a tissue and throw it in the bin. Wash your hands afterwards. This reduces the risk of spreading infection to others via respiratory droplets or contaminated surfaces.
However, spitting out phlegm isn’t always practical, or polite. And for most viral infections, it doesn’t help you get better any faster than swallowing. The aim is to remove phlegm from the lungs, which occurs with either method.
Spitting is also not feasible for young children, who haven’t yet developed the coordination to do so effectively. They’ll generally swallow their phlegm. https://www.youtube.com/embed/WW4skW6gucU?wmode=transparent&start=0 How mucus keeps us healthy all year round, even if we’re not sick.
The case for swallowing
It might not sound particularly appealing, but swallowing phlegm is a normal process, and harmless. In fact, we often swallow phlegm without realising it.
The lungs generate about 50 millilitres of phlegm daily. It goes unnoticed because it’s thin, blends with saliva and we continuously swallow it. We only become aware of it when it thickens, such as during a viral infection.
After you swallow phlegm, it travels to the stomach, where acid and enzymes break it down, along with any germs it carries.
Swallowing phlegm doesn’t “recycle” the germs, and it won’t result in the infection spreading elsewhere.
In fact, swallowing viruses can even help build immunity. Once inside the gut, immune cells begin to recognise pieces of the virus and start preparing the body to respond more effectively to it in the future. Some important immunisations, such as the oral polio vaccine, work through this very mechanism.
So, what’s the verdict?
Whether you spit or swallow phlegm, both are safe. Spitting can help some people feel better, especially if their cough is associated with thick phlegm that’s causing distress.
But for most healthy people, there’s no need to force a cough or spit out phlegm. Swallowing phlegm is completely safe. And in young children, it’s the only feasible option.
In the end, it won’t matter if you spit or swallow your phlegm this winter. So choose what feels right (and least icky) for you.
Niall Johnston, Conjoint Associate Lecturer, Faculty of Medicine, UNSW Sydney and Phoebe Williams, Paediatrician & Infectious Diseases Physician; Senior Lecturer & NHMRC Fellow, Faculty of Medicine, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: