How Do Bond-Builders Really Work?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Michelle Wong explains how they do what they do, and also what they don’t do!
It’s bonding time
Let’s get straight into it:
What bond builders claim to do: they’re marketed as repairing broken disulfide bonds inside your hair, but solid evidence for true disulfide repair is limited and controversial, especially regarding early claims made about Olaplex.
A note on chemistry: of the three main bond types going on in human hair, disulfide bonds are the strongest and most structural, ionic or salt bonds are medium strength, and hydrogen bonds are the weakest but very numerous and constantly breaking and reforming with water, heat, and humidity.
What most bond-builders actually seem to do: the best available evidence suggests most bond builders work mainly by forming lots of hydrogen bonds and sometimes ionic bonds with hair proteins, which helps block water from entering and breaking your hair’s natural hydrogen bonds, making your hair less fragile when wet or humid.
Now, blocking water is important, because water disrupts hydrogen bonds between keratin proteins, so if a molecule can sit between proteins and form multiple hydrogen bonds itself, it acts like a more stable “bridge,” reducing swelling and mechanical weakness.
So, what’s in the products that do this? It varies a lot, but common candidates include small acids like maleic acid, succinic acid, malic acid, and citric acid, as well as ingredients like peptides and panthenol, which can hydrogen-bond with keratin; some brands use specialized peptides such as those in K18, which have comparatively stronger published evidence for penetrating and improving hair properties.
However, the science is pretty hairy: most hair research is industry-funded, independent funding is scarce, many studies lack proper controls, and companies often publish only a fraction of their data (specifically, the data that best supports their claims, while holding back data that calls their claims into question or outright contradicts them), making it difficult to directly compare ingredients or formulas.
On which note, the formulation matters as much as the ingredient, because even if an ingredient can hydrogen bond, the overall product determines whether it penetrates your hair, spreads evenly, and also conditions the surface, because rough, under-conditioned hair can feel worse and break more easily even if internal strength improves.
Illustrative analogy: if you buy all the correct materials to build a house, and then put those correct materials in a heap, the result will not necessarily be a well-built house with correct structure and such.
In summary, bond builders don’t magically rebuild every broken disulfide bond (sometimes they don’t even rebuild any disulfide bonds at all), but many can meaningfully improve strength, reduce fragility when wet, and help manage chemical damage, especially when matched to your hair type and level of damage.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Should We Skip Shampoo? ← short answer is “no”, but the science is interesting
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How Vitamin D May Help Protect Against Diabetes

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
…and other items from this week’s health science news:
D vs D
Vitamin D may help protect you from diabetes… Or it may not. The science is clear on this!
In other words: the data (with a large amount of data analysis and a RCT with 2,098 people with prediabetes) is clear about the effect in general, and what that science says, is that whether or not it helps you as an individual, will depend on your genes.
Specifically:
- Participants with the AA variation of the vitamin D receptor gene showed no meaningful response when taking 4,000 IU of vitamin D daily compared with a placebo.
- Participants with AC or CC in the the vitamin D receptor gene had a 19% lower risk of developing diabetes when taking 4,000 IU of vitamin D daily compared with a placebo.
Why the genetic variation matters: vitamin D must bind to the vitamin D receptor to work in your body, and differences in this receptor—particularly in insulin-producing cells in your pancreas—will affect how well vitamin D helps regulate blood sugar.
So, this one’s a case for personalized prevention, where a simple genetic test could identify who is likely to benefit from higher vitamin D intake.
Read in full: Vitamin D may help prevent diabetes
Related: The Real Benefit Of Genetic Testing
Relighting the brain’s fire for happiness
Researchers (Dr. Alice Meuret et al.) have found that a therapy that directly targets lost pleasure (anhedonia*) improves depression and anxiety more than standard treatments that mainly reduce negative emotions.
*It’s not just about pleasure in the sense most might speak of such, though; anhedonia is the reduced or absent ability to feel positive emotions in general. It affects nearly all people with depression, and is strongly linked to worse outcomes, relapse, and suicidal risk.
The problem with standard therapies: most treatments focus on reducing sadness, fear, or distress, but largely ignore rebuilding positive emotions—even though patients often see that as their main goal.
Positive Affect Treatment (PAT), in contrast, is a 15-session psychotherapy designed to restore joy, motivation, meaning, and reward sensitivity. Specifically, it targets the brain’s reward system by encouraging engagement in meaningful activities, shifting attention towards positive experiences, and practising gratitude, savoring, and compassion-based exercises.
As for how well it works: the RCT of 98 adults with severe anhedonia, depression, and anxiety compared PAT to a conventional therapy focused on negative emotions. The results? PAT produced greater overall clinical improvement, including reductions in both depression and anxiety, even though it never directly targeted negative emotions.
Read in full: Targeting lost pleasure lifts depression and anxiety more than standard therapy, new study finds
Related: Behavioral Activation Against Depression & Anxiety
Allergy season feeling different this year?
Due to climate change, pollen seasons are starting earlier, lasting longer, and even overlapping. because of warmer temperatures and higher CO₂, which keeps your immune system in overdrive for longer and leads to more intense symptoms.
Air pollution (which is getting steadily worse in the US and likely many other places too) can also alter pollen particles, making them more irritating to your airways and increasing inflammation.
Children’s symptoms are easy to miss: kids may show allergies through mouth breathing, fatigue, irritability, sleep issues, ear infections, or dark circles under your eyes rather than clearly describing symptoms.
A very common mistake (regardless of age), is starting treatment too late, and/or using medication only when symptoms become onerous, but by this time, your immune system has already been overworked, and taking anti-allergy meds now won’t mean the already-in-progress war in your body suddenly stops instantly.
So instead, you might consider starting allergy medication before symptoms peak, and then taking it consistently for a few weeks (even if the symptoms stop, because that is what the meds are for!), to prevent your immune response from ramping up.
Read in full: Are you managing your allergies the wrong way?
Related: Antihistamines’ Generation Gap
Take care!
Share This Post
-
New Year, New Health Habits?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s that time of the year, and many of us hope to make this our healthiest year yet—or at least significantly improve it in some particular area that’s important to us! So, what news from the health world?
The rise of GLP-1 agonists continues
GLP-1 agonists have surged in popularity in the past year, and it looks like that trend is set to continue in the new one. The title of the below-linked pop-science article is slightly misleading, it’s not “almost three quarters of UK women”, but rather, “72% of the women using the digital weight loss platform Juniper”, which means the sample is confined to people interested in weight loss. Still, of those interested in weight loss, 72% is a lot, and the sample size was over 1000:
Read in full: New Year, new approach to weight loss: Almost three quarters of UK women are considering using GLP-1s in 2025
Related: 5 ways to naturally boost the “Ozempic Effect” ← these natural methods “hack” the same metabolic pathways as GLP-1 agonists do (it has to do with incretin levels), causing similar results
The lesser of two evils
Smoking is terrible, for everything. Vaping is… Not great, honestly, but as the below-discussed study shows, at the very least it results in much less severe respiratory symptoms than actual smoking. For many, vaping is a halfway-house to actually quitting; for some, it’s just harm reduction, and that too can be worthwhile.
We imagine that probably very few 10almonds readers smoke cigarettes, but we know quite a few use cannabis, which is discussed also:
Read in full: Switching to e-cigarettes may ease respiratory symptoms, offering hope for smokers
Related: Vaping: A Lot Of Hot Air? ← we look at the pros, cons, and popular beliefs that were true a little while ago but now they’re largely not (because of regulatory changes re what’s allowed in vapes)
Sometimes, more is more
The below-linked pop-science article has a potentially confusingly-worded title that makes it sound like increased exercise duration results in decreasing marginal returns (i.e., after a certain point, you’re getting very limited extra benefits), but in fact the study says the opposite.
Rather, increased moderate exercise (so, walking etc) results in a commensurately decreasing weight and a decreasing waistline.
In short: walk more, lose more (pounds and inches). The study examined those who moved their bodies for 150–300 minutes per week:
Read in full: Increased exercise duration linked to decreasing results in weight and waistline
Related: The Doctor Who Wants Us To Exercise Less, & Move More
Take care!
Share This Post
-

Aspirin, CVD Risk, & Potential Counter-Risks
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Aspirin Pros & Cons

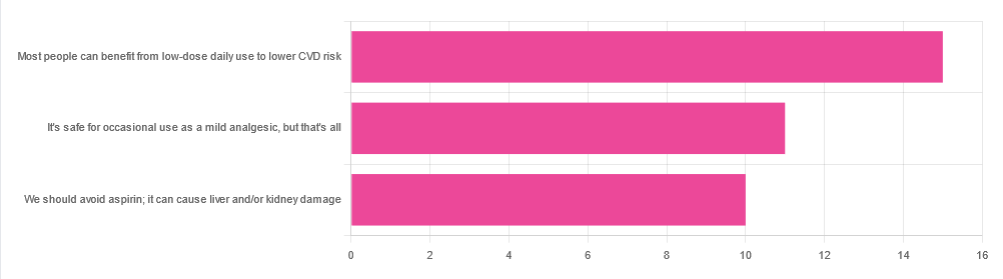
In Tuesday’s newsletter, we asked your health-related opinion of aspirin, and got the above-depicted, below-described set of responses:
- About 42% said “Most people can benefit from low-dose daily use to lower CVD risk”
- About 31% said “It’s safe for occasional use as a mild analgesic, but that’s all”
- About 28% said “We should avoid aspirin; it can cause liver and/or kidney damage”
So, what does the science say?
Most people can benefit from low-dose daily aspirin use to lower the risk of cardiovascular disease: True or False?
True or False depending on what we mean by “benefit from”. You see, it works by inhibiting platelet function, which means it simultaneously:
- decreases the risk of atherothrombosis
- increases the risk of bleeding, especially in the gastrointestinal tract
When it comes to balancing these things and deciding whether the benefit merits the risk, you might be asking yourself: “which am I most likely to die from?” and the answer is: neither
While aspirin is associated with a significant improvement in cardiovascular disease outcomes in total, it is not significantly associated with reductions in cardiovascular disease mortality or all-cause mortality.
In other words: speaking in statistical generalizations of course, it may improve your recovery from minor cardiac events but is unlikely to help against fatal ones
The current prevailing professional (amongst cardiologists) consensus is that it may be recommended for secondary prevention of ASCVD (i.e. if you have a history of CVD), but not for primary prevention (i.e. if you have no history of CVD). Note: this means personal history, not family history.
In the words of the Journal of the American College of Cardiology:
❝Low-dose aspirin (75-100 mg orally daily) might be considered for the primary prevention of ASCVD among select adults 40 to 70 years of age who are at higher ASCVD risk but not at increased bleeding risk (S4.6-1–S4.6-8).
Low-dose aspirin (75-100 mg orally daily) should not be administered on a routine basis for the primary prevention of ASCVD among adults >70 years of age (S4.6-9).
Low-dose aspirin (75-100 mg orally daily) should not be administered for the primary prevention of ASCVD among adults of any age who are at increased risk of bleeding (S4.6-10).❞
~ Dr. Donna Arnett et al. (those section references are where you can find this information in the document)
Read in full: Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology
Or if you’d prefer a more pop-science presentation:
Many older adults still use aspirin for CVD prevention, contrary to clinical guidance
Aspirin can cause liver and/or kidney damage: True or False?
True, but that doesn’t mean we must necessarily abstain, so much as exercise caution.
Aspirin is (at recommended doses) not usually hepatotoxic (toxic to the liver), but there is a strong association between aspirin use in children and the development of Reye’s syndrome, a disease involving encephalopathy and a fatty liver. For this reason, most places have an official recommendation that aspirin not be used by children (cut-off age varies from place to place, for example 12 in the US and 16 in the UK, but the key idea is: it’s potentially dangerous for those who are not fully grown).
Aspirin is well-established as nephrotoxic (toxic to the kidneys), however, the toxicity is sufficiently low that this is not expected to be a problem to otherwise healthy adults taking it at no more than the recommended dose.
For numbers, symptoms, and treatment, see this very clear and helpful resource:
An evidence based flowchart to guide the management of acute salicylate (aspirin) overdose
Take care!
Share This Post

Related Posts
-
Trouble getting out of bed? Signs the ‘winter blues’ may be something more serious
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Winter is here. As the days grow shorter and the skies turn darker, you might start to feel a bit “off”. You may notice a dip in your mood or energy levels. Maybe you’re less motivated to do things you previously enjoyed in the warmer months.
The “winter blues” can feel like an inevitable part of life. You might feel sluggish or less social, but you can still get on with your day.
However, if your winter blues are making everyday life difficult and interfering with your work and relationships, it could be the sign of something more serious.
Seasonal affective disorder is more than a seasonal slump – it’s a recognised psychiatric condition. Here’s what to look for and how to get help.
Justin Paget/Getty What is seasonal affective disorder?
The Diagnostic and Statistical Manual of Mental Disorders officially recognises seasonal affective disorder as a recurrent major depressive disorder “with seasonal pattern”.
In other words, the condition shares many symptoms with major depressive disorder, but it also follows a seasonal rhythm. While this might be most common in winter, the disorder can also occur in summer.
- persistent low mood or feelings of sadness
- loss of interest in activities you once enjoyed
- low energy and fatigue, even after lots of sleep
- changes in appetite
- weight gain or weight loss
- difficulty concentrating
- sleeping more or less than usual
- feelings of hopelessness or worthlessness
- in some cases, thoughts of self-harm or suicide.
Research suggests seasonal affective disorder affects up to 10% of the global population.
Although it can affect anyone, it is more common in women, people aged between 18 and 30 years, and those living far from the equator, where winter daylight hours are especially limited.
A review of the Australian research on seasonal affective disorder showed the highest proportion of Australians with seasonal affective disorder was found in the most southern state, Tasmania (9% of the population).
What causes it?
Unfortunately, the exact cause of seasonal affective disorder is still poorly understood.
Some theories propose it is primarily caused by a lack of light in the environment, although we are not exactly sure how this leads to depression.
As sunlight is responsible for the production of vitamin D, some have suggested a lack of vitamin D is what causes depression. However, the evidence for such a link is inconclusive.
Others suggest a lack of light in winter delays the circadian rhythms which regulate our sleep/wake cycle. Poor sleep is related to many mental health difficulties, including depression.
Seasonal affective disorder can be treated
Fortunately, there are several evidence-based treatments for seasonal affective disorder. Relief may be found through a combination of approaches.
Bright light therapy is usually the first treatment recommended for seasonal affective disorder. It involves sitting near a specially designed lightbox (with a strength of 10,000 lux) for about 20 to 30 minutes a day to mimic natural sunlight and help regulate the body’s internal clock.
Cognitive behavioural therapy aims to help people develop some flexibility around the negative thoughts that might maintain seasonal affective disorder symptoms (for example, “I am worthless because I never get up to anything meaningful in winter”).
Lifestyle changes such as regular exercise, time spent outdoors (even on gloomy days), a balanced diet, and good sleep hygiene can all support recovery.
Antidepressants – especially selective serotonin reuptake inhibitors (SSRIs) – may be prescribed when symptoms are moderate to severe, or when other treatments have not worked.
What else helps?
Even those without seasonal affective disorder might need to fight the winter blues. So, what works?
Prioritise social connection
Schedule regular, achievable and pleasant activities with friends, such as trivia at the pub or a brisk walk.
Reframe winter
Rather than dreading the cold, see if you can embrace what is special about this time of year. The mindset of “hygge” (a Danish and Norwegian term for cosiness and contentment) may help.
Let winter be your excuse for snuggling on your couch with a thick blanket and hot chocolate while catching up on books and TV shows. Or see if there are any winter-specific activities (such as night markets) where you live.
Maximise daylight
Taking a walk during lunchtime when the sun is out, even briefly, can make a difference.
The bottom line
If your “winter blues” last more than two weeks, start interfering with your daily life or feel overwhelming, then it might be time to seek professional help.
Speaking to your GP or mental health professional can help you get support early and prevent symptoms getting worse.
Kelvin (Shiu Fung) Wong, Senior Lecturer in Clinical Psychology, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Prozac’s Effect On Neuroplasticity
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Neuroplasticity is the brain’s ability to change over time, in accordance with our experiences, and what things we practise.
For example, before the ubiquity of GPS, taxi-drivers tended to get unusually well-developed in areas of the brain associated with memory and spatial reasoning. In contrast, your writer here, a person who does a lot of reading and writing and also uses at least 3+ languages daily, doubtlessly has overdeveloped language centers. A visual artist might develop much better visual centers. And so forth.
These changes are in large part physical, and very easy to measure (with the right equipment). It’s not hard to see when a certain part of the brain has proportionally more volume than usual, for example.
So, what does Prozac have to do with it?
More than a mood-brightener
Aside from the obvious primary intended effect of antidepressants (i.e., to treat depression by increasing relevant neurotransmitter levels), antidepressants have a bad reputation for side effects.
For example: How Serious Are Antidepressant Side Effects?
Some side effects are often exaggerated in popular (mis)understanding, such as: How Much Weight Gain Do Antidepressants Cause? ← the answer being: often less weight than people gain per year when not on antidepressants (although weight gain can happen, especially if one was previously under-eating while depressed)
When it comes to Prozac (the most well-known brand name for fluoxetine, a selective serotonin reuptake inhibitor (SSRI), which works by increasing serotonin levels in the brain by decreasing the rate at which the brain “loses” serotonin), it’s worth initially noting that while serotonin is mostly associated with happiness, it does other things too; see: Serotonin For More Than Just Happiness
The study we wrote about in that article found that it’s not just a matter of how much serotonin we have, but also where in the brain in accumulates, and which parts of the brain get prioritized. Sound familiar?
Recently, researchers (Dr. Ilida Suleymanova et al.) investigated the effects of serotonin on neuroplasticity, and found that indeed fluoxetine (Prozac) does more than boost serotonin—it also reshapes how certain brain cells manage energy and plasticity.
This happens as quickly as the first two weeks; for example, parvalbumin interneurons in the prefrontal cortex, which normally keep brain activity balanced, became less rigid after two weeks of treatment (which makes further changes much more possible), bearing in mind that since depression is linked to overly rigid brain circuits, this means that fluoxetine can “soften” these networks, allowing rewiring and flexibility.
- Specifically, mitochondria in these rigidity-inducing braincells got disempowered by reduced expression of energy-production genes (remember, people think of genes as unchangeable, but they can be turned on and off by hormones/neurotransmitters, amongst other things).
- Even more specifically, genes tied to adaptability were upregulated, and perineuronal nets that restrict plasticity were weakened.
To read this paper in full, see: Chronic treatment with fluoxetine regulates mitochondrial features and plasticity-associated transcriptomic pathways in parvalbumin-positive interneurons of prefrontal cortex
This becomes extra important as we age, because neurogenesis (the brain’s ability to produce new brain cells) is an important factor in neuroplasticity.
Contrary to popular belief, we continue to do this all the way through life, albeit it does usually slow down in older age, but there are things that affect how much this happens, and when.
To learn more about that, see: Building Your Brain At Every Age
Finally, if you’ve been considering antidepressants but haven’t been sure if they’d be right for you, then before you rush to your doctor to get a prescription for Prozac, you might want to check out: Antidepressants: Personalization Is Key! ← because it makes a difference which one you pick
Alternatively, if you don’t love the idea of having to keep taking something, you might consider: Psychedelics: Yes Even Once? ← since a single dose can have a lasting (positive!) effect on cognitive flexibility
Want to learn more?
You might like this book we reviewed a little while ago:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What Happens To Your Body When You Plank 1 Minute Every Day
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Planks improve strength, flexibility, balance, posture, reduce chronic back pain, lower blood pressure, and enhance physique. But can we really get benefits from just 1 minute per day?
To the core
The benefits that can be expected, according to the science cited in this video, include:
- Within 2–3 weeks, daily planking of just 1 minute per day activates deep core muscles, enhancing balance, which helps in everyday tasks and prevents muscle imbalances.
- Strengthening core muscles through planks also helps alleviate lower back pain, with research supporting its effectiveness within 3 weeks.
- Posture is important for good health, and planks align the spine and hips, improving posture naturally, which also helps alleviate back issues. So, there’s a good kind of synergy to this exercise.
- Of course, many people exercising have the goal of a more toned body; regular planking leads to a toned core, sculpted shoulders, and leaner legs.
- For those who care more about mobility, though, planking enhances flexibility in hamstrings, feet, and toes within 4–6 weeks.
- Anything else? Yes, isometric exercises like planks are highly effective at reducing blood pressure, and, counterintuitively, more so than aerobic exercises.
The video also looks at a study in which participants did 20 minutes per day instead of 1, which predictably also significantly improved strength, endurance, flexibility, and reduced body fat.
However, another study cited gives the stats for just 1 minute daily, and that was not even a whole minute, so much as 30 seconds hold, 1 minute rest, 30 seconds hold—and still showed very good improvements.
For more on all this, plus links to three studies mentioned in the video, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Isometric Exercises That Are Good If You Have Osteoporosis (or if you don’t, but the point is, they are safe and beneficial for people with osteoporosis)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: