High-Protein Plant-Based Diet for Beginners – by Maya Howard with Ariel Warren
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Seasoned vegans (well-seasoned vegans?) will know that getting enough protein from a plant-based diet is really not the challenge that many think it is, but for those just embarking on cutting out the meat, it’s not useful to say “it’s easy!”; it’s useful to show how.
That’s what this book does. And not just by saying “these foods” and leaving people to wonder if they need to eat a pound of tofu each day to get their protein in. Instead, recipes. Enough for a 4-week meal plan, and the idea is that after a month of eating that way, it won’t be nearly so mysterious.
The recipes are very easy to execute, while still having plenty of flavor (which is what happens when one uses a lot of flavorsome main ingredients and then seasons them well too). The ingredients are not obscure, and you should be able to find everything easily in any medium-sized supermarket.
As for the well-roundedness of the diet, we’ll mention that the “with Ariel Warren” in the by-line means that while the book was principally authored by Maya Howard (who is, at time of writing, a nutritionist-in-training), she had input throughout from Ariel Warren (a Registered Dietician Nutritionist) to ensure she didn’t go off-piste anyway and it gets the professional stamp of approval.
Bottom line: if you’d like to cook plant based while still prioritizing protein and you’re not sure how to make that exciting and fun instead of a chore, then this book will show you how to please your taste buds and improve your body composition at the same time.
Click here to check out High-Protein Plant-Based Diet for Beginners, and dig in!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Prolonged Grief: A New Mental Disorder?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The issue is not whether certain mental conditions are real—they are. It is how we conceptualize them and what we think treating them requires.
The latest edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) features a new diagnosis: prolonged grief disorder—used for those who, a year after a loss, still remain incapacitated by it. This addition follows more than a decade of debate. Supporters argued that the addition enables clinicians to provide much-needed help to those afflicted by what one might simply consider a too much of grief, whereas opponents insisted that one mustn’t unduly pathologize grief and reject an increasingly medicalized approach to a condition that they considered part of a normal process of dealing with loss—a process which in some simply takes longer than in others.
By including a condition in a professional classification system, we collectively recognize it as real. Recognizing hitherto unnamed conditions can help remove certain kinds of disadvantages. Miranda Fricker emphasizes this in her discussion of what she dubs hermeneutic injustice: a specific sort of epistemic injustice that affects persons in their capacity as knowers1. Creating terms like ‘post-natal depression’ and ‘sexual harassment’, Fricker argues, filled lacunae in the collectively available hermeneutic resources that existed where names for distinctive kinds of social experience should have been. The absence of such resources, Fricker holds, put those who suffered from such experiences at an epistemic disadvantage: they lacked the words to talk about them, understand them, and articulate how they were wronged. Simultaneously, such absences prevented wrong-doers from properly understanding and facing the harm they were inflicting—e.g. those who would ridicule or scold mothers of newborns for not being happier or those who would either actively engage in sexual harassment or (knowingly or not) support the societal structures that helped make it seem as if it was something women just had to put up with.
For Fricker, the hermeneutical disadvantage faced by those who suffer from an as-of-yet ill-understood and largely undiagnosed medical condition is not an epistemic injustice. Those so disadvantaged are not excluded from full participation in hermeneutic practices, or at least not through mechanisms of social coercion that arise due to some structural identity prejudice. They are not, in other words, hermeneutically marginalized, which for Fricker, is an essential characteristic of epistemic injustice. Instead, their situation is simply one of “circumstantial epistemic bad luck”2. Still, Fricker, too, can agree that providing labels for ill-understood conditions is valuable. Naming a condition helps raise awareness of it, makes it discursively available and, thus, a possible object of knowledge and understanding. This, in turn, can enable those afflicted by it to understand their experience and give those who care about them another way of nudging them into seeking help.
Surely, if adding prolonged grief disorder to the DSM-5 were merely a matter of recognizing the condition and of facilitating assistance, nobody should have any qualms with it. However, the addition also turns intense grief into a mental disorder—something for whose treatment insurance companies can be billed. With this, significant forces of interest enter the scene. The DSM-5, recall, is mainly consulted by psychiatrists. In contrast to talk-therapists like psychotherapists or psychoanalysts, psychiatrists constitute a highly medicalized profession, in which symptoms—clustered together as syndromes or disorders—are frequently taken to require drugs to treat them. Adding prolonged grief disorder thus heralds the advent of research into various drug-based grief therapies. Ellen Barry of the New York Times confirms this: “naltrexone, a drug used to help treat addiction,” she reports, “is currently in clinical trials as a form of grief therapy”, and we are likely to see a “competition for approval of medicines by the Food and Drug Administration.”3
Adding diagnoses to the DSM-5 creates financial incentives for players in the pharmaceutical industry to develop drugs advertised as providing relief to those so diagnosed. Surely, for various conditions, providing drug-induced relief from severe symptoms is useful, even necessary to enable patients to return to normal levels of functioning. But while drugs may help suppress feelings associated with intense grief, they cannot remove the grief. If all mental illnesses were brain diseases, they might be removed by adhering to some drug regimen or other. Note, however, that ‘mental illness’ is a metaphor that carries the implicit suggestion that just like physical illnesses, mental afflictions, too, are curable by providing the right kind of physical treatment. Unsurprisingly, this metaphor is embraced by those who stand to massively benefit from what profits they may reap from selling a plethora of drugs to those diagnosed with any of what seems like an ever-increasing number of mental disorders. But metaphors have limits. Lou Marinoff, a proponent of philosophical counselling, puts the point aptly:
Those who are dysfunctional by reason of physical illness entirely beyond their control—such as manic-depressives—are helped by medication. For handling that kind of problem, make your first stop a psychiatrist’s office. But if your problem is about identity or values or ethics, your worst bet is to let someone reify a mental illness and write a prescription. There is no pill that will make you find yourself, achieve your goals, or do the right thing.
Much more could be said about the differences between psychotherapy, psychiatry, and the newcomer in the field: philosophical counselling. Interested readers may benefit from consulting Marinoff’s work. Written in a provocative, sometimes alarmist style, it is both entertaining and—if taken with a substantial grain of salt—frequently insightful. My own view is this: from Fricker’s work, we can extract reasons to side with the proponents of adding prolonged grief disorder to the DSM-5. Creating hermeneutic resources that allow us to help raise awareness, promote understanding, and facilitate assistance is commendable. If the addition achieves that, we should welcome it. And yet, one may indeed worry that practitioners are too eager to move from the recognition of a mental condition to the implementation of therapeutic interventions that are based on the assumption that such afflictions must be understood on the model of physical disease. The issue is not whether certain mental conditions are real—they are. It is how we conceptualize them and what we think treating them requires.
No doubt, grief manifests physically. It is, however, not primarily a physical condition—let alone a brain disease. Grief is a distinctive mental condition. Apart from bouts of sadness, its symptoms typically include the loss of orientation or a sense of meaning. To overcome grief, we must come to terms with who we are or can be without the loved one’s physical presence in our life. We may need to reinvent ourselves, figure out how to be better again and whence to derive a new purpose. What is at stake is our sense of identity, our self-worth, and, ultimately, our happiness. Thinking that such issues are best addressed by popping pills puts us on a dangerous path, leading perhaps towards the kind of dystopian society Aldous Huxley imagined in his 1932 novel Brave New World. It does little to help us understand, let alone address, the moral and broader philosophical issues that trouble the bereaved and that lie at the root not just of prolonged grief but, arguably, of many so-called mental illnesses.
Footnotes:
1 For this and the following, cf. Fricker 2007, chapter 7.
2 Fricker 2007: 152
3 Barry 2022
References:
Barry, E. (2022). “How Long Should It Take to Grieve? Psychiatry Has Come Up With an Answer.” The New York Times, 03/18/2022, URL = https://www.nytimes.com/2022/03/18/health/prolonged-grief-
disorder.html [last access: 04/05/2022])
Fricker, M. (2007). Epistemic Injustice. Power & the Ethics of knowing. Oxford/New York: Oxford University Press.
Huxley, A. (1932). Brave New World. New York: Harper Brothers.
Marinoff, L. (1999). Plato, not Prozac! New York: HarperCollins Publishers.Professor Raja Rosenhagen is currently serving as Assistant Professor of Philosophy, Head of Department, and Associate Dean of Academic Affairs at Ashoka University. He earned his PhD in Philosophy from the University of Pittsburgh and has a broad range of philosophical interests (see here). He wrote this article a) because he was invited to do so and b) because he is currently nurturing a growing interest in philosophical counselling.
This article is republished from OpenAxis under a Creative Commons license. Read the original article.
Share This Post
-

The Biggest Cause Of Back Pain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Will Harlow, specialist over-50s physiotherapist, shares the most common cause (and its remedy) in this video:
The seat of the problem
The issue (for most people, anyway) is not in the back itself, nor the core in general, but rather, in the glutes. That is to say: the gluteus maximus, medius, and minimus. They assist in bending forwards (collaborating half-and-half with your back muscles), and help control pelvic alignment while walking.
Sitting for long periods weakens the glutes, causing the back to overcompensate, leading to pain. So, obviously don’t do that, if you can help it. Weak glutes shift the work to your back muscles during bending and walking, increasing strain and—as a result—back pain.
The solution (besides “sit less”) is to do specific exercises to strengthen the glutes. When you do, focus on good form and do not try to push through pain. If the exercises themselves all cause pain, then stop and consult a local physiotherapist to figure out your next step.
With that in mind, the five exercises recommended in this video to strengthen glutes and reduce back pain are:
- Hip abduction (isometric): use a heavy resistance band or belt around legs above the knees, push outwards.
- The clam: lie on your side, bend your knees 90°, and lift your top knee while keeping your body forward. Focus on glute engagement.
- Clam with resistance band: use a light resistance band above your knees and perform the same clam exercise.
- Hip abduction (straight leg): lie on your side, keep legs straight, lift your top leg diagonally backward. Lead with your heel to target your glutes and avoid back strain.
- Hip abduction with resistance band: place a resistance band around your ankles, and lift leg as in the previous exercise.
For more on all these, plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- 6 Ways To Look After Your Back
- Strong Curves: A Woman’s Guide To Building A Better Butt And Body – by Bret Contreras & Kellie Davis
- How To Stop Pain From Spreading
Take care!
Share This Post
-

Loving Life at 50+ – by Maria Sabando
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What a pleasant mix of a book! Sabando writes about aging with a great blend of light-heartedness and seriousness, and gives extra attention to the important balancing act of:
- Indulging sufficiently to enjoy life
- Staying well enough to enjoy life
…because one without the other will not generally result in an enjoyable life! An American proud of her Italian heritage, she blends (as many immigrant families do) cultures and perspectives, aiming where she can for “the best of both” in that regard, too.
Nor is this just a philosophical book—there’s yoga to be learned here, chapter by chapter, and recipes peppered throughout. The recipes, by the way, are simple and… Honestly, not as healthy as the recipes we share here at 10almonds, but they are good and when it comes to those indulgences we mentioned, her philosophy is that strategic mindful indulgence keeps mindless binge-eating at bay. Which is generally speaking not a bad approach, and is one we’ve written about before as well.
When it comes to health advice, the author is no doctor or scientist, but her husband (a doctor) had input throughout, keeping things on track and medically sound.
The style is very casual, like talking to a friend, which makes for a very easy and enjoyable read. Absolutely a book that one could read casually in the garden, put down when interrupted, pick up again, and continue happily where one left off.
Bottom line: whatever your age (no matter whether your 50th birthday is in your shrinkingly near future or your increasingly distant past), there’s wisdom to be gained here—it’s not a manual (unless you want to treat it as one), it’s more… Thought-provoking, from cover to cover. Highly recommendable.
Click here to check out Loving Life at 50+, and love life at 50+!
Share This Post
Related Posts
-

Addiction Myths That Are Hard To Quit
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Which Addiction-Quitting Methods Work Best?

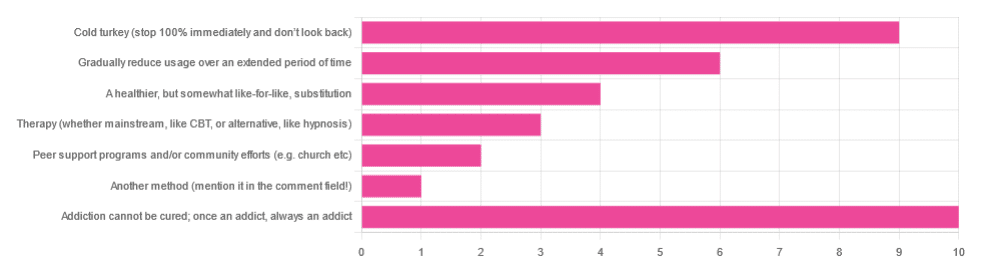
In Tuesday’s newsletter we asked you what, in your opinion, is the best way to cure an addiction. We got the above-depicted, below-described, interesting distribution of responses:
- About 29% said: “Addiction cannot be cured; once an addict, always an addict”
- About 26% said “Cold turkey (stop 100% and don’t look back)”
- About 17% said “Gradually reduce usage over an extended period of time”
- About 11% said “A healthier, but somewhat like-for-like, substitution”
- About 9% said “Therapy (whether mainstream, like CBT, or alternative, like hypnosis)”
- About 6% said “Peer support programs and/or community efforts (e.g. church etc)”
- About 3% said “Another method (mention it in the comment field)” and then did not mention it in the comment field
So what does the science say?
Addiction cannot be cured; once an addict, always an addict: True or False?
False, which some of the people who voted for it seemed to know, as some went on to add in the comment field what they thought was the best way to overcome the addiction.
The widespread belief that “once an addict, always an addict” is a “popular truism” in the same sense as “once a cheater, always a cheater”. It’s an observation of behavioral probability phrased as a strong generalization, but it’s not actually any kind of special unbreakable law of the universe.
And, certainly the notion that one cannot be cured keeps membership in many 12-step programs and similar going—because if you’re never cured, then you need to stick around.
However…
❝What is the definition of addiction?
Addiction is a treatable, chronic medical disease involving complex interactions among brain circuits, genetics, the environment, and an individual’s life experiences. People with addiction use substances or engage in behaviors that become compulsive and often continue despite harmful consequences.
Prevention efforts and treatment approaches for addiction are generally as successful as those for other chronic diseases.❞
~ American Society of Addiction Medicine
Or if we want peer-reviewed source science, rather than appeal to mere authority as above, then:
❝What is drug addiction?
Addiction is defined as a chronic, relapsing disorder characterized by compulsive drug seeking and use despite adverse consequences. It is considered a brain disorder, because it involves functional changes to brain circuits involved in reward, stress, and self-control. Those changes may last a long time after a person has stopped taking drugs.
Addiction is a lot like other diseases, such as heart disease. Both disrupt the normal, healthy functioning of an organ in the body, both have serious harmful effects, and both are, in many cases, preventable and treatable.❞
~ Nora D. Volkow (Director, National Institute of Drug Abuse)
Read more: Drugs, Brains, and Behavior: The Science of Addiction
In short: part of the definition of addiction is the continued use; if the effects of the substance are no longer active in your physiology, and you are no longer using, then you are not addicted.
Just because you would probably become addicted again if you used again does not make you addicted when neither the substance nor its after-effects are remaining in your body. Otherwise, we could define all people as addicted to all things based on “well if they use in the future they will probably become addicted”.
This means: the effects of addiction can and often will last for long after cessation of use, but ultimately, addiction can be treated and cured.
(yes, you should still abstain from the thing to which you were formerly addicted though, or you indeed most probably will become addicted again)
Cold turkey is best: True or False?
True if and only if certain conditions are met, and then only for certain addictions. For all other situations… False.
To decide whether cold turkey is a safe approach (before even considering “effective”), the first thing to check is how dangerous the withdrawal symptoms are. In some cases (e.g. alcohol, cocaine, heroin, and others), the withdrawal symptoms can kill.
That doesn’t mean they will kill, so knowing (or being!) someone who quit this way does not refute this science by counterexample. The mortality rates that we saw while researching varied from 8% to 37%, so most people did not die, but do you really want (yourself or a loved one) to play those odds unnecessarily?
See also: Detoxification and Substance Abuse Treatment
Even in those cases where it is considered completely safe for most people to quit cold turkey, such as smoking, it is only effective when the quitter has appropriate reliable medical support, e.g.
- Without support: 3–5% success rate
- With support: 22% success rate
And yes, that 22% was for the “abrupt cessation” group; the “gradual cessation” group had a success rate of 15.5%. On which note…
Gradual reduction is the best approach: True or False?
False based on the above data, in the case of addictions where abrupt cessation is safe. True in other cases where abrupt cessation is not safe.
Because if you quit abruptly and then die from the withdrawal symptoms, then well, technically you did stay off the substance for the rest of your life, but we can’t really claim that as a success!
A healthier, but somewhat like-for-like substitution is best: True or False?
True where such is possible!
This is why, for example, medical institutions recommend the use of buprenorphine (e.g. Naloxone) in the case of opioid addiction. It’s a partial opioid receptor agonist, meaning it does some of the job of opioids, while being less dangerous:
It’s also why vaping—despite itself being a health hazard—is recommended as a method of quitting smoking:
Similarly, “zero alcohol drinks that seem like alcohol” are a popular way to stop drinking alcohol, alongside other methods:
This is also why it’s recommended that if you have multiple addictions, to quit one thing at a time, unless for example multiple doctors are telling you otherwise for some specific-to-your-situation reason.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The Painkilling Power Of Opioids, Without The Harm?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to painkilling medications, they can generally be categorized into two kinds:
- non-opioids (e.g. ibuprofen, paracetamol/acetaminophen, aspirin)
- ones that actually work for something more serious than a headache
That’s an oversimplification, but broadly speaking, when there is serious painkilling to be done, that’s when doctors consider it’s time to break out the opioids.
Nor are all opioids created equal—there’s a noteworthy difference between codeine and morphine, for instance—but the problems of opioids are typically the same (tolerance, addiction, and eventual likelihood of overdose when one tries to take enough to make it work after developing a tolerance), and it becomes simply a matter of degree.
See also: I’ve been given opioids after surgery to take at home. What do I need to know?
So, what’s the new development?
A team of researchers have found that the body can effectively produce its own targetted painkilling peptides, similar in function to benzodiazepines (an opioid drug), but—and which is a big difference—confined to the peripheral nervous system (PNS), meaning that it doesn’t enter the brain.
- The peptides killing the pain before it can reach the brain is obviously good because that means the pain is simply not experienced
- The peptides not having any effect on the brain, however, means that the mechanism of addiction of opioids simply does not apply here
- The peptides not having any effect on the brain also means that the CNS can’t be “put to sleep” by these peptides in the same way it can if a high dose of opioids is taken (this is what typically causes death in opioid overdoses; the heart simply beats too slowly to maintain life)
The hope, therefore, is to now create medications that target the spinal ganglia that produce these peptides, to “switch them on” at will.
Obviously, this won’t happen overnight; there will need to be first a lot of research to find a drug that does that (likely this will involve a lot of trial and error and so many mice/rats), and then multiple rounds of testing to ascertain that the drug is safe and effective for humans, before it can then be rolled out commercially.
But, this is still a big breakthrough; there arguably hasn’t been a breakthrough this big in pain research since various opioid-related breakthroughs in the 70s and 80s.
You can see a pop-science article about it here:
And you can see the previous research (from earlier this year) that this is now building from, about the glial cells in the spinal ganglia, here:
Peripheral gating of mechanosensation by glial diazepam binding inhibitor
But wait, there’s more!
Remember what we said about affecting the PNS without affecting the CNS, to kill the pain without killing the brain?
More researchers are already approaching the same idea to deal with the same problem, but from the angle of gene therapy, and have already had some very promising results with mice:
Structure-guided design of a peripherally restricted chemogenetic system
…which you can read about in pop-science terms (with diagrams!) here:
New gene therapy could alleviate chronic pain, researchers find
While you’re waiting…
In the meantime, approaches that are already available include:
- The 7 Approaches To Pain Management
- Managing Chronic Pain (Realistically!)
- Science-Based Alternative Pain Relief ← when painkillers aren’t helping, these things might!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How to test for STIs at home
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What you need to know
- Anyone can contract an STI through sexual activity involving the mouth, genitals, or anus. Regular testing is important since many STIs can be treated with medication, but untreated STIs can lead to serious complications.
- The Food and Drug Administration has approved at-home STI tests for HIV, syphilis, chlamydia, gonorrhea, trichomoniasis, and HPV.
- You can get at-home STI test kits online and at some pharmacies, health clinics, and health departments depending on where you live. Most test providers will get you your results within a week.
This year, federal budget cuts are forcing many Planned Parenthood health centers to close. As some communities lose access to local sexual health services, at-home testing for STIs makes getting a diagnosis more accessible, which supports treatment and limits infection spread.
Read on to learn how to test for STIs at home, what to do if you get a positive test result, and more.
What are STIs?
STIs—sometimes called sexually transmitted diseases or STDs—are infections that anyone can contract through sexual activity involving the mouth, genitals, or anus. They can be caused by bacteria, viruses, or parasites.
Some common STI symptoms include:
- Bumps, sores, or warts on or near the genitals, mouth, or anus.
- Swelling, pain, or itching on or near the genitals.
- Painful or frequent urination.
- Genital discharge, bleeding, or odor.
Many STIs are easily treated with medication. However, if left untreated or unmanaged, some can cause long-term and even deadly complications.
Some STIs won’t cause symptoms, but they can lead to complications later on.
Which STIs can I test for at home?
Many at-home STI tests are available, and while experts believe that most tests provide accurate results, only a few are approved by the FDA.
The FDA has approved at-home tests for syphilis and for HIV that anyone can use. An FDA-approved, at-home vaginal swab for chlamydia, gonorrhea, and trichomoniasis is also available. Currently, any California resident with a cervix between ages 25 and 65 can also test for HPV (human papillomavirus) at home using the FDA-approved Teal Wand, which is expected to be available nationwide next year.
Who should consider at-home STI tests?
Testing for STIs at home may be right for you if you are unable to go to a doctor’s office or health clinic that offers sexual health services or if you feel more comfortable testing yourself in a private space.
Even if you take an at-home test, you may need to schedule an appointment with a health care provider for treatment and prevention recommendations.
At-home STI tests are “a great way to expand our reach of sexual health services to patient populations that have a hard time getting to sexual clinical services, but they don’t stand alone,” said Dr. Robert A. Pitts, an infectious disease specialist at NYU Langone Health, in an April New York Times article.
Free or low-cost STI tests are still available through local community health centers and public health clinics. Find a location near you through the Centers for Disease Control and Prevention’s GetTested site.
How do I test for STIs at home, and when will I get my results?
At-home STI testing typically involves collecting a sample of a bodily fluid and mailing it to a lab. Your test instructions may direct you to urinate in a sealable cup, prick your finger to get a drop of blood, or swab your mouth, genitals, or anus.
Most test kits include a prepaid envelope addressed to a lab so that you can mail in your samples.
Check with your test kit provider to find out when you can expect your results. Most kits provide results through an online portal within a week. However, if you’re using an at-home rapid HIV test, you’ll see your result in about 20 minutes.
Where can I get at-home STI tests?
You can purchase at-home STI tests without a prescription at some pharmacies. Many are also available online.
You may also be able to pick up at-home test kits from your local health clinic or health department.
How much do at-home STI tests cost?
Without insurance, the price of at-home STI test kits can range from $10 to $250. Health clinics may provide free or low-cost kits for low-income individuals.
Some health insurance plans cover at-home STIs tests. Contact your insurance to learn more.
Together TakeMeHome offers free at-home HIV test kits via mail for anyone 17 and older living in the U.S., including Puerto Rico. Some state-specific programs also offer free at-home STI tests.
What should I do if I get a positive test result?
If you receive a positive test result, see a health care provider right away for treatment. Remember that it can take days or even months for some STIs to show up on a test, so even if your tests are negative, retesting regularly is recommended, even if you don’t have new sexual partners.
Talk to your health care provider for more information and to find out how often you should test for STIs.
This article first appeared on Public Good News and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: