I’ve been given opioids after surgery to take at home. What do I need to know?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Opioids are commonly prescribed when you’re discharged from hospital after surgery to help manage pain at home.
These strong painkillers may have unwanted side effects or harms, such as constipation, drowsiness or the risk of dependence.
However, there are steps you can take to minimise those harms and use opioids more safely as you recover from surgery.

Which types of opioids are most common?
The most commonly prescribed opioids after surgery in Australia are oxycodone (brand names include Endone, OxyNorm) and tapentadol (Palexia).
In fact, about half of new oxycodone prescriptions in Australia occur after a recent hospital visit.
Most commonly, people will be given immediate-release opioids for their pain. These are quick-acting and are used to manage short-term pain.
Because they work quickly, their dose can be easily adjusted to manage current pain levels. Your doctor will provide instructions on how to adjust the dosage based on your pain levels.
Then there are slow-release opioids, which are specially formulated to slowly release the dose over about half to a full day. These may have “sustained-release”, “controlled-release” or “extended-release” on the box.
Slow-release formulations are primarily used for chronic or long-term pain. The slow-release form means the medicine does not have to be taken as often. However, it takes longer to have an effect compared with immediate-release, so it is not commonly used after surgery.
Controlling your pain after surgery is important. This allows you get up and start moving sooner, and recover faster. Moving around sooner after surgery prevents muscle wasting and harms associated with immobility, such as bed sores and blood clots.
Everyone’s pain levels and needs for pain medicines are different. Pain levels also decrease as your surgical wound heals, so you may need to take less of your medicine as you recover.
But there are also risks
As mentioned above, side effects of opioids include constipation and feeling drowsy or nauseous. The drowsiness can also make you more likely to fall over.
Opioids prescribed to manage pain at home after surgery are usually prescribed for short-term use.
But up to one in ten Australians still take them up to four months after surgery. One study found people didn’t know how to safely stop taking opioids.
Such long-term opioid use may lead to dependence and overdose. It can also reduce the medicine’s effectiveness. That’s because your body becomes used to the opioid and needs more of it to have the same effect.
Dependency and side effects are also more common with slow-release opioids than immediate-release opioids. This is because people are usually on slow-release opioids for longer.
Then there are concerns about “leftover” opioids. One study found 40% of participants were prescribed more than twice the amount they needed.
This results in unused opioids at home, which can be dangerous to the person and their family. Storing leftover opioids at home increases the risk of taking too much, sharing with others inappropriately, and using without doctor supervision.

How to mimimise the risks
Before using opioids, speak to your doctor or pharmacist about using over-the-counter pain medicines such as paracetamol or anti-inflammatories such as ibuprofen (for example, Nurofen, Brufen) or diclofenac (for example, Voltaren, Fenac).
These can be quite effective at controlling pain and will lessen your need for opioids. They can often be used instead of opioids, but in some cases a combination of both is needed.
Other techniques to manage pain include physiotherapy, exercise, heat packs or ice packs. Speak to your doctor or pharmacist to discuss which techniques would benefit you the most.
However, if you do need opioids, there are some ways to make sure you use them safely and effectively:
- ask for immediate-release rather than slow-release opioids to lower your risk of side effects
- do not drink alcohol or take sleeping tablets while on opioids. This can increase any drowsiness, and lead to reduced alertness and slower breathing
- as you may be at higher risk of falls, remove trip hazards from your home and make sure you can safely get up off the sofa or bed and to the bathroom or kitchen
- before starting opioids, have a plan in place with your doctor or pharmacist about how and when to stop taking them. Opioids after surgery are ideally taken at the lowest possible dose for the shortest length of time.

If you’re concerned about side effects
If you are concerned about side effects while taking opioids, speak to your pharmacist or doctor. Side effects include:
- constipation – your pharmacist will be able to give you lifestyle advice and recommend laxatives
- drowsiness – do not drive or operate heavy machinery. If you’re trying to stay awake during the day, but keep falling asleep, your dose may be too high and you should contact your doctor
- weakness and slowed breathing – this may be a sign of a more serious side effect such as respiratory depression which requires medical attention. Contact your doctor immediately.
If you’re having trouble stopping opioids
Talk to your doctor or pharmacist if you’re having trouble stopping opioids. They can give you alternatives to manage the pain and provide advice on gradually lowering your dose.
You may experience withdrawal effects, such as agitation, anxiety and insomnia, but your doctor and pharmacist can help you manage these.
How about leftover opioids?
After you have finished using opioids, take any leftovers to your local pharmacy to dispose of them safely, free of charge.
Do not share opioids with others and keep them away from others in the house who do not need them, as opioids can cause unintended harms if not used under the supervision of a medical professional. This could include accidental ingestion by children.
For more information, speak to your pharmacist or doctor. Choosing Wisely Australia also has free online information about managing pain and opioid medicines.
Katelyn Jauregui, PhD Candidate and Clinical Pharmacist, School of Pharmacy, Faculty of Medicine and Health, University of Sydney; Asad Patanwala, Professor, Sydney School of Pharmacy, University of Sydney; Jonathan Penm, Senior lecturer, School of Pharmacy, University of Sydney, and Shania Liu, Postdoctoral Research Fellow, Faculty of Medicine and Dentistry, University of Alberta
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The 7 Approaches To Pain Management

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
More Than One Way To Kill Pain

This is Dr. Deepak Ravindran (MD, FRCA. FFPMRCA, EDRA. FIPP, DMSMed). He has decades of experience and is a specialist in acute and chronic pain management, anesthesia, musculoskeletal medicine, and lifestyle medicine.
A quick catch-up, first:
We’ve written about chronic pain management before:
Managing Chronic Pain (Realistically!)
As well as:
Science-Based Alternative Pain Relief
Dr. Ravindran’s approach
Dr. Ravindran takes a “trauma-informed care” approach to his professional practice, and recommends the same for others.
In a nutshell, this means starting from a position of not “what’s wrong with you?”, but rather “what happened to you?”.
This seemingly subtle shift is important, because it means actually dealing with a person’s issues, instead of “take one of these and call my secretary next month”. Read more:
Pain itself can be something of a many-headed hydra. Dr. Ravindran’s approach is equally many-headed; specifically, he has a 7-point plan:
Medications
Dr. Ravindran sees painkillers (and a collection of other drugs, like antidepressants and muscle relaxants) as a potential means to an end worth exploring, but he doesn’t expect them to be the best choice for everyone, and nor does he expect them to be a cure-all. Neither should we. He also advises being mindful of the drawbacks and potential complications of these drugs, too.
Interventions
Sometimes, surgery is the right choice. Sometimes it isn’t. Often, it will change a life—one way or the other. Similar to with medications, Dr. Ravindran is very averse to a “one size fits all” approach here. See also:
The Insider’s Guide To Making Hospital As Comfortable As Possible
Neuroscience and stress management
Often a lot of the distress of pain is not just the pain itself, but the fear associated with it. Will it get worse if I move wrong or eat the wrong thing? How long will it last? Will it ever get better? Will it get worse if I do nothing?. Dr. Ravindran advises tackling this, with the same level of importance as the pain itself. Here’s a good start:
Stress, And Building Psychological Resilience
Diet and the microbiome
Many chronic illnesses are heavily influenced by this, and Dr. Ravindran’s respect for lifestyle medicine comes into play here. While diet might not fix all our ills, it certainly can stop things from being a lot worse. Beyond the obvious “eat healthily” (Mediterranean diet being a good starting point for most people), he also advises doing elimination tests where appropriate, to screen out potential flare-up triggers. You also might consider:
Four Ways To Upgrade The Mediterranean Diet
Sleep
“Get good sleep” is easy advice for those who are not in agonizing pain that sometimes gets worse from staying in the same position for too long. Nevertheless, it is important, and foundational to good health. So it’s important to explore—whatever limitations one might realistically have—what can be done to improve it.
If you can only sleep for a short while at a time, you may get benefit from this previous main feature of ours:
How To Nap Like A Pro (No More “Sleep Hangovers”!)
Exercise and movement
The trick here is to move little and often; without overdoing it, but without permitting loss of mobility either. See also:
The Doctor Who Wants Us To Exercise Less, And Move More
Therapies of the mind and body
This is about taking a holistic approach to one’s wellness. In Dr. Ravindran’s words:
❝Mind-body therapies are often an extremely sensitive topic about which people hold very strong opinions and sometimes irrational beliefs.
Some, like reiki and spiritual therapy and homeopathy, have hardly any scientific evidence to back them up, while others like yoga, hypnosis, and meditation/mindfulness are mainstream techniques with many studies showing the benefits, but they all work for certain patients.❞
In other words: evidence-based is surely the best starting point, but if you feel inclined to try something else and it works for you, then it works for you. And that’s a win.
Want to know more?
You might like his book…
The Pain-Free Mindset: 7 Steps to Taking Control and Overcoming Chronic Pain
He also has a blog and a podcast.
Take care!
Share This Post
-

Gluten Sensitivity May Not Be About The Gluten
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to understanding of how gluten affects different people’s bodies, there’s a lot that’s not well-understood.
By this we mean: there’s a lot that’s not well-understood by science, and there’s even more that’s not well-understood by people in general.
We did some demystification, covering such things as celiac disease and the differences between an allergy, intolerance, and sensitivity, here:
And now…
A new culprit arises
Well, actually a moderately well-known culprit, just, not usually associated with this.
Researchers (Dr. Jessica Biesiekierski et al.) found that non-celiac gluten sensitivity (NCGS) appears to be driven by gut–brain interactions rather than gluten itself.
You may be thinking: “yes, but the gut is reacting to the gluten, right?”
A very reasonable assumption! And the answer is: no
As Dr. Biesiekierski put it:
❝Contrary to popular belief, most people with NCGS aren’t reacting to gluten. Our findings show that symptoms are more often triggered by fermentable carbohydrates, commonly known as FODMAPs, by other wheat components or by people’s expectations and prior experiences with food.❞
As for how she and her team figured this out, they did the largest combined analysis of its kind that’s ever been done on this topic, and found:
❝Across recent studies, people with IBS who believe they’re gluten-sensitive react similarly to gluten, wheat, and placebo.
This suggests that how people anticipate and interpret gut sensations can strongly influence their symptoms.
Taken together, this redefines NCGS as part of the gut–brain interaction spectrum, closer to conditions like irritable bowel syndrome, rather than a distinct gluten disorder.❞
You can find the paper itself, here: Non-coeliac gluten sensitivity ← where you can also read the insights of Dr. Daisy Jonkers and other researchers!
If you do want to avoid FODMAPs while still getting enough other important plant nutrients, see: Fruit, Fiber, & Leafy Greens… On A Low-FODMAP Diet!
So, with this in mind, one might wonder: is there any harm in going gluten-free as well just to be on the safe side?
And yes, there may be issues! See: Why Going Gluten-Free Could Be A Bad Idea
And as for grains in general (for most people) enjoying whole grains remains a very good idea:
3 servings (each being 90g, or about ½ cup) of whole grains per day is associated with a 22% reduction in risk of heart disease, 5% reduction in all-cause mortality, and a lot of benefits across a lot of other disease risks:
❝This meta-analysis provides further evidence that whole grain intake is associated with a reduced risk of coronary heart disease, cardiovascular disease, and total cancer, and mortality from all causes, respiratory diseases, infectious diseases, diabetes, and all non-cardiovascular, non-cancer causes.
These findings support dietary guidelines that recommend increased intake of whole grain to reduce the risk of chronic diseases and premature mortality.❞
~ Dr. Dagfinn Aune et al.
We’d like to give a lot more sources for the same findings, as well as papers for all the individual claims, but frankly, there are so many that there isn’t room. Suffice it to say, this is neither controversial nor uncertain; these benefits are well-established.
Want to learn more?
Here’s a guest article written by none other than Dr. Jessica Biesiekierski, the lead researcher on the first study we linked today:
Your gluten sensitivity might be something else entirely, new study shows
Take care!
Share This Post
-

How Does One Test Acupuncture Against Placebo Anyway?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Pinpointing The Usefulness Of Acupuncture

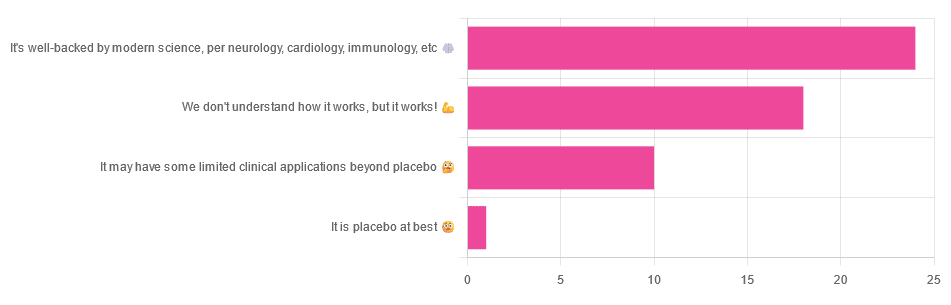
We asked you for your opinions on acupuncture, and got the above-depicted, below-described, set of answers:
- A little under half of all respondents voted for “It’s well-backed by modern science, per neurology, cardiology, immunology, etc”
- Slightly fewer respondents voted for “We don’t understand how it works, but it works!”
- A little under a fifth of respondents voted for “It may have some limited clinical applications beyond placebo”
- One (1) respondent voted for for “It’s placebo at best”
When we did a main feature about homeopathy, a couple of subscribers wrote to say that they were confused as to what homeopathy was, so this time, we’ll start with a quick definition first.
First, what is acupuncture? For the convenience of a quick definition so that we can move on to the science, let’s borrow from Wikipedia:
❝Acupuncture is a form of alternative medicine and a component of traditional Chinese medicine in which thin needles are inserted into the body.
Acupuncture is a pseudoscience; the theories and practices of TCM are not based on scientific knowledge, and it has been characterized as quackery.❞
Now, that’s not a promising start, but we will not be deterred! We will instead examine the science itself, rather than relying on tertiary sources like Wikipedia.
It’s worth noting before we move on, however, that there is vigorous debate behind the scenes of that article. The gist of the argument is:
- On one side: “Acupuncture is not pseudoscience/quackery! This has long been disproved and there are peer-reviewed research papers on the subject.”
- On the other: “Yes, but only in disreputable quack journals created specifically for that purpose”
The latter counterclaim is a) potentially a “no true Scotsman” rhetorical ploy b) potentially true regardless
Some counterclaims exhibit specific sinophobia, per “if the source is Chinese, don’t believe it”. That’s not helpful either.
Well, the waters sure are muddy. Where to begin? Let’s start with a relatively easy one:
It may have some clinical applications beyond placebo: True or False?
True! Admittedly, “may” is doing some of the heavy lifting here, but we’ll take what we can get to get us going.
One of the least controversial uses of acupuncture is to alleviate chronic pain. Dr. Vickers et al, in a study published under the auspices of JAMA (a very respectable journal, and based in the US, not China), found:
❝Acupuncture is effective for the treatment of chronic pain and is therefore a reasonable referral option. Significant differences between true and sham acupuncture indicate that acupuncture is more than a placebo.
However, these differences are relatively modest, suggesting that factors in addition to the specific effects of needling are important contributors to the therapeutic effects of acupuncture❞
Source: Acupuncture for Chronic Pain: Individual Patient Data Meta-analysis
If you’re feeling sharp today, you may be wondering how the differences are described as “significant” and “relatively modest” in the same text. That’s because these words have different meanings in academic literature:
- Significant = p<0.05, where p is the probability of the achieved results occurring randomly
- Modest = the differences between the test group and the control group were small
In other words, “significant modest differences” means “the sample sizes were large, and the test group reliably got slightly better results than placebo”
We don’t understand how it works, but it works: True or False
Broadly False. When it works, we generally have an idea how.
Placebo is, of course, the main explanation. And even in examples such as the above, how is placebo acupuncture given?
By inserting acupuncture needles off-target rather than in accord with established meridians and points (the lines and dots that, per Traditional Chinese Medicine, indicate the flow of qi, our body’s vital energy, and welling-points of such).
So, if a patient feels that needles are being inserted randomly, they may no longer have the same confidence that they aren’t in the control group receiving placebo, which could explain the “modest” difference, without there being anything “to” acupuncture beyond placebo. After all, placebo works less well if you believe you are only receiving placebo!
Indeed, a (Korean, for the record) group of researchers wrote about this—and how this confounding factor cuts both ways:
❝Given the current research evidence that sham acupuncture can exert not only the originally expected non-specific effects but also sham acupuncture-specific effects, it would be misleading to simply regard sham acupuncture as the same as placebo.
Therefore, researchers should be cautious when using the term sham acupuncture in clinical investigations.❞
Source: Sham Acupuncture Is Not Just a Placebo
It’s well-backed by modern science, per neurology, cardiology, immunology, etc: True or False?
False, for the most part.
While yes, the meridians and points of acupuncture charts broadly correspond to nerves and vasculature, there is no evidence that inserting needles into those points does anything for one’s qi, itself a concept that has not made it into Western science—as a unified concept, anyway…
Note that our bodies are indeed full of energy. Electrical energy in our nerves, chemical energy in every living cell, kinetic energy in all our moving parts. Even, to stretch the point a bit, gravitational potential energy based on our mass.
All of these things could broadly be described as qi, if we so wish. Indeed, the ki in the Japanese martial art of aikido is the latter kinds; kinetic energy and gravitational potential energy based on our mass. Same goes, therefore for the ki in kiatsu, a kind of Japanese massage, while the ki in reiki, a Japanese spiritual healing practice, is rather more mystical.
The qi in Chinese qigong is mostly about oxygen, thus indirectly chemical energy, and the electrical energy of the nerves that are receiving oxygenated blood at higher or lower levels.
On the other hand, the efficacy of the use of acupuncture for various kinds of pain is well-enough evidenced. Indeed, even the UK’s famously thrifty NHS (that certainly would not spend money on something it did not find to work) offers it as a complementary therapy for some kinds of pain:
❝Western medical acupuncture (dry needling) is the use of acupuncture following a medical diagnosis. It involves stimulating sensory nerves under the skin and in the muscles.
This results in the body producing natural substances, such as pain-relieving endorphins. It’s likely that these naturally released substances are responsible for the beneficial effects experienced with acupuncture.❞
Source: NHS | Acupuncture
Meanwhile, the NIH’s National Cancer Institute recommends it… But not as a cancer treatment.
Rather, they recommend it as a complementary therapy for pain management, and also against nausea, for which there is also evidence that it can help.
Frustratingly, while they mention that there is lots of evidence for this, they don’t actually link the studies they’re citing, or give enough information to find them. Instead, they say things like “seven randomized clinical trials found that…” and provide links that look reassuring until one finds, upon clicking on them, that it’s just a link to the definition of “randomized clinical trial”:
Source: NIH | Nactional Cancer Institute | Acupuncture (PDQ®)–Patient Version
However, doing our own searches finds many studies (mostly in specialized, potentially biased, journals such as the Journal of Acupuncture and Meridian Studies) finding significant modest outperformance of [what passes for] placebo.
Sometimes, the existence of papers with promising titles, and statements of how acupuncture might work for things other than relief of pain and nausea, hides the fact that the papers themselves do not, in fact, contain any evidence to support the hypothesis. Here’s an example:
❝The underlying mechanisms behind the benefits of acupuncture may be linked with the regulation of the hypothalamic-pituitary-gonadal (adrenal) axis and activation of the Wnt/β-catenin and OPG/RANKL/RANK signaling pathways.
In summary, strong evidence may still come from prospective and well-designed clinical trials to shed light on the potential role of acupuncture in preserving bone loss❞
Source: Acupuncture for Osteoporosis: a Review of Its Clinical and Preclinical Studies
So, here they offered a very sciencey hypothesis, and to support that hypothesis, “strong evidence may still come”.
“We must keep faith” is not usually considered evidence worthy of inclusion in a paper!
PS: the above link is just to the abstract, because the “Full Text” link offered in that abstract leads to a completely unrelated article about HIV/AIDS-related cryptococcosis, in a completely different journal, nothing to do with acupuncture or osteoporosis).
Again, this is not the kind of professionalism we expect from peer-reviewed academic journals.
Bottom line:
Acupuncture reliably performs slightly better than sham acupuncture for the management of pain, and may also help against nausea.
Beyond placebo and the stimulation of endorphin release, there is no consistently reliable evidence that is has any other discernible medical effect by any mechanism known to Western science—though there are plenty of hypotheses.
That said, absence of evidence is not evidence of absence, and the logistical difficulty of testing acupuncture against placebo makes for slow research. Maybe one day we’ll know more.
For now:
- If you find it helps you: great! Enjoy
- If you think it might help you: try it! By a licensed professional with a good reputation, please.
- If you are not inclined to having needles put in you unnecessarily: skip it! Extant science suggests that at worst, you’ll be missing out on slight relief of pain/nausea.
Take care!
Share This Post


Related Posts
-
Scrolling on the toilet increases your risk of haemorrhoids, new study shows
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many of us are guilty of scrolling our smartphones on the toilet. But a new study from the United States, published today, has found this habit may increase your risk of developing haemorrhoids by up to 46%.
So, what’s the link? How can time on your phone lead to these painful lumps in and around your anus? Here’s what we know.

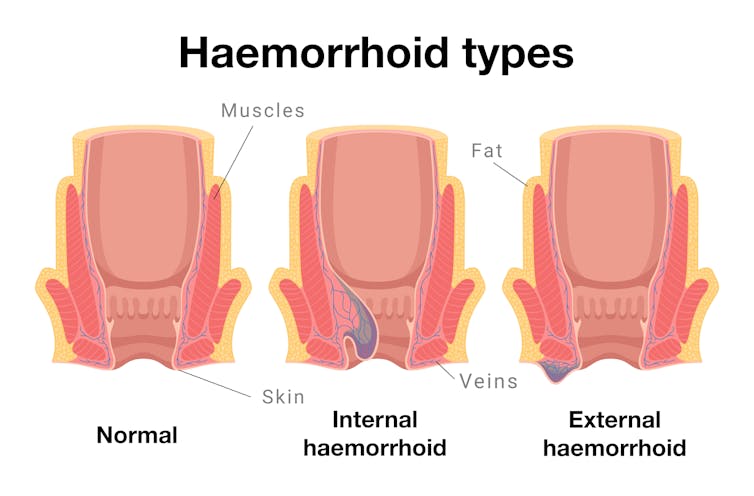
Arisara_Tongdonnoi/Getty What are haemorrhoids?
Every healthy person has haemorrhoids, sometimes called piles. They are columns of cushioned tissue and blood vessels found close to the opening of the anus.
We don’t notice haemorrhoids until they’re symptomatic. Aleksandr Kharitonov/Getty Haemorrhoids have a really important role in maintaining bowel continence or, to put it simply, keeping your poo in.
When all is well, we don’t notice them. But haemorrhoids can get swollen and this can lead to symptoms such as pain, bleeding or feeling a lump just inside your anus (internal haemorrhoids) or protruding outside (external haemorrhoids).
So when someone “has haemorrhoids”, it means they have become inflamed or symptomatic.
This is extremely common: more than one in two of us will experience symptomatic haemorrhoids at some point in our lives.
You are more likely to get haemorrhoids if you:
- are older (over 45)
- are pregnant
- are overweight
- have persistent constipation or diarrhoea
- regularly lift heavy objects
- spend a lot of time on the toilet.
The link between toilet time and haemorrhoids
Prolonged sitting in general has not been linked to developing haemorrhoids.
However, a standard toilet seat – unlike a chair or couch – has a large internal opening that provides no support for the pelvic floor (the group of muscles and ligaments that support the bladder, bowel and uterus).
Prolonged sitting on a toilet seat is believed to increase pressure inside the pelvic floor and lead to blood pooling in the vascular cushions of the anus. This makes haemorrhoids more likely to develop.
What the new study looked at
The new US study recruited 125 adults, aged 45 and older, who were undergoing a colonoscopy at Beth Israel Deaconess Medical centre.
Researchers surveyed them about their smartphone habits while using the toilet, including how often they checked their phone and for how long. Participants also reported on other behaviours such as straining, their fibre intake, and how much physical activity they did.
The researchers recorded whether they had haemorrhoids. Since the participants were all having a colonoscopy, the presence of internal haemorrhoids could be directly confirmed visually.
What did the study show?
Two-thirds (66%) of all participants used smartphones while on the toilet. The most common activity was reading news (54.3%), followed by social media (44.4%).
Those who used their smartphones spent longer on the toilet than those who didn’t. More than one in three (37.3%) toilet smartphone users spent over five minutes on the toilet, compared to just over one in 20 (7%) of those who didn’t use their smartphones.
The smartphone users had a 46% higher risk of haemorrhoids, compared to those who didn’t use their smartphone. To calculate this, researchers took into account other known risk factors for haemorrhoids such as gender, age, body mass index, exercise activity, straining and fibre intake.
However, unlike some other research, this study did not find a link between straining and haemorrhoids.
As a result, the researchers concluded that time spent on the toilet poses a more significant risk for haemorrhoids than straining. However, we can’t rule out straining as a risk factor, based on one study.
Some other limitations to consider
The study relied on participants remembering whether or not they strained, and how long they spent on the toilet.
This kind of recall is subjective, and may also be influenced by taking part in the study. For example, if the participants thought they had haemorrhoids, they may be more likely to report straining.
The study’s small sample size and the participants’ age (all over 45) also mean it is unlikely to be representative of the broader population.
Toilet sitting time
The new study is not the first to study the link between time spent on the toilet and developing haemorrhoids. In 2020, a Turkish study found spending more than five minutes on the toilet was associated with haemorrhoids.
Another 2020 study from Italy of 52 people with diagnosed internal or external haemorrhoids noted the longer they spent on the toilet, the more severe their haemorrhoids.
So, what are we doing on the toilet?
Defaecation itself usually doesn’t take long. One study found it took healthy adults an average two minutes when sitting, but only 51 seconds when squatting.
The majority of “toilet sitting time” usually means just that – sitting on the toilet, doing other activities aside from pooing (or weeing).
One 2008 study from Israel surveyed 500 adults and found more than half (52.7%) read books or newspapers while on the toilet. It also found toilet readers spent significantly more time on the toilet.
How to avoid haemorrhoids
The usual advice is to increase the amount of fibre in your diet (eating more fruit, vegetables and wholegrains) and ensure you drink enough water. This makes it easier to pass a stool and reduces straining – which you should also try to avoid.
However, the new research confirms previous evidence that cutting down toilet sitting time may also help. So, avoiding distractions by leaving your smartphone outside the bathroom is a good idea (and as a bonus, will expose your device to fewer germs).
If you have any concerning symptoms, such as blood in your stool, a new lump in the anal region, or pain when passing a bowel motion then you should see your local doctor for further investigations and treatment.
Vincent Ho, Associate Professor and Clinical Academic Gastroenterologist, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
‘Decision fatigue’ could be hurting your health. A nutritionist explains
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You’re standing in a supermarket aisle, weighing up whether to buy a microwave meal or a bunch of fresh carrots.
We all know making healthy eating choices can be tough. That’s especially true if you are hungry, or have a hungry household to feed.
There are so many reasons for this, and many are outside our control. But one you might not be aware of is a psychological concept known as “decision fatigue”.
So what exactly is decision fatigue? And could it help or hinder your healthy eating goals?
Peter Dazeley/Getty What is decision fatigue?
Decision fatigue, also known as choice overload, describes what happens when we make many effortful decisions over time.
Whenever you make a decision, you use a small amount of mental energy. As that energy runs low, you tend to make worse decisions.
This means you’re more likely to act without thinking, or simply choose what is easy or familiar. You might also find it harder to plan ahead and resist certain impulses.
This means you might be more likely to grab a takeaway instead of the ingredients to make a meal, or default to familiar comfort foods instead of making intentional, healthy choices.
How might it affect my eating habits?
The average person makes hundreds of food decisions each day.
You may think you’re just choosing a meal. But that one decision involves making many layered choices about what and how much you eat, as well as where, when and how you eat it.
You may make these choices subconsciously or automatically. But they each require to you weigh up various factors, such as taste, costs, time, expectations and more.
When decision fatigue sets in, you’re less likely to make thoughtful, health-focused choices. Instead, you may gravitate towards options that require less effort and offer quick rewards. You may also become more influenced by outside cues. An example of this is advertising that promotes convenient but high-calorie options such as fast food, snacks or indulgent treats.
Having too much information can make these decisions even harder. Nutrition advice often assesses the value of foods by how much protein, fat, fibre or vitamins they contain. This way of thinking, sometimes called nutritionism, can make food choices more complex. Instead of choosing food as food, we try to calculate and juggle many numbers at once.
Not the only factor
Several other factors may affect your food choices.
One is stress. One study from 2022 showed parents who experience high levels of both stress and decision fatigue found it more difficult to stick to positive food-related behaviours, such as making meals from scratch or eating together as a family.
Another is tiredness. One 2017 study showed time of day affected meal choices. It found between mealtimes, and especially in the afternoon, people were more likely to choose the simpler default food choice than one that required more consideration. This suggests having lower blood sugar and less mental energy meant people made less considered decisions.
How can I reduce my decision fatigue?
Here are four tips.
Have healthy foods on hand
When we’re low on mental or physical energy, we usually turn to what’s easy or familiar. That’s why it’s important to have healthy food options within reach. Thankfully, this doesn’t need to be complicated. It could look like pre-cutting fruit or having some healthy frozen meals in the freezer. And research suggests removing unhealthy foods – for example from the pantry or fridge – can be just as helpful when you’re trying to make healthier food choices.
Plan your meals
Planning meals could help too. This may involve setting some weekend time aside to decide what meals you’ll cook and eat. That’s instead of making last-minute decisions at the supermarket or on the drive home. Meal kits and batch cooking, which both reduce the number of food-related decisions you have to make, may also reduce decision fatigue.
Reframe your eating choices
How you frame choices may also improve your eating habits. For example, you may be more likely to “eat a colourful meal” rather than simply telling yourself to “eat more vegetables”.
Outsource some of the decision-making
If you’re looking for healthy, tasty recipes, you don’t need to re-invent the wheel. You can find a wealth of free ideas on the Eat for Health, Heart Foundation and National Nutrition Foundation websites. And if making food decisions feels overwhelming, Accredited Practicing Dietitians and Registered Nutritionists can help you turn complex nutrition advice into manageable steps.
The bottom line
We often think eating should be simple and intuitive, but blame ourselves when it doesn’t feel that way. However, the concept of decision fatigue shows healthy eating is not just about willpower. It’s also about noticing when you’re tired, stressed or time-poor, and taking practical steps to make healthy foods the easiest option.
Emma Beckett, Senior Lecturer, Nutrition and Food Science, Australian Catholic University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Carrot vs Pumpkin – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing carrots to pumpkin, we picked the carrots.
Why?
Both are great, but…
In terms of macros, carrots have 6x the fiber for slightly more carbs and (for what it’s worth, which isn’t much) slightly more protein, winning this round.
In the category of vitamins, carrots have more of vitamins A, B1, B3, B5, B6, B7, B9, E, K, and choline, while pumpkin has slightly more of vitamins B2, C, and E, giving a 9:3 win to carrots here.
Looking at minerals, carrots have more calcium and manganese, while pumpkin has more copper, iron, phosphorus, potassium, selenium, and zinc, finally winning a round.
In other considerations, both have a modest yet comparable array of polyphenols, for a tie in this round.
Adding up the sections makes for an overall win for carrots, but by all means enjoy either or both, as diversity is good!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: