Health Simplified – by Daniel Cottmeyer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Health Simplified – by Daniel Cottmeyer
A lot of books focus on the most marketable aspects of health, such as fat loss or muscle gain. Instead, Cottmeyer takes a “birds-eye-view” of health in all its aspects, and then boils it down to the most critical key parts.
Rather than giving a science-dense tome that nobody reads, or a light motivational piece that everyone reads but it amounts to “you can do it!”, here we get substance… but in a digestible form.
Which we at 10almonds love.
The book presents a simple action plan to:
- Improve your relationship with food/exercise
- Actually get better sleep
- Understand how nutrition really works
- Set up helpful habits that are workable and sustainable
- Bring these components together synergistically
Bottom line: if you’re going to buy only one health/fitness book, this is a fine contender.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Some women’s breasts can’t make enough milk, and the effects can be devastating

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many new mothers worry about their milk supply. For some, support from a breastfeeding counsellor or lactation consultant helps.
Others cannot make enough milk no matter how hard they try. These are women whose breasts are not physically capable of producing enough milk.
Our recently published research gives us clues about breast features that might make it difficult for some women to produce enough milk. Another of our studies shows the devastating consequences for women who dream of breastfeeding but find they cannot.
Some breasts just don’t develop
Unlike other organs, breasts are not fully developed at birth. There are key developmental stages as an embryo, then again during puberty and pregnancy.
At birth, the breast consists of a simple network of ducts. Usually during puberty, the glandular (milk-making) tissue part of the breast begins to develop and the ductal network expands. Then typically, further growth of the ductal network and glandular tissue during pregnancy prepares the breast for lactation.
But our online survey of women who report low milk supply gives us clues to anomalies in how some women’s breasts develop.
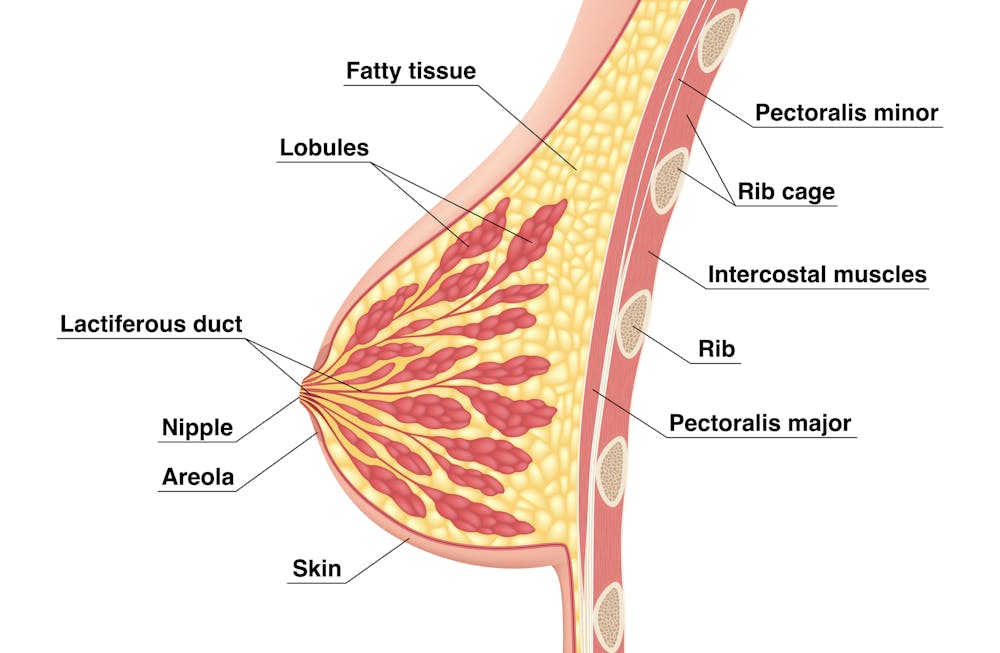
We’re not talking about women with small breasts, but women whose glandular tissue (shown in this diagram as “lobules”) is underdeveloped and have a condition called breast hypoplasia.

Sometimes not enough glandular tissue, shown here as lobules, develop.
Tsuyna/ShutterstockWe don’t know how common this is. But it has been linked with lower rates of exclusive breastfeeding.
We also don’t know what causes it, with much of the research conducted in animals and not humans.
However, certain health conditions have been associated with it, including polycystic ovary syndrome and other endocrine (hormonal) conditions. A high body-mass index around the time of puberty may be another indicator.
Could I have breast hypoplasia?
Our survey and other research give clues about who may have breast hypoplasia.
But it’s important to note these characteristics are indicators and do not mean women exhibiting them will definitely be unable to exclusively breastfeed.
Indicators include:
- a wider than usual gap between the breasts
- tubular-shaped (rather than round) breasts
- asymmetric breasts (where the breasts are different sizes or shapes)
- lack of breast growth in pregnancy
- a delay in or absence of breast fullness in the days after giving birth
In our survey, 72% of women with low milk supply had breasts that did not change appearance during pregnancy, and about 70% reported at least one irregular-shaped breast.
The effects
Mothers with low milk supply – whether or not they have breast hyoplasia or some other condition that limits their ability to produce enough milk – report a range of emotions.
Research, including our own, shows this ranges from frustration, confusion and surprise to intense or profound feelings of failure, guilt, grief and despair.
Some mothers describe “breastfeeding grief” – a prolonged sense of loss or failure, due to being unable to connect with and nourish their baby through breastfeeding in the way they had hoped.
These feelings of failure, guilt, grief and despair can trigger symptoms of anxiety and depression for some women.
Feelings of failure, guilt, grief and despair were common.
Bricolage/ShutterstockOne woman told us:
[I became] so angry and upset with my body for not being able to produce enough milk.
Many women’s emotions intensified when they discovered that despite all their hard work, they were still unable to breastfeed their babies as planned. A few women described reaching their “breaking point”, and their experience felt “like death”, “the worst day of [my] life” or “hell”.
One participant told us:
I finally learned that ‘all women make enough milk’ was a lie. No amount of education or determination would make my breasts work. I felt deceived and let down by all my medical providers. How dare they have no answers for me when I desperately just wanted to feed my child naturally.
Others told us how they learned to accept their situation. Some women said they were relieved their infant was “finally satisfied” when they began supplementing with formula. One resolved to:
prioritise time with [my] baby over pumping for such little amounts.
Where to go for help
If you are struggling with low milk supply, it can help to see a lactation consultant for support and to determine the possible cause.
This will involve helping you try different strategies, such as optimising positioning and attachment during breastfeeding, or breastfeeding/expressing more frequently. You may need to consider taking a medication, such as domperidone, to see if your supply increases.
If these strategies do not help, there may be an underlying reason why you can’t make enough milk, such as insufficient glandular tissue (a confirmed inability to make a full supply due to breast hypoplasia).
Even if you have breast hypoplasia, you can still breastfeed by giving your baby extra milk (donor milk or formula) via a bottle or using a supplementer (which involves delivering milk at the breast via a tube linked to a bottle).
More resources
The following websites offer further information and support:
- Australian Breastfeeding Association
- Lactation Consultants of Australia and New Zealand
- Royal Women’s Hospital, Melbourne
- Supply Line Breastfeeders Support Group of Australia Facebook support group
- IGT And Low Milk Supply Support Group Facebook support group
- Breastfeeding Medicine Network Australia/New Zealand
- Supporting breastfeeding grief (a collection of resources).
Shannon Bennetts, a research fellow at La Trobe University, contributed to this article.

Renee Kam, PhD candidate and research officer, La Trobe University and Lisa Amir, Professor in Breastfeeding Research, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Body by Science – by Dr. Doug McGuff & John Little
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The idea that you’ll get a re-sculpted body at 12 minutes per week is a bold claim, isn’t it? Medical Doctor Doug McGuff and bodybuilder John Little team up to lay out their case. So, how does it stand up to scrutiny?
First, is it “backed by rigorous research” as claimed? Yes… with caveats.
The book uses a large body of scientific literature as its foundation, and that weight of evidence does support this general approach:
- Endurance cardio isn’t very good at burning fat
- Muscle, even just having it without using it much, burns fat to maintain it
- To that end, muscle can be viewed as a fat-burning asset
- Muscle can be grown quickly with short bursts of intense exercise once per week
Why once per week? The most relevant muscle fibers take about that long to recover, so doing it more often will undercut gains.
So, what are the caveats?
The authors argue for slow reps of maximally heavy resistance work sufficient to cause failure in about 90 seconds. However, most of the studies cited for the benefits of “brief intense exercise” are for High Intensity Interval Training (HIIT). HIIT involves “sprints” of exercise. It doesn’t have to be literally running, but for example maxing out on an exercise bike for 30 seconds, slowing for 60, maxing out for 30, etc. Or in the case of resistance work, explosive (fast!) concentric movements and slow eccentric movements, to work fast- and slow-twitch muscle fibers, respectively.
What does this mean for the usefulness of the book?
- Will it sculpt your body as described in the blurb? Yes, this will indeed grow your muscles with a minimal expenditure of time
- Will it improve your body’s fat-burning metabolism? Yes, this will indeed turn your body into a fat-burning machine
- Will it improve your “complete fitness”? No, if you want to be an all-rounder athlete, you will still need HIIT, as otherwise anything taxing your under-worked fast-twitch muscle fibers will exhaust you quickly.
Bottom line: read this book if you want to build muscle efficiently, and make your body more efficient at burning fat. Best supplemented with at least some cardio, though!
Click here to check out Body by Science, and get re-sculpting yours!
Share This Post
-

High Histamine Foods To Avoid (And Low Histamine Foods To Eat Instead)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Nour Zibdeh is an Integrative and Functional Dietician, and she helps people overcome food intolerances. Today, it’s about getting rid of the underdiagnosed condition that is histamine intolerance, by first eliminating the triggers, and then not getting stuck on the low-histamine diet
The recommendations
High histamine foods to avoid include:
- Alcohol (all types)
- Fermented foods—normally great for the gut, but bad in this case
- That includes most cheeses and yogurts
- Aged, cured, or otherwise preserved meat
- Some plants, e.g. tomato, spinach, eggplant, banana, avocado. Again, normally all great, but not in this case.
Low histamine foods to eat include:
- Fruits and vegetables not mentioned above
- Minimally processed meat and fish, either fresh from the butcher/fishmonger, or frozen (not from the chilled food section of the supermarket), and eaten the same day they were purchased or defrosted, because otherwise histamine builds up over time (and quite quickly)
- Grains, but she recommends skipping gluten, given the high likelihood of a comorbid gluten intolerance. So instead she recommends for example quinoa, oats, rice, buckwheat, millet, etc.
For more about these (and more examples), as well as how to then phase safely off the low histamine diet, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Further reading
Food intolerances often gang up on a person (i.e., comorbidity is high), so you might also like to read about:
- Gluten: What’s The Truth?
- Fiber For FODMAP-Avoiders
- Foods For Managing Hypothyroidism (incl. Hashimoto’s)
- Crohn’s, Food Intolerances, & More
Take care!
Share This Post

Related Posts
-

Strawberries vs Blackberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing strawberries to blackberries, we picked the blackberries.
Why?
Shocking nobody, both are very healthy options. However, blackberries do come out on top:
In terms of macros, the main thing that sets them apart is that blackberries have more than 2x the fiber. Other differences in macros are also in blackberries’ favor, but only very marginally, so we’ll not distract with those here. The fiber difference is distinctly significant, though.
In the category of vitamins, blackberries lead with more of vitamins A, B2, B3, B5, B9, E, and K, as well as more choline. Meanwhile, strawberries boast more of vitamins B1, B6, and C. So, a 8:2 advantage for blackberries (and some of the margins are very large, such as 9x more choline, 4x more vitamin E, and nearly 18x more vitamin A).
When it comes to minerals, things are not less clear: blackberries have considerably more calcium, copper, iron, magnesium, manganese, and zinc. The two fruits are equal in other minerals that they both contain, and strawberries don’t contain any mineral in greater amounts than blackberries do.
A discussion of these berries’ health benefits would be incomplete without at least mentioning polyphenols, but both of them are equally good sources of such, so there’s no distinction to set one above the other in this category.
As ever, enjoy both, though! Diversity is good.
Want to learn more?
You might like to read:
- Strawberries vs Cherries – Which is Healthier?
- Blackberries vs Blueberries – Which is Healthier?
- Strawberries vs Raspberries – Which is Healthier?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How Useful Is Hydrotherapy?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hyyyyyyydromatic…
Hydrotherapy is a very broad term, and refers to any (external) use of water as part of a physical therapy. Today we’re going to look at some of the top ways this can be beneficial—maybe you’ll know them all already, but maybe there’s something you hadn’t thought about or done decently; let’s find out!
Notwithstanding the vague nature of the umbrella term, some brave researchers have done a lot of work to bring us lots of information about what works and what doesn’t, so we’ll be using this to guide us today. For example:
Scientific Evidence-Based Effects of Hydrotherapy on Various Systems of the Body
Swimming (and similar)
An obvious one, this can for most people be a very good full-body exercise, that’s exactly as strenuous (or not) as you want/need it to be.
It can be cardio, it can be resistance, it can be endurance, it can be high-intensity interval training, it can be mobility work, it can be just support for an aching body that gets to enjoy being in the closest to zero-gravity we can get without being in freefall or in space.
See also: How To Do HIIT (Without Wrecking Your Body)
Depending on what’s available for you locally (pool with a shallow area, for example), it can also be a place to do some exercises normally performed on land, but with your weight being partially supported (and as a counterpoint, a little resistance added to movement), and no meaningful risk of falling.
Tip: check out your local facilities, to see if they offer water aerobics classes; because the water necessitates slow movement, this can look a lot like tai chi to watch, but it’s great for mobility and balance.
Water circuit therapy
This isn’t circuit training! Rather, it’s a mixture of thermo- and cryotherapy, that is to say, alternating warm and cold water immersion. This can also be interspersed with the use of a sauna, of course.
See also:
- Ice Baths: To Dip Or Not To Dip?
- Saunas: Health Benefits (& Caveats)
- The Stress Prescription (Against Aging!)
this last one is about thermal shock-mediated hormesis, which sounds drastic, but it’s what we’re doing here with the hot and cold, and it’s good for most people!
Pain relief
Most of the research for this has to do with childbirth pain rather than, for example, back pain, but the science is promising:
Post-exercise recovery
It can be tempting to sink into a hot bath, or at least enjoy a good hot shower, after strenuous exercise. But does it help recovery too? The answer is probably yes:
Effect of hot water immersion on acute physiological responses following resistance exercise
For more on that (and other means of improving post-exercise recovery), check out our previous main feature:
How To Speed Up Recovery After A Workout (According To Actual Science)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Top 8 Fruits That Prevent & Kill Cancer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Amy Dee, pharmacist and cancer survivor herself, lays out the best options for anticancer fruits:
The fruits
Without further ado, they are:
- Kiwi: promotes cancer cell death while sparing healthy cells
- Plums & peaches: an interesting choice to list these similar fruits together as one item, but they both also induce cell death in cancer cells while sparing healthy ones
- Dragon fruit: this does the same, while also inhibiting cancer cell growth
- Figs: these have antitumor effects specifically, while removing carcinogens too, and additionally sensitizing cancer cells to light therapy
- Cranberries: disrupt cancer cell adhesion, breaking down tumors, while protecting non-cancerous cells against DNA damage
- Citrus fruits: inhibit tumor growth and kill cancer cells; regular consumption is also associated with a lower cancer risk (be warned though, grapefruit interacts with some medications)
- Cherries: induce cancer cell death; protect healthy cells against DNA damage
- Tomatoes: don’t often make it into lists of fruits, but lycopene reduces cancer risk, and slows the growth of cancer cells (10almonds note: watermelon has more lycopene than tomatoes, and is more traditionally considered a fruit in all respects, so could have taken the spot here).
We would also argue that apricots could have had a spot on the list, both for their lycopene content (comparable to tomatoes) and their botanical (and thus phytochemical) similarities to peaches and plums.
For more information on each of these (she also talks about the different polyphenols and other nutrients that constitute the active compounds delivering these anticancer effects), enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Food Choice & Cancer Risk: Eat To Beat Cancer
- Beat Cancer Kitchen: Deliciously Simple Plant-Based Anticancer Recipes (book)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: