Gluten: What’s The Truth?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Gluten: What’s The Truth?
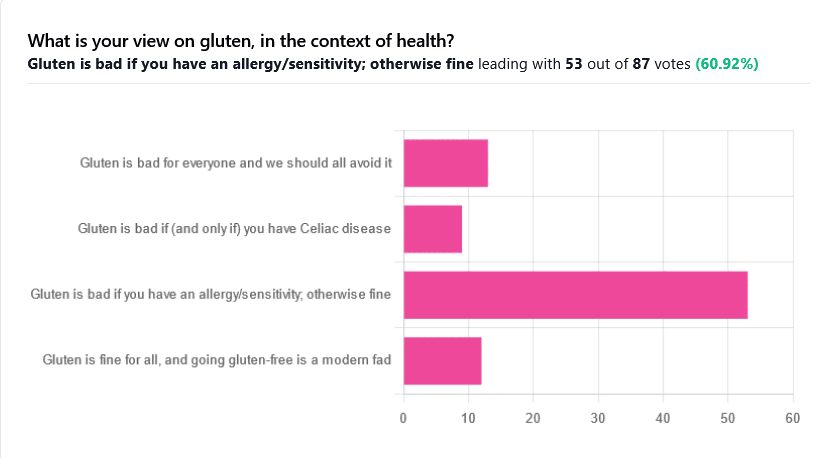
We asked you for your health-related view of gluten, and got the above spread of results. To put it simply:
Around 60% of voters voted for “Gluten is bad if you have an allergy/sensitivity; otherwise fine”
The rest of the votes were split fairly evenly between the other three options:
- Gluten is bad for everyone and we should avoid it
- Gluten is bad if (and only if) you have Celiac disease
- Gluten is fine for all, and going gluten-free is a modern fad
First, let’s define some terms so that we’re all on the same page:
What is gluten?
Gluten is a category of protein found in wheat, barley, rye, and triticale. As such, it’s not one single compound, but a little umbrella of similar compounds. However, for the sake of not making this article many times longer, we’re going to refer to “gluten” without further specification.
What is Celiac disease?
Celiac disease is an autoimmune disease. Like many autoimmune diseases, we don’t know for sure how/why it occurs, but a combination of genetic and environmental factors have been strongly implicated, with the latter putatively including overexposure to gluten.
It affects about 1% of the world’s population, and people with Celiac disease will tend to respond adversely to gluten, notably by inflammation of the small intestine and destruction of enterocytes (the cells that line the wall of the small intestine). This in turn causes all sorts of other problems, beyond the scope of today’s main feature, but suffice it to say, it’s not pleasant.
What is an allergy/intolerance/sensitivity?
This may seem basic, but a lot of people conflate allergy/intolerance/sensitivity, so:
- An allergy is when the body mistakes a harmless substance for something harmful, and responds inappropriately. This can be mild (e.g. allergic rhinitis, hayfever) or severe (e.g. peanut allergy), and as such, responses can vary from “sniffly nose” to “anaphylactic shock and death”.
- In the case of a wheat allergy (for example), this is usually somewhere between the two, and can for example cause breathing problems after ingesting wheat or inhaling wheat flour.
- An intolerance is when the body fails to correctly process something it should be able to process, and just ejects it half-processed instead.
- A common and easily demonstrable example is lactose intolerance. There isn’t a well-defined analog for gluten, but gluten intolerance is nonetheless a well-reported thing.
- A sensitivity is when none of the above apply, but the body nevertheless experiences unpleasant symptoms after exposure to a substance that should normally be safe.
- In the case of gluten, this is referred to as non-Celiac gluten sensitivity
A word on scientific objectivity: at 10almonds we try to report science as objectively as possible. Sometimes people have strong feelings on a topic, especially if it is polarizing.
Sometimes people with a certain condition feel constantly disbelieved and mocked; sometimes people without a certain condition think others are imagining problems for themselves where there are none.
We can’t diagnose anyone or validate either side of that, but what we can do is report the facts as objectively as science can lay them out.
Gluten is fine for all, and going gluten-free is a modern fad: True or False?
Definitely False, Celiac disease is a real autoimmune disease that cannot be faked, and allergies are also a real thing that people can have, and again can be validated in studies. Even intolerances have scientifically measurable symptoms and can be tested against nocebo.
See for example:
- Epidemiology and clinical presentations of Celiac disease
- Severe forms of food allergy that can precipitate allergic emergencies
- Properties of gluten intolerance: gluten structure, evolution, and pathogenicity
However! It may not be a modern fad, so much as a modern genuine increase in incidence.
Widespread varieties of wheat today contain a lot more gluten than wheat of ages past, and many other molecular changes mean there are other compounds in modern grains that never even existed before.
However, the health-related impact of these (novel proteins and carbohydrates) is currently still speculative, and we are not in the business of speculating, so we’ll leave that as a “this hasn’t been studied enough to comment yet but we recognize it could potentially be a thing” factor.
Gluten is bad if (and only if) you have Celiac disease: True or False?
Definitely False; allergies for example are well-evidenced as real; same facts as we discussed/linked just above.
Gluten is bad for everyone and we should avoid it: True or False?
False, tentatively and contingently.
First, as established, there are people with clinically-evidenced Celiac disease, wheat allergy, or similar. Obviously, they should avoid triggering those diseases.
What about the rest of us, and what about those who have non-Celiac gluten sensitivity?
Clinical testing has found that of those reporting non-Celiac gluten sensitivity, nocebo-controlled studies validate that diagnosis in only a minority of cases.
In the following study, for example, only 16% of those reporting symptoms showed them in the trials, and 40% of those also showed a nocebo response (i.e., like placebo, but a bad rather than good effect):
This one, on the other hand, found that positive validations of diagnoses were found to be between 7% and 77%, depending on the trial, with an average of 30%:
Re-challenge Studies in Non-celiac Gluten Sensitivity: A Systematic Review and Meta-Analysis
In other words: non-Celiac gluten sensitivity is a thing, and/but may be over-reported, and/but may be in some part exacerbated by psychosomatic effect.
Note: psychosomatic effect does not mean “imagining it” or “all in your head”. Indeed, the “soma” part of the word “psychosomatic” has to do with its measurable effect on the rest of the body.
For example, while pain can’t be easily objectively measured, other things, like inflammation, definitely can.
As for everyone else? If you’re enjoying your wheat (or similar) products, it’s well-established that they should be wholegrain for the best health impact (fiber, a positive for your health, rather than white flour’s super-fast metabolites padding the liver and causing metabolic problems).
Wheat itself may have other problems, for example FODMAPs, amylase trypsin inhibitors, and wheat germ agglutinins, but that’s “a wheat thing” rather than “a gluten thing”.
That’s beyond the scope of today’s main feature, but you might want to check out today’s featured book!
For a final scientific opinion on this last one, though, here’s what a respected academic journal of gastroenterology has to say:
From coeliac disease to noncoeliac gluten sensitivity; should everyone be gluten-free?
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Managing Your Mortality

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When Planning Is a Matter of Life and Death
Barring medical marvels as yet unrevealed, we are all going to die. We try to keep ourselves and our loved ones in good health, but it’s important to be prepared for the eventuality of death.
While this is not a cheerful topic, considering these things in advance can help us manage a very difficult thing, when the time comes.
We’ve put this under “Psychology Sunday” as it pertains to processing our own mortality, and managing our own experiences and the subsequent grief that our death may invoke in our loved ones.
We’ll also be looking at some of the medical considerations around end-of-life care, though.
Organizational considerations
It’s generally considered good to make preparations in advance. Write (or update) a Will, tie up any loose ends, decide on funerary preferences, perhaps even make arrangements with pre-funding. Life insurance, something difficult to get at a good rate towards the likely end of one’s life, is better sorted out sooner rather than later, too.
Beyond bureaucracy
What’s important to you, to have done before you die? It could be a bucket list, or it could just be to finish writing that book. It could be to heal a family rift, or to tell someone how you feel.
It could be more general, less concrete: perhaps to spend more time with your family, or to engage more with a spiritual practice that’s important to you.
Perhaps you want to do what you can to offset the grief of those you’ll leave behind; to make sure there are happy memories, or to make any requests of how they might remember you.
Lest this latter seem selfish: after a loved one dies, those who are left behind are often given to wonder: what would they have wanted? If you tell them now, they’ll know, and can be comforted and reassured by that.
This could range from “bright colors at my funeral, please” to “you have my blessing to remarry if you want to” to “I will now tell you the secret recipe for my famous bouillabaisse, for you to pass down in turn”.
End-of-life care
Increasingly few people die at home.
- Sometimes it will be a matter of fighting tooth-and-nail to beat a said-to-be-terminal illness, and thus expiring in hospital after a long battle.
- Sometimes it will be a matter of gradually winding down in a nursing home, receiving medical support to the end.
- Sometimes, on the other hand, people will prefer to return home, and do so.
Whatever your preferences, planning for them in advance is sensible—especially as money may be a factor later.
Not to go too much back to bureaucracy, but you might also want to consider a Living Will, to be enacted in the case that cognitive decline means you cannot advocate for yourself later.
Laws vary from place to place, so you’ll want to discuss this with a lawyer, but to give an idea of the kinds of things to consider:
National Institute on Aging: Preparing A Living Will
Palliative care
Palliative care is a subcategory of end-of-life care, and is what occurs when no further attempts are made to extend life, and instead, the only remaining goal is to reduce suffering.
In the case of some diseases including cancer, this may mean coming off treatments that have unpleasant side-effects, and retaining—or commencing—pain-relief treatments that may, as a side-effect, shorten life.
Euthanasia
Legality of euthanasia varies from place to place, and in some times and places, palliative care itself has been considered a form of “passive euthanasia”, that is to say, not taking an active step to end life, but abstaining from a treatment that prolongs it.
Clearer forms of passive euthanasia include stopping taking a medication without which one categorically will die, or turning off a life support machine.
Active euthanasia, taking a positive action to end life, is legal in some places and the means varies, but an overdose of barbiturates is an example; one goes to sleep and does not wake up.
It’s not the only method, though; options include benzodiazepines, and opioids, amongst others:
Efficacy and safety of drugs used for assisted dying
Unspoken euthanasia
An important thing to be aware of (whatever your views on euthanasia) is the principle of double-effect… And how it comes to play in palliative care more often than most people think.
Say a person is dying of cancer. They opt for palliative care; they desist in any further cancer treatments, and take medication for the pain. Morphine is common. Morphine also shortens life.
It’s common for such a patient to have a degree of control over their own medication, however, after a certain point, they will no longer be in sufficient condition to do so.
After this point, it is very common for caregivers (be they medical professionals or family members) to give more morphine—for the purpose of reducing suffering, of course, not to kill them.
In practical terms, this often means that the patient will die quite promptly afterwards. This is one of the reasons why, after sometimes a long-drawn-out period of “this person is dying”, healthcare workers can be very accurate about “it’s going to be in the next couple of days”.
The take-away from this section is: if you would like for this to not happen to you or your loved one, you need to be aware of this practice in advance, because while it’s not the kind of thing that tends to make its way into written hospital/hospice policies, it is very widespread and normalized in the industry on a human level.
Further reading: Goods, causes and intentions: problems with applying the doctrine of double effect to palliative sedation
One last thing…
Planning around our own mortality is never a task that seems pressing, until it’s too late. We recommend doing it anyway, without putting it off, because we can never know what’s around the corner.
Share This Post
-

Trout vs Carp – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing trout to carp, we picked the trout.
Why?
Both have their strong points!
In terms of macros, trout has slightly more protein and fat, and/but also has less cholesterol than carp. So, we pick the trout in the macros category.
In the category of vitamins, trout has much more of vitamins A, B1, B2, B3, B5, B6, B7, B12, C, D, E, K, and choline, while carp has slightly more vitamin B9. In other words, an easy win for trout here.
When it comes to minerals, however, trout has more potassium and selenium, while carp has more calcium, copper, iron, magnesium, manganese, phosphorus, and zinc. A fair win for carp this time.
You may be wondering about heavy metals: this will vary depending on location, as well as the age of the fish (younger fish have had less time to accumulate heavy metals than old ones, so if you’re visiting the fishmonger, choose the smaller ones) and the lives they have led (e.g. wild vs farmed), however, as a general rule of thumb, trout will generally have lower heavy metals levels than carp, all other things (e.g. location, age, etc) being equal.
In short, enjoy either or both in moderation, but trout wins on 3/4 categories today.
Want to learn more?
You might like to read:
Farmed Fish vs Wild Caught: Antibiotics, Mercury, & More
Take care!
Share This Post
-

Death by Sitting – by Carolyne Thompson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You may be wondering: is this a lot of words to say “sit down less”?
And the answer is: there’s a lot more in here than that. Of course, yes, “sit down less” is an important take-away, but there’s a lot about the specific problems caused by sitting in chairs, the health risks are that are increased and how, and the early warning signs to watch out for.
After these chapters of woe, most of the book is given over to solutions; about taking standing and walking breaks, tying movement to productivity, why exercise alone is not enough to offset the damage of sitting, relearning ergonomic posture in the context of mitigating the harm, psychological shifts to break the habit of sitting, redefining social norms around sitting and socializing, rewiring one’s body and retraining better movements as well as postures to always immediately move out of if one finds oneself in, and much much more.
The style is light and easy to read, while still including scientific research as appropriate along with practical, actionable advice.
Bottom line: if you’d like to do better for your body than slowly killing it for however many hours a day, then this book has a wealth of advice far beyond the obvious (but important!) “sit less”.
Share This Post
Related Posts
-
Kidney Beans vs White Beans – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing kidney beans to white beans, we picked the white.
Why?
It was close, and each has its strengths! Bear in mind, these are very closely-related beans. But as we say, there are distinguishing factors…
In terms of macros, kidney beans have very slightly more fiber and white beans have very slightly more protein. But both are close enough in both of those things to call this a tie in this category.
When it comes to vitamins, there are two ways of looking at this:
- kidney beans have more of vitamins B1, B2, B3, B6, B9, C, and K, while white beans have more vitamin B5, E, and choline
- kidney beans have slightly more of some vitamins that don’t usually see a deficiency, while white beans have 31x more vitamin E
Nevertheless, we’re sticking by our usual method of noting that this is a 7:3 win for kidney beans in this category; we just wanted to note that in practical health terms, an argument can be made for white beans on the vitamin front too.
In the category of minerals, kidney beans have slightly more phosphorus, while white beans have more calcium, copper, iron, magnesium, manganese, potassium, selenium, and zinc. An easy win for white beans this time.
(In case you’re wondering about the margin on phosphorus, it was 0.2x more, so we’re not seeing a situation like white beans’ 31x more vitamin E)
In short: both are great and both have their strengths. Enjoy both, together if you like! But if we have to pick one, we’re going with white beans.
Want to learn more?
You might like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Drug Metabolism (When You’re Not Average!)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When Your Medications Run Out… Of You
Everybody knows that alcohol can affect medications’ effects, but what of smoking, and what of obesity? And how does the alcohol thing work anyway?
It’s all about the enzymes
Medicines that are processed by the liver (which is: most medicines) are metabolized there by specialist enzymes, and the things we do can increase or decrease the quantity of those enzymes—and/or how active they are.
Dr. Kata Wolff Pederson and her team of researchers at Aarhus University in Denmark examined the livers of recently deceased donors in ways that can’t (ethically) be done with live patients, and were able to find the associations between various lifestyle factors and different levels of enzymes responsible for drug metabolism.
And it’s not always how you might think!
Some key things they found:
- Smokers have twice as high levels of enzyme CYP1A2 than non-smokers, which results in the faster metabolism of a lot of drugs.
- Drinkers have 30% higher levels of enzyme CYP2E1, which also results in a faster metabolism of a lot of drugs.
- Patients with obesity have 50% lower levels of enzyme CYP3A4, resulting in slower metabolism of many drugs
This gets particularly relevant when we take into account the next fact:
- Of the individuals in the study, 40% died from poisoning from a mixture of drugs (usually: prescription and otherwise)
Read in full: Sex- and Lifestyle-Related Factors are Associated with Altered Hepatic CYP Protein Levels
Read a pop-sci article about it: Your lifestyle can determine how well your medicine will work
How much does the metabolism speed matter?
It can matter a lot! If you’re taking drugs and carefully abiding by the dosage instructions, those instructions were assuming they know your speed of metabolism, and this is based on an average.
- If your metabolism is faster, you can get too much of a drug too quickly, and it can harm you
- If your metabolism is faster, it also means that while yes it’ll start working sooner, it’ll also stop working sooner
- If it’s a painkiller, that’s inconvenient. If it’s a drug that keeps you alive, then well, that’s especially unfortunate.
- If your metabolism is slower, it can mean your body is still processing the previous dose(s) when you take the next one, and you can overdose (and potentially die)
We touched on this previously when we talked about obesity in health care settings, and how people can end up getting worse care:
As for alcohol and drugs? Obviously we do not recommend, but here’s some of the science of it with many examples:
Why it’s a bad idea to mix alcohol with some medications
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What Too Much Exercise Does To Your Body And Brain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Get more exercise” is a common rallying-cry for good health, but it is possible to overdo it. And, this is not just a matter of extreme cases of “exercise addiction”, but even going much above certain limits can already result in sabotaging one’s healthy gains. But how, and where does the line get drawn?
Too Much Of A Good Thing
The famous 150 minutes per week of moderate exercise (or 75 minutes of intense exercise) is an oft-touted figure. This video, on the other hand, springs for 5 hours of moderate exercise or 2.5 hours intense exercise as a good guideline.
We’re advised that going over those guidelines doesn’t necessarily increase health benefits, and on the contrary, may reduce or even reverse them. For example, we are told…
- Light to moderate running reduces the risk of death, but running intensely more than 3 times a week can negate these benefits.
- Extreme endurance exercises, like ultra-marathons, may cause heart damage, heart rhythm disorders, and artery enlargement.
- Women who exercise strenuously every day have a higher risk of heart attacks and strokes compared to those who exercise moderately.
- Excessive exercise in women can lead to the “female athlete triad” (loss of menstruation, osteoporosis, and eating disorders).
- In men, intense exercise can lower libido due to fatigue and reduced testosterone levels.
- Both men and women are at increased risk of overuse injuries (e.g., tendinitis, stress fractures) and impaired immunity from excessive exercise.
- There is a 72-hour window of impaired immunity after intense exercise, increasing the risk of infections.
Exercise addiction is rare, though, with this video citing “around 1 million people in the US suffer from exercise addiction”.
For more on finding the right balance, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: