Fermenting Everything – by Andy Hamilton
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is not justanother pickling book! This is, instead, what it says on the front cover, “fermenting everything”.
Ok, maybe not literally everything, but every kind of thing that can reasonably be fermented, and it’s probably a lot more things than you might think.
From habanero chutney to lacto-lemonade, aioli to kombucha, Ukrainian fermented tomatoes to kvass. We could go on, but we’d soon run out of space. You get the idea. If it’s a fermented product (food, drink, condiment) and you’ve heard of it, there’s probably a recipe in here.
All in all, this is a great way to get in your gut-healthy daily dose of fermented products!
He does also talk safety, and troubleshooting too. And so long as you have a collection of big jars and a fairly normally-furnished kitchen, you shouldn’t need any more special equipment than that, unless you decide to you your fermentation skills for making beer (which does need some extra equipment, and he offers advice on that—our advice as a health science publication is “don’t drink beer”, though).
Bottom line: with this in hand, you can create a lot of amazing foods/drinks/condiments that are not only delicious, but also great for gut health.
Click here to check out Fermenting Everything, and widen your culinary horizons!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Antidepressants: Personalization Is Key!

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Antidepressants: Personalization Is Key!

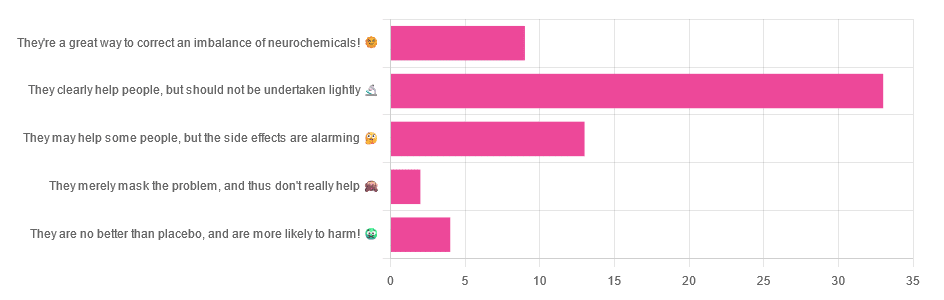
Yesterday, we asked you for your opinions on antidepressants, and got the above-depicted, below-described, set of responses:
- Just over half of respondents said “They clearly help people, but should not be undertaken lightly”
- Just over a fifth of respondents said “They may help some people, but the side effects are alarming”
- Just under a sixth of respondents said “They’re a great way to correct an imbalance of neurochemicals”
- Four respondents said “They are no better than placebo, and are more likely to harm”
- Two respondents said “They merely mask the problem, and thus don’t really help”
So what does the science say?
❝They are no better than placebo, and are more likely to harm? True or False?❞
True or False depending on who you are and what you’re taking. Different antidepressants can work on many different systems with different mechanisms of action. This means if and only if you’re not taking the “right” antidepressant for you, then yes, you will get only placebo benefits:
- Placebo Effect in the Treatment of Depression and Anxiety ← randomly assigned antidepressants are, shockingly, luck of the draw in usefulness
- Antidepressants versus placebo in major depression: an overview ← “wow this science is messy”
- Comparative efficacy and acceptability of 21 antidepressant drugs: a systematic review and network meta-analysis ← “oh look, it makes a difference which antidepressant we give to people”
Rather than dismissing antidepressants as worthless, therefore, it is a good idea to find out (by examination or trial and error) what kind of antidepressant you need, if you indeed do need such.
Otherwise it is like getting a flu shot and being surprised when you still catch a cold!
❝They merely mask the problem, and thus don’t really help: True or False?❞
False, categorically.
The problem in depressed people is the depressed mood. This may be influenced by other factors, and antidepressants indeed won’t help directly with those, but they can enable the person to better tackle them (more on this later).
❝They may help some people, but the side-effects are alarming: True or False?❞
True or False depending on more factors than we can cover here.
Side-effects vary from drug to drug and person to person, of course. As does tolerability and acceptability, since to some extent these things are subjective.
One person’s dealbreaker may be another person’s shrugworthy minor inconvenience at most.
❝They’re a great way to correct an imbalance of neurochemicals: True or False?❞
True! Contingently.
That is to say: they’re a great way to correct an imbalance of neurochemicals if and only if your problem is (at least partly) an imbalance of neurochemicals. If it’s not, then your brain can have all the neurotransmitters it needs, and you will still be depressed, because (for example) the other factors* influencing your depression have not changed.
*common examples include low self-esteem, poor physical health, socioeconomic adversity, and ostensibly bleak prospects for the future.
For those for whom the problem is/was partly a neurochemical imbalance and partly other factors, the greatest help the antidepressants give is getting the brain into sufficient working order to be able to tackle those other factors.
Want to know more about the different kinds?
Here’s a helpful side-by-side comparison of common antidepressants, what type they are, and other considerations:
Mind | Comparing Antidepressants
Want a drug-free approach?
You might like our previous main feature:
The Mental Health First-Aid That You’ll Hopefully Never Need
Take care!
Share This Post
-

Codependent No More – by Melody Beattie
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is a book review, not a book summary, but first let’s quickly cover a common misconception, because the word “codependent” gets misused a lot in popular parlance:
- What codependence isn’t: “we depend on each other and must do everything together”
- What codependence is:“person 1 has a dependency on a substance (or perhaps a behavior, such as gambling); person 2 is trying to look after person 1, and so has developed a secondary relationship with the substance/behavior. Person 2 is now said to be codependent, because it becomes all-consuming for them too, even if they’re not using the substance/behavior directly”
Funny how often it happens that the reality is more complex than the perception, isn’t it?
Melody Beattie unravels all this for us. We get a compassionate and insightful look at how we can look after ourselves, while looking after another. Perhaps most importantly: how and where to draw a line of what we can and cannot do/change for them.
Because when we love someone, of course we want to fight their battles with them, if not for them. But if we want to be their rock of strength, we can’t get lost in it too, and of course that hurts.
Beatty takes us through these ideas and more, for example:
- How to examine our own feelings even when it’s scary
- How to practice self-love and regain self-worth, while still caring for them
- How to stop being reactionary, step back, and act with purpose
If the book has any weak point, it’s that it repeatedly recommends 12-step programs, when in reality that’s just one option. But for those who wish to take another approach, this book does not require involvement in a 12-step program, so it’s not a barrier to usefulness.
Click here to check out Codependent No More and take care of yourself, too
Share This Post
-

Statins: His & Hers?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Hidden Complexities of Statins and Cardiovascular Disease (CVD)

This is Dr. Barbara Roberts. She’s a cardiologist and the Director of the Women’s Cardiac Center at one of the Brown University Medical School teaching hospitals. She’s an Associate Clinical Professor of Medicine and takes care of patients, teaches medical students, and does clinical research. She specializes in gender-specific aspects of heart disease, and in heart disease prevention.
We previously reviewed Dr. Barbara Roberts’ excellent book “The Truth About Statins: Risks and Alternatives to Cholesterol-Lowering Drugs”. It prompted some requests to do a main feature about Statins, so we’re doing it today. It’s under the auspices of “Expert Insights” as we’ll be drawing almost entirely from Dr. Roberts’ work.
So, what are the risks of statins?
According to Dr. Roberts, one of the biggest risks is not just drug side-effects or anything like that, but rather, what they simply won’t treat. This is because statins will lower LDL (bad) cholesterol levels, without necessarily treating the underlying cause.
Imagine you got Covid, and it’s one of the earlier strains that’s more likely deadly than “merely” debilitating.
You’re coughing and your throat feels like you gargled glass.
Your doctor gives you a miracle cough medicine that stops your coughing and makes your throat feel much better.
(Then a few weeks later, you die, because this did absolutely nothing for the underlying problem)
You see the problem?
Are there problematic side-effects too, though?
There can be. But of course, all drugs can have side effects! So that’s not necessarily news, but what’s relevant here is the kind of track these side-effects can lead one down.
For example, Dr. Roberts cites a case in which a woman’s LDL levels were high and she was prescribed simvastatin (Zocor), 20mg/day. Here’s what happened, in sequence:
- She started getting panic attacks. So, her doctor prescribed her sertraline (Zoloft) (a very common SSRI antidepressant) and when that didn’t fix it, paroxetine (Paxil). This didn’t work either… because the problem was not actually her mental health. The panic attacks got worse…
- Then, while exercising, she started noticing progressive arm and leg weakness. Her doctor finally took her off the simvastatin, and temporarily switched to ezetimibe (Zetia), a less powerful nonstatin drug that blocks cholesterol absorption, which change eased her arm and leg problem.
- As the Zetia was a stopgap measure, the doctor put her on atorvastatin (Lipitor). Now she got episodes of severe chest pressure, and a skyrocketing heart rate. She also got tremors and lost her body temperature regulation.
- So the doctor stopped the atorvastatin and tried rosovastatin (Crestor), on which she now suffered exhaustion (we’re not surprised, by this point) and muscle pains in her arms and chest.
- So the doctor stopped the rosovastatin and tried lovastatin (Mevacor), and now she had the same symptoms as before, plus light-headedness.
- So the doctor stopped the lovastatin and tried fluvastatin (Lescol). Same thing happened.
- So he stopped the fluvastatin and tried pravastatin (Pravachol), without improvement.
- So finally he took her off all these statins because the high LDL was less deleterious to her life than all these things.
- She did her own research, and went back to the doctor to ask for cholestyramine (Questran), which is a bile acid sequestrent and nothing to do with statins. She also asked for a long-acting niacin. In high doses, niacin (one of the B-vitamins) raises HDL (good) cholesterol, lowers LDL, and lowers tryglycerides.
- Her own non-statin self-prescription (with her doctor’s signature) worked, and she went back to her life, her work, and took up running.
Quite a treatment journey! Want to know more about the option that actually worked?
Read: Bile Acid Resins or Sequestrants
What are the gender differences you/she mentioned?
Actually mostly sex differences, since this appears to be hormonal (which means that if your hormones change, so will your risk). A lot of this is still pending more research—basically it’s a similar problem in heart disease to one we’ve previously talked about with regard to diabetes. Diabetes disproportionately affects black people, while diabetes research disproportionately focuses on white people.
In this case, most heart disease research has focused on men, with women often not merely going unresearched, but also often undiagnosed and untreated until it’s too late. And the treatments, if prescribed? Assumed to be the same as for men.
Dr. Roberts tells of how medicine is taught:
❝When I was in medical school, my professors took the “bikini approach” to women’s health: women’s health meant breasts and reproductive organs. Otherwise the prototypical patient was presented as a man.❞
There has been some research done with statins and women, though! Just, still not a lot. But we do know for example that some statins can be especially useful for treating women’s atherosclerosis—with a 50% success rate, rather than 31% for men.
For lowering LDL itself, however, it can work but is generally not so hot in women.
Fun fact:
In men:
- High total cholesterol
- High non-HDL cholesterol
- High LDL cholesterol
- Low HDL cholesterol
…are all significantly associated with an increased risk of death from CVD.
In women:
…levels of LDL cholesterol even more than 190 were associated with only a small, statistically insignificant increased risk of dying from CVD.
So…
The fact that women derive less benefit from a medicine that mainly lowers LDL cholesterol, may be because elevated LDL cholesterol is less harmful to women than it is to men.
And also: Treatment and Response to Statins: Gender-related Differences
And for that matter: Women Versus Men: Is There Equal Benefit and Safety from Statins?*
Definitely a case where Betteridge’s Law of Headlines applies!
What should women do to avoid dying of CVD, then?
First, quick reminder of our general disclaimer: we can’t give medical advice and nothing here comprises such. However… One particularly relevant thing we found illuminating in Dr. Roberts’ work was this observation:
The metabolic syndrome is diagnosed if you have three (or more) out of five of the following:
- Abdominal obesity (waist >35″ if a woman or >40″ if a man)
- Fasting blood sugars of 100mg/dl or more
- Fasting triglycerides of 150mg/dl or more
- Blood pressure of 130/85 or higher
- HDL <50 if a woman or <40 if a man
And yet… because these things can be addressed with exercise and a healthy diet, which neither pharmaceutical companies nor insurance companies have a particular stake in, there’s a lot of focus instead on LDL levels (since there are a flock of statins that can be sold be lower them)… Which, Dr. Roberts says, is not nearly as critical for women.
So women end up getting prescribed statins that cause panic attacks and all those things we mentioned earlier… To lower our LDL, which isn’t nearly as big a factor as the other things.
In summary:
Statins do have their place, especially for men. They can, however, mask underlying problems that need treatment—which becomes counterproductive.
When it comes to women, statins are—in broad terms—statistically not as good. They are a little more likely to be helpful specifically in cases of atherosclerosis, whereby they have a 50/50 chance of helping.
For women in particular, it may be worthwhile looking into alternative non-statin drugs, and, for everyone: diet and exercise.
Further reading: How Can I Safely Come Off Statins?
Share This Post
Related Posts
-

When supplies resume, should governments subsidise drugs like Ozempic for weight loss? We asked 5 experts
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hundreds of thousands of people worldwide are taking drugs like Ozempic to lose weight. But what do we actually know about them? This month, The Conversation’s experts explore their rise, impact and potential consequences.
You’ve no doubt heard of Ozempic but have you heard of Wegovy? They’re both brand names of the drug semaglutide, which is currently in short supply worldwide.
Ozempic is a lower dose of semaglutide, and is approved and used to treat diabetes in Australia. Wegovovy is approved to treat obesity but is not yet available in Australia. Shortages of both drugs are expected to last throughout 2024.
Both drugs are expensive. But Ozempic is listed on Australia’s Pharmaceutical Benefits Schedule (PBS), so people with diabetes can get a three-week supply for A$31.60 ($7.70 for concession card holders) rather than the full price ($133.80).
Wegovy isn’t listed on the PBS to treat obesity, meaning when it becomes available, users will need to pay the full price. But should the government subsidise it?
Wegovy’s manufacturer will need to make the case for it to be added to the PBS to an independent advisory committee. The company will need to show Wegovy is a safe, clinically effective and cost-effective treatment for obesity compared to existing alternatives.
In the meantime, we asked five experts: when supplies resume, should governments subsidise drugs like Ozempic for weight loss?
Four out of five said yes
This is the last article in The Conversation’s Ozempic series. Read the other articles here.
Disclosure statements: Clare Collins is a National Health and Medical Research Council (NHMRC) Leadership Fellow and has received research grants from the National Health and Medical Research Council (NHMRC), the Australian Research Council (ARC), the Medical Research Future Fund (MRFF), the Hunter Medical Research Institute, Diabetes Australia, Heart Foundation, Bill and Melinda Gates Foundation, nib foundation, Rijk Zwaan Australia, the Western Australian Department of Health, Meat and Livestock Australia, and Greater Charitable Foundation. She has consulted to SHINE Australia, Novo Nordisk (for weight management resources and an obesity advisory group), Quality Bakers, the Sax Institute, Dietitians Australia and the ABC. She was a team member conducting systematic reviews to inform the 2013 Australian Dietary Guidelines update, the Heart Foundation evidence reviews on meat and dietary patterns and current co-chair of the Guidelines Development Advisory Committee for Clinical Practice Guidelines for Treatment of Obesity; Emma Beckett has received funding for research or consulting from Mars Foods, Nutrition Research Australia, NHMRC, ARC, AMP Foundation, Kellogg and the University of Newcastle. She works for FOODiQ Global and is a fat woman. She is/has been a member of committees/working groups related to nutrition or food, including for the Australian Academy of Science, the NHMRC and the Nutrition Society of Australia; Jonathan Karnon does not work for, consult, own shares in or receive funding from any company or organisation that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment; Nial Wheate in the past has received funding from the ACT Cancer Council, Tenovus Scotland, Medical Research Scotland, Scottish Crucible, and the Scottish Universities Life Sciences Alliance. He is a fellow of the Royal Australian Chemical Institute, a member of the Australasian Pharmaceutical Science Association and a member of the Australian Institute of Company Directors. Nial is the chief scientific officer of Vaihea Skincare LLC, a director of SetDose Pty Ltd (a medical device company) and a Standards Australia panel member for sunscreen agents. Nial regularly consults to industry on issues to do with medicine risk assessments, manufacturing, design and testing; Priya Sumithran has received grant funding from external organisations, including the NHMRC and MRFF. She is in the leadership group of the Obesity Collective and co-authored manuscripts with a medical writer provided by Novo Nordisk and Eli Lilly.
Fron Jackson-Webb, Deputy Editor and Senior Health Editor, The Conversation
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Princess of Wales wants to stay cancer-free. What does this mean?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Catherine, Princess of Wales, has announced she has now completed a course of preventive chemotherapy.
The news comes nine months after the princess first revealed she was being treated for an unspecified form of cancer.
In the new video message released by Kensington Palace, Princess Catherine says she’s focused on doing what she can to stay “cancer-free”. She acknowledges her cancer journey is not over and the “path to recovery and healing is long”.
While we don’t know the details of the princess’s cancer or treatment, it raises some questions about how we declare someone fully clear of the disease. So what does being – and staying – “cancer-free” mean?

Pete Hancock/Shutterstock What’s the difference between being cancer-free and in remission?
Medically, “cancer-free” means two things. First, it means no cancer cells are able to be detected in a patient’s body using the available testing methods. Second, there is no cancer left in the patient.
These might sound basically the same. But this second aspect of “cancer-free” can be complicated, as it’s essentially impossible to be sure no cancer cells have survived a treatment.
Testing can’t completely rule out the chance some cancer cells have survived treatment. Andrewshots/Shutterstock It only takes a few surviving cells for the cancer to grow back. But these cells may not be detectable via testing, and can lie dormant for some time. The possibility of some cells still surviving means it is more accurate to say a patient is “in remission”, rather than “cancer-free”.
Remission means there is no detectable cancer left. Once a patient has been in remission for a certain period of time, they are often considered to be fully “cancer-free”.
Princess Catherine was not necessarily speaking in the strict medical sense. Nonetheless, she is clearly signalling a promising step in her recovery.
What happens during remission?
During remission, patients will usually undergo surveillance testing to make sure their cancer hasn’t returned. Detection tests can vary greatly depending on both the patient and their cancer type.
Many tests involve simply looking at different organs to see if there are cancer cells present, but at varying levels of complexity.
Some cancers can be detected with the naked eye, such as skin cancers. In other cases, technology is needed: colonoscopies for colorectal cancers, X-ray mammograms for breast cancers, or CT scans for lung cancers. There are also molecular tests, which test for the presence of cancer cells using protein or DNA from blood or tissue samples.
For most patients, testing will continue for years at regular intervals. Surveillance testing ensures any returning cancer is caught early, giving patients the best chance of successful treatment.
Remaining in remission for five years can be a huge milestone in a patient’s cancer journey. For most types of cancer, the chances of cancer returning drop significantly after five years of remission. After this point, surveillance testing may be performed less frequently, as the patients might be deemed to be at a lower risk of their cancer returning.
Skin cancer may be detected by the naked eye, but many other cancers require technology for detection and monitoring. wavebreakmedia/Shutterstock Measuring survival rates
Because it is very difficult to tell when a cancer is “cured”, clinicians may instead refer to a “five-year survival rate”. This measures how likely a cancer patient is to be alive five years after their diagnosis.
For example, data shows the five-year survival rate for bowel cancer among Australian women (of all ages) is around 70%. That means if you had 100 patients with bowel cancer, after five years you would expect 70 to still be alive and 30 to have succumbed to the disease.
These statistics can’t tell us much about individual cases. But comparing five-year survival rates between large groups of patients after different cancer treatments can help clinicians make the often complex decisions about how best to treat their patients.
The likelihood of cancer coming back, or recurring, is influenced by many factors which can vary over time. For instance, approximately 30% of people with lung cancer develop a recurrent disease, even after treatment. On the other hand, breast cancer recurrence within two years of the initial diagnosis is approximately 15%. Within five years it drops to 10%. After ten, it falls below 2%.
These are generalisations though – recurrence rates can vary greatly depending on things such as what kind of cancer the patient has, how advanced it is, and whether it has spread.
Staying cancer-free
Princess Catherine says her focus now is to “stay cancer-free”. What might this involve?
How a cancer develops and whether it recurs can be influenced by things we can’t control, such as age, ethnicity, gender, genetics and hormones.
However, there are sometimes environmental factors we can control. That includes things like exposure to UV radiation from the sun, or inhaling carcinogens like tobacco.
Lifestyle factors also play a role. Poor diet and nutrition, a lack of exercise and excessive alcohol consumption can all contribute to cancer development.
Research estimates more than half of all cancers could potentially be prevented through regular screening and maintaining a healthy lifestyle (not to mention preventing other chronic conditions such as heart disease and diabetes).
Recommendations to reduce cancer risk are the same for everyone, not just those who’ve had treatment like Princess Catherine. They include not smoking, eating a nutritious and balanced diet, exercising regularly, cutting down on alcohol and staying sun smart.
Amali Cooray, PhD Candidate in Genetic Engineering and Cancer, WEHI (Walter and Eliza Hall Institute of Medical Research) ; John (Eddie) La Marca, Senior Research Officer, Blood Cells and Blood Cancer, WEHI (Walter and Eliza Hall Institute of Medical Research) , and Sarah Diepstraten, Senior Research Officer, Blood Cells and Blood Cancer Division, WEHI (Walter and Eliza Hall Institute of Medical Research)
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

As The Summer Gets Hotter Still…
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I would love to see an article about heat dehydrated illness….so much of the US is under hot conditions. I had an fainting sweating episode and now trying to recoup from it. What should we do? Drink water,rest…???❞
We have done some of this, but it’s always a good one to revisit! Last summer (N. Hemisphere summer), we wrote this:
Stay Safe From Heat Exhaustion & Heatstroke!
…and this year, it’s getting hotter still (and is already the hottest summer on record), with certainly much of the US seriously affected, as you say. Next year, it will probably be worse again; climate change is getting predictable like that, and likely will continue until fixed. We are but a health science publication, so we can’t fix the world’s climate, but we can reiterate the above advice, and urge everyone to take it seriously.
Note: heat exhaustion and heatstroke kill. Yes, we’re including heat exhaustion in that, because by the time you get heat exhaustion, you’re often not in the best state of mind to take the correct steps to avoid the heatstroke that follows.
To think otherwise would be akin to thinking “falling never killed anyone; it’s only when you stop falling that it’s dangerous”.
This summer, we did also write this more niche article:
…whose advice won’t apply to everyone, but will be helpful to some, and honestly, some of that advice does go for everyone.
One thing we didn’t write about in those articles that we’ll add here:
Humidity is dangerous:
- Dry heat: you sweat, the sweat evaporates, cooling you. As well as losing heat, you’ve also now lost water and salts, which you’ll need to replenish, but your body is operating correctly.
- Humid heat: you sweat, and now you are just sweaty until further notice. It doesn’t evaporate because the surrounding humidity doesn’t provide the physics for that. Not only are you not losing heat through evaporating sweat, but also, if you’re wearing clothes, that’s now an insulating layer you’re wearing.
…so that means, watch the humidity as carefully as you watch the temperature, and when it’s high, get extra serious about finding ways to keep yourself cool (e.g. shade, rest, cooling showers etc if you can, that kind of thing).
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: