Eye Drops: Safety & Alternatives
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Before important business meetings my father used to use eye drops to add a “sparkle” to his eyes. I think that is a step too far, but what, short of eye drops, can we do to keep our eyes bright throughout the day?❞
Firstly, we’d indeed not recommend eye drops unless advised to do so by your doctor to treat a specific health condition:
- Infections from over-the-counter artificial tears
- Are my eye drops safe to use?
- More eye drops recalled due to infection danger
Those eye drops that “add sparkle” are often based on astringents such as witch hazel. This means that the capillaries in the eye undergo vasoconstriction, becoming much less visible and the eye thus appears much whiter and thus brighter.
There isn’t a way to do the same thing from the inside, as taking a vasoconstrictor will simply increase your general blood pressure, making the capillaries of your eyes more, rather than less, visible.
However, what you can do is…
- look after your general vasculature (cardiovascular health)
- in particular, reduce hypertension
- that includes limiting salt
- stay away from vasoconstrictors (including caffeine)
- reduce your resting cortisol levels
- that certainly also means reducing alcohol consumption
- maintain good hydration
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Q&A with the 10almonds Team
Q: Very interested in this article on CBD oil in the states. hope you do another one in the future with more studies done on people and more information on what’s new as far as CBD oil goes
A: We’re glad you enjoyed it! We’ll be sure to revisit CBD in the future—partly because it was a very popular article, and partly because, as noted, there is a lot going on there, research-wise!
And yes, we prefer human studies rather than mouse/rat studies where possible, too, and try to include those where we find them. In some cases, non-human animal studies allow us to know things that we can’t know from human studies… because a research institution’s ethics board will greenlight things for mice that it’d never* greenlight for humans.
Especially: things that for non-human animals are considered “introduction of external stressors” while the same things done to humans would be unequivocally called “torture”.
Animal testing in general is of course a moral quagmire, precisely because of the suffering it causes for animals, while the research results (hopefully) can be brought to bear to reduce to suffering of humans. We’re a health and productivity newsletter, not a philosophical publication, but all this to say: we’re mindful of such too.
And yes, we agree, when studies are available on humans, they’re always going to be better than the same study done on mice and rats.
As a topical aside, did you know there’s a monument to laboratory mice and all they’ve (however unintentionally) done for us?
❝The quirky statue depicts an anthropomorphic mouse as an elderly woman, complete with glasses balanced atop its nose. Emerging from two knitting needles in its hands is the recognizable double-helix of a strand of DNA.❞
~ Smithsonian Magazine
Share This Post
-

Amid Wildfire Trauma, L.A. County Dispatches Mental Health Workers to Evacuees

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
PASADENA, Calif. — As Fernando Ramirez drove to work the day after the Eaton Fire erupted, smoke darkened the sky, ash and embers rained onto his windshield, and the air smelled of melting rubber and plastic.
He pulled to the side of the road and cried at the sight of residents trying to save their homes.
“I could see people standing on the roof, watering it, trying to protect it from the fire, and they just looked so hopeless,” said Ramirez, a community outreach worker with the Pasadena Public Health Department.
That evening, the 49-year-old volunteered for a 14-hour shift at the city’s evacuation center, as did colleagues who had also been activated for emergency medical duty. Running on adrenaline and little sleep after finding shelter for homeless people all day, Ramirez spent the night circulating among more than a thousand evacuees, offering wellness checks, companionship, and hope to those who looked distressed.
Local health departments, such as Ramirez’s, have become a key part of governments’ response to wildfires, floods, and other extreme weather events, which scientists say are becoming more intense and frequent due to climate change. The emotional toll of fleeing and possibly losing a home can help cause or exacerbate mental health conditions such as anxiety, depression, post-traumatic stress disorder, suicidal ideation, and substance use, according to health and climate experts.
Wildfires have become a recurring experience for many Angelenos, making it difficult for people to feel safe in their home or able to go about daily living, said Lisa Wong, director of the Los Angeles County Department of Mental Health. However, with each extreme weather event, the county has improved its support for evacuees, she said.
For instance, Wong said the county deployed a team of mental health workers trained to comfort evacuees without retraumatizing them, including by avoiding asking questions likely to bring up painful memories. The department has also learned to better track people’s health needs and redirect those who may find massive evacuation settings uncomfortable to other shelters or interim housing, Wong said. In those first days, the biggest goal is often to reduce people’s anxiety by providing them with information.
“We’ve learned that right when a crisis happens, people don’t necessarily want to talk about mental health,” said Wong, who staffed the evacuation site Jan. 8 with nine colleagues.
Instead, she and her team deliver a message of support: “This is really bad right now, but you’re not going to do this alone. We have a whole system set up for recovery too. Once you get past the initial shock of what happened — initial housing needs, medication needs, all those things — then there’s this whole pathway to recovery that we set up.”
The convention center in downtown Pasadena, which normally hosts home shows, comic cons, and trade shows, was transformed into an evacuation site with hundreds of cots. It was one of at least 13 shelters opened to serve more than 200,000 residents under evacuation orders.
The January wildfires have burned an estimated 64 square miles — an area larger than the city of Paris — and destroyed at least 12,300 buildings since they started Jan. 7. AccuWeather estimates the region will likely face more than $250 billion in economic losses from the blazes, surpassing the estimates from the state’s record-breaking 2020 wildfire season.
Lisa Patel, executive director of the Medical Society Consortium on Climate and Health, said she’s most concerned about low-income residents, who are less likely to access mental health support.
“There was a mental health crisis even before the pandemic,” said Patel, who is also a clinical associate professor of pediatrics at Stanford School of Medicine, referring to the covid-19 pandemic. “The pandemic made it worse. Now you lace in all of this climate change and these disasters into a health care system that isn’t set up to care for the people that already have mental health illness.”
Early research suggests exposure to large amounts of wildfire smoke can damage the brain and increase the risk of developing anxiety, she added.
At the Pasadena Convention Center, Elaine Santiago sat on a cot in a hallway as volunteers pulled wagons loaded with soup, sandwiches, bottled water, and other necessities.
Santiago said she drew comfort from being at the Pasadena evacuation center, knowing that she wasn’t alone in the tragedy.
“It sort of gives me a sense of peace at times,” Santiago said. “Maybe that’s weird. We’re all experiencing this together.”
She had been celebrating her 78th birthday with family when she fled her home in the small city of Sierra Madre, east of Pasadena. As she watched flames whip around her neighborhood, she, along with children and grandkids, scrambled to secure their dogs in crates and grabbed important documents before they left.
The widower had leaned on her husband in past emergencies, and now she felt lost.
“I did feel helpless,” Santiago said. “I figured I’m the head of the household; I should know what to do. But I didn’t know.”
Donny McCullough, who sat on a neighboring green cot draped in a Red Cross blanket, had fled his Pasadena home with his family early on the morning of Jan. 8. Without power at home, the 68-year-old stayed up listening for updates on a battery-powered radio. His eyes remained red from smoke irritation hours later.
“I had my wife and two daughters, and I was trying not to show fear, so I quietly, inside, was like, ‘Oh my God,’” said McCullough, a music producer and writer. “I’m driving away, looking at the house, wondering if it’s going to be the last time I’m going to see it.”
He saved his master recording from a seven-year music project, but he left behind his studio with all his other work from a four-decade career in music.
Not all evacuees arrived with family. Some came searching for loved ones. That’s one of the hardest parts of his shift, Ramirez said. The community outreach worker helped walk people around the building, cot by cot.
A week in, at least two dozen people had been killed in the wildfires.
The work takes a toll on disaster relief workers too. Ramirez said many feared losing their homes in the fires and some already had. He attends therapy weekly, which he said helps him manage his emotions.
At the evacuation center, Ramirez described being on autopilot.
“Some of us react differently. I tend to go into fight mode,” Ramirez said. “I react. I run towards the fire. I run towards personal service. Then once that passes, that’s when my trauma catches up with me.”
Need help? Los Angeles County residents in need of support can call the county’s mental health helpline at 1-800-854-7771. The national Suicide & Crisis Lifeline, 988, is also available for those who’d like to speak with someone confidentially, free of charge.
This article was produced by KFF Health News, which publishes California Healthline, an editorially independent service of the California Health Care Foundation.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Share This Post
-
Breast Milk’s Benefits That Are (So Far) Not Replicable
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Simply The Breast 🎶

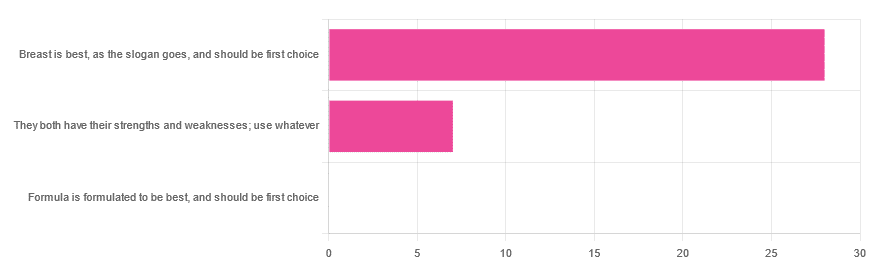
In Wednesday’s newsletter, we asked you for your opinion on breast vs formula milk (for babies!), and got the above-depicted, below-described, set of responses:
- 80% said “Breast is best, as the slogan goes, and should be first choice”
- 20% said “They both have their strengths and weaknesses; use whatever”
- 0% said “Formula is formulated to be best, and should be first choice”
That’s the first time we’ve ever had a possible poll option come back with zero votes whatsoever! It seems this topic is relatively uncontentious amongst our readership, so we’ll keep things brief today, but there is still a little mythbusting to be done.
So, what does the science say?
[Breast milk should be the first choice] at least for the few few weeks and months for the benefit of baby’s health as breast milk has protective factors formula does not: True or False?
True! The wording here was taken from one of our readers’ responses, by the way (thank you, Robin). There are a good number of those protective factors, the most well-known of which is passing on immune cells and cell-like things; in other words, immune-related information being passed from parent* to child.
*usually the mother, though in principle it could be someone else and in practice sometimes it is; the only real requirements are that the other person be healthy, lactating, and willing.
As for immune benefits, see for example:
Perspectives on Immunoglobulins in Colostrum and Milk
And for that matter, also:
(Colostrum is simply the milk that is produced for a short period after giving birth; the composition of milk will tend to change later)
In any case, immunoglobulin A is a very important component in breast milk (colostrum and later), as well as lactoferrin (has an important antimicrobial effect and is good for the newborn’s gut), and a plethora of cytokines:
As for that about the gut, lactoferrin isn’t the only breast milk component that benefits this, by far, and there’s a lot that can’t be replicated yet:
Human Breast Milk and the Gastrointestinal Innate Immune System
As long as your infant/child is nutritiously fed, it shouldn’t matter if it comes from breast or formula: True or False?
False! Formula milk will not convey those immune benefits.
This doesn’t mean that formula-feeding is neglectful; as several people who commented mentioned*, there are many reasons a person may not be able to breastfeed, and they certainly should not be shamed for that.
*(including the reader whose words we borrowed for this True/False item; the words we quoted above were prefaced with: “Not everyone is able to breastfeed for many different reasons”)
But, while formula milk is a very good second choice, and absolutely a respectable choice if breast milk isn’t an option (or an acceptable option) for whatever reason, it still does not convey all the health benefits of breast milk—yet! The day may come when they’ll find a way to replicate the immune benefits, but today is not that day.
They both have their strengths and weaknesses: True or False?
True! But formula’s strengths are only in the category of convenience and sometimes necessity—formula conveys no health benefits that breast milk could not do better, if available.
For many babies, formula means they get to eat, when without it they would starve due to non-availability of breast milk. That’s a pretty important role!
Note also: this is a health science publication, not a philosophical publication, but we’d be remiss not to mention one thing; let’s bring it in under the umbrella of sociology:
The right to bodily autonomy continues to be the right to bodily autonomy even if somebody else wants/needs something from your body.
Therefore, while there are indeed many good reasons for not being able to breastfeed, or even just not being safely* able to breastfeed, it is at the very least this writer’s opinion that nobody should be pressed to give their reason for not breastfeeding; “no” is already a sufficient answer.
*Writer’s example re safety: when I was born, my mother was on such drugs that it would have been a very bad idea for her to breastfeed me. There are plenty of other possible reasons why it might be unsafe for someone one way or another, but “on drugs that have a clear ‘do not take while pregnant or nursing’ warning” is a relatively common one.
All that said, for those who are willing and safely able, the science is clear: breast is best.
Want to read more?
The World Health Organization has a wealth of information (including explanations of its recommendations of, where possible, exclusive breastfeeding for the first 6 months, ideally continuing some breastfeeding for the first 2 years), here:
World Health Organization | Breastfeeding
Take care!
Share This Post



Related Posts
-

Take This Two-Minute Executive Dysfunction Test
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Roll For Initiative
Some of us struggle with executive dysfunction a lot; others, a little.
What Is Executive Dysfunction?
• Executive function is a broad group of mental skills that enable people to complete tasks and interact with others.
• Executive dysfunction can impair a person’s ability to organize and manage behavior
• Executive dysfunction is not a specific stand-alone diagnosis or condition.
• Instead, conditions such as depression and ADHD (amongst others) can affect a person’s executive function.
Take This Two-Minute Executive Dysfunction Test
How did you score? (8/16 here!)
Did you do it? (it honestly is really two minutes and is quite informative)
If not, here’s your cue to go back up and do it
For almost all of us, we sometimes find ourselves torn between several competing tasks, and end up doing… none of them.
For such times, compile yourself a “productivity buffet”, print it, and pin it above your desk or similar space.
What’s a productivity buffet?
It’s a numbered list of 6, 8, 10, 12 or 20 common tasks that pretty much always need doing (to at least some extent!). Doesn’t matter how important they are, just that they are frequently recurring tasks. For example:
- Tidy desk (including that drawer!)
- Reply to emails/messages
- Drink water
- Collect stray one-off to-dos into a list
- Stretch (or at least correct your posture!)
- Extend that Duolingo streak
- Read one chapter of a book
- Etc
Why 6, 8, 10, 12, or 20?
Because those are common denominations of polyhedral dice that are very cheap to buy!
Keep the relevant die to hand (perhaps in your pocket or on your desk), and when you know you should be doing something but can’t decide what exactly, roll the die and do the item corresponding to the number you roll.
And if you find yourself thinking “damn, I got 12, I wanted 7!” then go ahead and do item 7—the dice aren’t the boss of you, they’re just there to break the ice between you and your to-do list!
The Housekeeper In Your Pocket?
If you found the tidying tips (up top) helpful, but don’t like cleaning schedules because you just can’t stick to them, this one’s for you.
It’s easy to slip into just doing the same few easy tasks while neglecting others for far too long.
The answer? Outsource!
Not “get a cleaner” (though if you want to and can, great, go for it, this one won’t be for you after all), but rather, try this nifty little app that helps you keep on top of daily cleaning—which we all know is better than binge-cleaning every few months.
Sweepy keeps track of:
- What jobs there are that might need doing in each room (or type of room) in the house
- How often those jobs generally need doing
- How much of your energy (a finite resource, which it also takes into account!) those jobs will take
- How much energy you are prepared to spend per day (you can “lighter/heavier” days, or even “off-days”, too)
…and then it populates a small daily task list according to what needs cleaning and how much energy it’ll take.
For example, today Sweepy gives me (your trusty writer, hi! ) the tasks:
- Bathroom: clean sink (every 3 days, 1pt of energy)
- Dining room: clean and tidy table (every day, 1pt of energy)
- Bedroom: vacuum floor (every 7 days, 2pts of energy)
- Kitchen: clean coffee machine (every 30 days, 2pts of energy)
And that’s my 6pts of energy I’ve told Sweepy I’m happy to spend per day cleaning. There are “3 pts” tasks too—cleaning the oven, for example—but none came up today.
Importantly: it does not bother me about any other tasks today (even if something’s overdue), and I don’t have to worry my pretty head about it.
I don’t have to feel guilty for not doing other cleaning tasks; if they need doing, Sweepy will tell me tomorrow, and it will make sure I don’t get behind or leave anything neglected for too long.
Check it out (available for both iOS and Android)
PS: to premium or not to premium? We think the premium is worth it (unlocks some extra customization features) but the free version is sufficient to get your house in order, so don’t be afraid to give it a try first.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Mythbusting Moldy Food
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Most Food Should Not Be Fuzzy
In yesterday’s newsletter, we asked you for your policy when it comes to mold on food (aside from intentional mold, e.g. blue cheese etc), and the responses were interesting:
- About 49% said “throw the whole thing away no matter what it is; it is dangerous”
- About 24% said “cut the mold off and eat the rest of whatever it is”
- The remainder were divided equally between “eat it all; keep the immune system on its toes” and “cut the mold off bread, but moldy animal products are dangerous”
So what does the science say?
Some molds are safe to eat: True or False?
True! We don’t think this is contentious so we’ll not spend much time on it, but just for the sake of being methodical: foods that are supposed to have mold on, including many kinds of cheese and even some kinds of cured meat (salami is an example; that powdery coating is mold).
We could give a big list of safe and unsafe molds, but that would be a list of names and let’s face it, they don’t introduce themselves by name.
However! The litmus test of “is it safe to eat” is:
Did you acquire it with this mold already in place and exactly as expected and advertised?
- If so, it is safe to eat (unless you have an allergy or such)
- If not, it is almost certainly not safe to eat
(more on why, later)
The “sniff test” is a good way to tell if moldy food is bad: True or False?
False. Very false. Because of how the sense of smell works.
You may feel like smell is a way of knowing about something at a distance, but the only way you can smell something is if particles of it are physically connecting with your olfactory receptors inside you. Yes, that has unfortunate implications about bathroom smells, but for now, let’s keep our attention in the kitchen.
If you sniff a moldy item of food, you will now have its mold spores inside your respiratory system. You absolutely do not want them there.
If we cut off the mold, the rest is safe to eat: True or False?
True or False, depending on what it is:
- Hard vegetables (e.g carrots, cabbage), and hard cheeses (e.g. Gruyère, Gouda) – cut off with an inch margin, and it should be safe
- Soft vegetables (e.g. tomatoes, and any vegetables that were hard but are now soft after cooking) – discard entirely; it is unsafe
- Anything else – discard entirely; it is unsafe
The reason for this is because in the case of the hard products mentioned, the mycelium roots of the mold cannot penetrate far.
In the case of the soft products mentioned, the surface mold is “the tip of the iceberg”, and the mycelium roots, which you will not usually be able to see, will penetrate the rest of it.
“Anything else” seems like quite a sweeping statement, but fruits, soft cheeses, yogurt, liquids, jams and jellies, cooked grains and pasta, meats, and yes, bread, are all things where the roots can penetrate deeply and easily. Regardless of you only being able to see a small amount, the whole thing is probably moldy.
The USDA has a handy downloadable factsheet:
Molds On Food: Are They Dangerous?
Eating a little mold is good for the immune system: True or False?
False, generally. There are of course countless types of mold, but not only are many of them pathogenic (mycotoxins), but also, a food that has mold will usually also have pathogenic bacteria along with the mold.
See for example: Occurrence, Toxicity, and Analysis of Major Mycotoxins in Food
Food poisoning will never make you healthier.
But penicillin is safe to eat: True or False?
False, and also penicillin is not the mold on your bread (or other foods).
Penicillin, an antibiotic* molecule, is produced by some species of Penicillium sp., a mold. There are hundreds of known species of Penicillium sp., and most of them are toxic, usually in multiple ways. Take for example:
Penicillium roqueforti PR toxin gene cluster characterization
*it is also not healthy to consume antibiotics unless it is seriously necessary. Antibiotics will wipe out most of your gut’s “good bacteria”, leaving you vulnerable. People have died from C. diff infections for this reason. So obviously, if you really need to take antibiotics, take them as directed, but if not, don’t.
See also: Four Ways Antibiotics Can Kill You
One last thing…
It may be that someone reading this is thinking “I’ve eaten plenty of mold, and I’m fine”. Or perhaps someone you tell about this will say that.
But there are two reasons this logic is flawed:
- Survivorship bias (like people who smoke and live to 102; we just didn’t hear from the 99.9% of people who smoke and die early)
- Being unaware of illness is not being absent of illness. Anyone who’s had an alarming diagnosis of something that started a while ago will know this, of course. It’s also possible to be “low-level ill” often and get used to it as a baseline for health. It doesn’t mean it’s not harmful for you.
Stay safe!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Healing Arthritis – by Dr. Susan Blum
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We previously reviewed another book by this author, her Immune System Recovery Plan, and today it’s more specific: healing arthritis
Of course, not all arthritis is rooted in immune dysfunction, but a) all of it is made worse by immune dysfunction and b) rheumatoid arthritis, which is an autoimmune disease, affects 1% of the population.
This book tackles all kinds of arthritis, by focusing on addressing the underlying causes and treating those, and (whether it was the cause or not) reducing inflammation without medication, because that will always help.
The “3 steps” mentioned in the subtitle are three stages of a plan to improve the gut microbiome in such a way that it not only stops worsening your arthritis, but starts making it better.
The style here is on the hard end of pop-science, so if you want something more conversational/personable, then this won’t be so much for you, but if you just want the information and explanation, then this does it just fine, and it has frequent references to the science to back it up, with a reassuringly extensive bibliography.
Bottom line: if you have arthritis and want a book that will help you to get either symptom-free or as close to that as is possible from your current condition (bearing in mind that arthritis is generally degenerative), then this is a great book for that.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: