Eradicating mould would save millions in health-care costs: how our homes affect our health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Housing is a key determinant of physical health. Housing conditions can increase or reduce the risk of problems including respiratory illness, heart disease and injury.
Improving housing conditions would see an improvement in health at the population level and reduce health-care costs.
In a study yet to be peer-reviewed, our research team has estimated eradicating mould and damp in Australian housing could cut health expenditure by A$117 million per million people, and increase income by $174 million. These figures represent 0.5%–2.1% of annual health spending and 0.08%–0.36% of gross domestic product.
We also estimated tackling mould and damp could result in an extra 4,190 health-adjusted life years (the number of years a person can expect to live in good health) per million people over 20 years. This is equivalent to about 1.5 healthy days per person. We’d see the greatest gains among people who are most disadvantaged.
In Australia and several similar countries, the conditions and location of many people’s homes are heavily influenced by housing affordability and the failure of successive governments to treat housing as a human right. Instead, it’s often been treated as a wealth-generating asset.
But it’s time to change things. The significant effects of poor housing on health, and a growing body of evidence indicating healthier homes could lead to tangible improvements, build a strong case for prioritising healthy housing policy in Australia.

Respiratory health
Numerous studies have established strong links between poor housing quality and increased risk of respiratory issues.
Exposure to damp, mould and poor ventilation in homes has consistently been associated with higher rates of asthma, allergies and other respiratory conditions, particularly among children and vulnerable groups.
Cold and poorly insulated homes can exacerbate respiratory symptoms. Meanwhile, overcrowding may make it easier for respiratory infections to spread.
Indoor air pollutants, from sources such as building materials and inappropriate heating systems, can further compromise lung function and respiratory health.
On the flip side, interventions to improve housing conditions – such as enhancing insulation, reducing dampness and improving ventilation – can positively affect respiratory health.
For instance, studies have shown retrofitting homes with proper insulation can lead to significant reductions in asthma symptoms and hospital admissions for respiratory conditions.
Heart health
The conditions and location of housing are also linked to cardiovascular health (for example, blood pressure) and metabolic health conditions such as diabetes and obesity.
Cold and damp housing conditions can increase the risk of disease through their effect on blood pressure. Exposure to low indoor temperatures can lead to high blood pressure, a major risk factor for conditions including heart disease, stroke and type 2 diabetes.
Poor insulation and energy inefficiency can exacerbate these effects, especially in regions with cold climates or during winter months.
Conversely, changes to housing that make temperatures more comfortable – such as installing insulation or efficient heating and cooling systems – could reduce disease risk.
For example, studies have shown reductions in blood pressure and fewer hospital admissions following interventions designed to warm homes.
Where we live also matters. For instance, the location of our home determines how much we’re exposed to air pollution – a risk factor for a range of diseases.
Access to green spaces and places to exercise near home is linked to reduced risk of diabetes, obesity and cardiovascular disease.
Injuries
Poor housing conditions can increase the risk of injuries such as falls and burns.
Inadequate lighting, uneven flooring, and poorly maintained or constructed stairs are common hazards that increase the risk of falls, especially among older adults. What’s more, the absence of proper accessibility features in homes can lead to increased risk of injuries among people with disabilities.
Studies have shown low-cost housing modifications – such as installing grab bars and handrails, improving lighting and childproofing measures – can markedly reduce injury rates.
Faulty electrical wiring and inadequate fire safety measures, such as the absence of smoke detectors, increase the risk of injuries and deaths. When New South Wales made smoke alarms compulsory in all homes in 2006, hospitalisation rates for residential fire injuries decreased by an estimated 36% annually.
But there’s variation in smoke alarm legislation across different Australian jurisdictions. And challenges remain with enforcement and ensuring alarms are functional.
Failing to act will cost us
Lower-income households, and especially renters, are at higher risk of the health consequences of poor housing. This contributes to health inequities across society.
In a new paper published in The Lancet Public Health, we present housing as a key social determinant of health. We highlight how affordability, security and suitability of housing shape health and wellbeing.
At the same time, our recent modelling and other research internationally provide compelling evidence that improving housing could have substantial benefits.
These models consistently show targeting mould, damp and cold in housing not only improve health outcomes, but also offer significant economic gains. This positions housing improvement as a cost-effective public health strategy.
As well as interventions to directly improve housing conditions for the homes that most need it, we also need structural reform of our housing systems. We must ensure everyone has access to an affordable, secure and suitable home.
This article is part of a series, Healthy Homes.
Rebecca Bentley, Professor of Social Epidemiology and Director of the Centre of Research Excellence in Healthy Housing at the Melbourne School of Population and Global Health, The University of Melbourne and Kate Mason, Senior Research Fellow, Melbourne School of Population and Global Health, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

This Week In Brain News

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
While reading this week’s health news, we’ve singled out three brain-related articles to feature here:
Bad breath now, bad brain later?
Researchers found links between oral microbiome populations, and changes in brain function with aging. The short version is indeed “bad breath now = bad brain later”, but more specifically:
- People who had large numbers of the bacteria groups Neisseria and Haemophilus had better memory, attention and ability to do complex tasks
- People who had higher levels of Porphyromonas had more memory problems later
- People with a lot of Prevotella tended to predict poorer brain health and was more common in people who carry the Alzheimer’s Disease risk gene, APOE4.
If you’ve never heard of half of those, don’t worry: mostly your oral microbiome can take care of itself, provide you consistently do the things that create a “good” oral microbiome. So, see our “related” link below:
Read in full: Mouth bacteria may hold insight into your future brain function
Related: Improve Your Oral Microbiome
Weeding out a major cause of cognitive decline
Cannabis may be great for relaxation, but regular use is not great for mental sharpness, and recent use (even if not regular, and even if currently sober) shows a similar dip in cognitive abilities, especially working memory. In other words, cannabis use for relaxation should be at most an occasional thing, rather than an everyday thing.
While the results of the study are probably not shocking, something that we found interesting was their classification system:
❝Heavy users are considered young adults who’ve used cannabis more than 1000 times over their lifetime. Whereas, using 10 to 999 times was considered a moderate user, and fewer than 10 times was considered a non-user.❞
Which—while being descriptive rather than prescriptive in nature—suggests that, to be on the healthy end of the bell curve, an occasional cannabis-user might want to consider “if you have 999 uses before you hit the “heavy user” category, project those 999 uses against your life expectancy, and moderate your use accordingly”. In other words, a person just now starting use, who expects to live another 40 years, would calculate: 999/40 = 24.9 uses per year, so call it 2 per month. A person who only expects to live another 20 years, would do the same math and arrive at 4 per month.
Disclaimer: the above is intended as an interesting reframe, and a way of looking at long-term cannabis use while being mindful of the risks. It is not intended as advice. This health-conscious writer personally has no intention of using at all, unless perhaps in some bad future scenario in which I have bad chronic pain, I might consider that pain relief effects may be worth the downsides. Or I might not; I hope not to be in the situation to find out!
Read in full: Largest study ever done on cannabis and brain function finds impact on working memory
Related: Cannabis Myths vs Reality
Mind-reading technology improves again
We’ve come quite a way from simple 1/0 reads, and basic cursor control! Now, researchers have created a brain decode that can translate a person’s thoughts into continuous text, without requiring the person to focus on words—in other words, it verbalizes the ideas directly. Most recently, the latest upgrade means that while previously, the device had to be trained on an individual brain for many hours, now the training/calibration process takes only an hour:
Read in full: Improved brain decoder holds promise for communication in people with aphasia
Related: Are Brain Chips Safe?
Take care!
Share This Post
-

Apple Cider Vinegar vs Apple Cider Vinegar Gummies – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apple cider vinegar (bottled) to apple cider vinegar (gummies), we picked the bottled.
Why?
There are several reasons!
The first reason is about dosage. For example, the sample we picked for apple cider vinegar gummies, boasts:
❝2 daily chewable gummies deliver 800 mg of Apple Cider Vinegar a day, equivalent to a teaspoon of liquid apple cider vinegar❞
That sounds good until you note that it’s recommended to take 1–2 tablespoons (not teaspoons) of apple vinegar. So this would need more like 4–8 gummies to make the dose. Suddenly, either that bottle of gummies is running out quickly, or you’re just not taking a meaningful dose and your benefits will likely not exceed placebo.
The other is reason about sugar. Most apple cider vinegar gummies are made with some kind of sugar syrup, often even high-fructose corn syrup, which is one of the least healthy foodstuffs (in the loosest sense of the word “foodstuffs”) known to science.
The specific brand we picked today was the best we can find; it used maltitol syrup.
Maltitol syrup, a corn derivative (and technically a sugar alcohol), has a Glycemic Index of 52, so it does raise blood sugars but not as much as sucrose would. However (and somewhat counterproductive to taking apple cider vinegar for gut health) it can cause digestive problems for many people.
And remember, you’re taking 4–8 gummies, so this is amounting to several tablespoons of the syrup by now.
On the flipside, apple cider vinegar itself has two main drawbacks, but they’re much less troublesome issues:
- many people don’t like the taste
- its acidic nature is not good for teeth
To this the common advice for both is to dilute it with water, thus diluting the taste and the acidity.
(this writer shoots hers from a shot glass, thus not bathing the teeth since it passes them “without touching the sides”; as for the taste, well, I find it invigorating—I do chase it with water, though to be sure of not leaving vinegar in my mouth)
Want to check them out for yourself?
Here they are:
Apple cider vinegar | Apple cider vinegar gummies
Want to know more about apple cider vinegar?
Check out:
- An Apple (Cider Vinegar) A Day…
- 10 Ways To Balance Blood Sugars
- How To Recover Quickly From A Stomach Bug
Take care!
Share This Post
-
Mini Cuts: How To Lose Fat Quickly & Safely
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
No, one cannot healthily do this long-term. But for a few weeks to quickly drop fat while preserving lean muscle, yes:
Briefly does it
Step by step, the process goes like this:
- prep before starting: eat at maintenance for 1–2 weeks; set a clear goal (perhaps you have a vacation or event in mind that you want to look a certain way for).
- set calorie target: calculate maintenance calories; and subtract 300–500 for your mini cut. If unsure, use goal bodyweight in pounds ×10.
- set macro ratios: week 1 use 45% protein, 25% carbs, 30% fat; week 2 use 50% protein, 30% carbs, 20% fat; track as accurately as you reasonably can.
- plan and prep meals: batch-prep simple, repetitive meals (this makes tracking easier), with a focus on lean proteins, vegetables, fruits, and other high-volume foods to improve satiety.
- training adjustments: keep your strength training consistent; consider a small carb snack pre-workout if you usually train fasted, and avoid excessive cardio.
- remember to end the mini cut: per the first step, the duration should be 7–14 days (absolute maximum 30).
- reverse out: increase calories gradually by around 100 kcal per day until it’s back to the maintenance levels; you can reduce protein to 30–40% as carbs and fats normalize. then stay at maintenance for at least another 1–2 weeks before considering another deficit phase if you still want to lose more fat.
- reflect and reset: assess your results (body composition, energy, performance); treat mini cuts as a tool, not a lifestyle; returning to balanced eating is important for sustainability and general health.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
How To Lose Weight (Healthily!) ← for a more sustainable approach; honestly we recommend this much more
Take care!
Share This Post


-
Natto vs Tofu – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing nattō to tofu, we picked the nattō.
Why?
In other words, in the comparison of fermented soy to fermented soy, we picked the fermented soy. But the relevant difference here is that nattō is fermented whole soybeans, while tofu is fermented soy milk of which the coagulated curds are then compressed into a block—meaning that the nattō is the one that has “more food per food”.
Looking at the macros, it’s therefore no surprise that nattō has a lot more fiber to go with its higher carb count; it also has slightly more protein. You may be wondering what tofu has more of, and the answer is: water.
In terms of vitamins, nattō has more of vitamins B2, B4, B6, C, E, K, and choline, while tofu has more of vitamins A, B3, and B9. So, a 7:3 win for nattō, even before considering that that vitamin C content of nattō is 65x more than what tofu has.
When it comes to minerals, nattō has more copper, iron, magnesium, manganese, potassium, and zinc, while tofu has more calcium, phosphorus, and selenium. So, a 6:3 win for nattō, and yes, the margins of difference are comparable (being 2–3x more for most of these minerals).
In short, both of these foods are great, but nattō is better.
Want to learn more?
You might like to read:
21% Stronger Bones in a Year at 62? Yes, It’s Possible (No Calcium Supplements Needed!)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Perfectionism, And How To Make Yours Work For You
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Harness The Power Of Your Perfectionism
A lot of people see perfectionism as a problem—and it can be that!
We can use perfectionism as a would-be shield against our fear of failure, by putting things off until we’re better prepared (repeat forever, or at least until the deadliniest deadline that ever deadlined), or do things but really struggle to draw a line under them and check them off as “done” because we keep tweaking and improving and improving… With diminishing returns (forever). So, that’s not helpful.
But, if we’re mindful, we can also leverage our perfectionism to our benefit.
Great! How?
First we need to be able to discern the ways in which perfectionism can be bad or good for us. Or as it’s called in psychology, ways in which our perfectionism can be maladaptive or adaptive.
- Maladaptive: describing a behavioral adaptation to our environment—specifically, a reactive behavioral adaptation that is unhealthy and really is not a solution to the problem at hand
- Adaptive: describing a behavioral adaptation to our environment—specifically, a responsive behavioral adaptation that is healthy and helps us to thrive
So in the case of perfectionism, one example for each might be:
- Maladaptive: never taking up that new hobby, because you’re just going to suck at it anyway, and what’s the point if you’re not going to excel? You’re a perfectionist, and you don’t settle for anything less than excellence.
- Adaptive: researching the new hobby, learning the basics, and recognizing that even if the results are not immediately perfect, the learning process can be… Yes, even with mistakes along the way, for they too are part of learning! You’re a perfectionist, and you’re going to be the best possible student of your new hobby.
Did you catch the key there?
When it comes to approaching things we do in life—either because we want to or because we must—there are two kinds of mindset: goal-oriented, and task-oriented.
Broadly speaking, each has their merits, and as a general topic, it’s beyond the scope of today’s main feature. Here we’re looking at it in the context of perfectionism, and in that frame, there’s a clear qualitative difference:
- The goal-oriented perfectionist will be frustrated to the point of torment, at not immediately attaining the goal. Everything short of that will be a means to an end, at best. Not fun.
- The task-oriented perfectionist will take joy in going about the task in the best way possible, and optimizing their process as they go. The journey itself will be rewarding and a tangible product of their consistent perfectionism.
The good news is: you get to choose! You’re not stuck in a box.
If you’re thinking “I’m a perfectionist and I’m generally a goal-oriented person”, that’s fine. You’re just going to need to reframe your goals.
- Instead of: my goal is to be fluent in Arabic
- …so you never speak it, because to err is human, all too human, and you’re a perfectionist, so you don’t want that!
- Let’s try: my goal is to study Arabic for at least 15 minutes per day, every day, without fail, covering at least some new material each time, no matter how small the increase
- …and then you go and throw yourself into conversation way out of your depth, make mistakes, and get corrections, because that’s how you learn, and you’re a perfectionist, so you want that!
This goes for any field of expertise, of course.
- If you want to play the violin solo in Carnegie Hall, you have to pick up your violin and practice each day.
- If you want to be a world-renowned pastry chef, you have to make a consistent habit of baking.
- If you want to write a bestselling book, you have to show up at your keyboard.
Be perfect all you want, but be the perfect student.
And as your skills grow, maybe you’ll upgrade that to also being the perfect practitioner, and perhaps later still, the perfect teacher.
But just remember:
Perfection comes not from the end goal (that would be backwards thinking!) but from the process (which includes mistakes; they’re an important part of learning; embrace them and grow!), so perfect that first.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How Does One Test Acupuncture Against Placebo Anyway?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Pinpointing The Usefulness Of Acupuncture

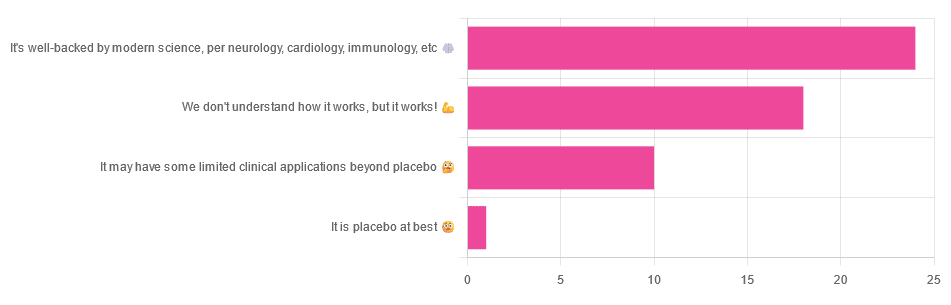
We asked you for your opinions on acupuncture, and got the above-depicted, below-described, set of answers:
- A little under half of all respondents voted for “It’s well-backed by modern science, per neurology, cardiology, immunology, etc”
- Slightly fewer respondents voted for “We don’t understand how it works, but it works!”
- A little under a fifth of respondents voted for “It may have some limited clinical applications beyond placebo”
- One (1) respondent voted for for “It’s placebo at best”
When we did a main feature about homeopathy, a couple of subscribers wrote to say that they were confused as to what homeopathy was, so this time, we’ll start with a quick definition first.
First, what is acupuncture? For the convenience of a quick definition so that we can move on to the science, let’s borrow from Wikipedia:
❝Acupuncture is a form of alternative medicine and a component of traditional Chinese medicine in which thin needles are inserted into the body.
Acupuncture is a pseudoscience; the theories and practices of TCM are not based on scientific knowledge, and it has been characterized as quackery.❞
Now, that’s not a promising start, but we will not be deterred! We will instead examine the science itself, rather than relying on tertiary sources like Wikipedia.
It’s worth noting before we move on, however, that there is vigorous debate behind the scenes of that article. The gist of the argument is:
- On one side: “Acupuncture is not pseudoscience/quackery! This has long been disproved and there are peer-reviewed research papers on the subject.”
- On the other: “Yes, but only in disreputable quack journals created specifically for that purpose”
The latter counterclaim is a) potentially a “no true Scotsman” rhetorical ploy b) potentially true regardless
Some counterclaims exhibit specific sinophobia, per “if the source is Chinese, don’t believe it”. That’s not helpful either.
Well, the waters sure are muddy. Where to begin? Let’s start with a relatively easy one:
It may have some clinical applications beyond placebo: True or False?
True! Admittedly, “may” is doing some of the heavy lifting here, but we’ll take what we can get to get us going.
One of the least controversial uses of acupuncture is to alleviate chronic pain. Dr. Vickers et al, in a study published under the auspices of JAMA (a very respectable journal, and based in the US, not China), found:
❝Acupuncture is effective for the treatment of chronic pain and is therefore a reasonable referral option. Significant differences between true and sham acupuncture indicate that acupuncture is more than a placebo.
However, these differences are relatively modest, suggesting that factors in addition to the specific effects of needling are important contributors to the therapeutic effects of acupuncture❞
Source: Acupuncture for Chronic Pain: Individual Patient Data Meta-analysis
If you’re feeling sharp today, you may be wondering how the differences are described as “significant” and “relatively modest” in the same text. That’s because these words have different meanings in academic literature:
- Significant = p<0.05, where p is the probability of the achieved results occurring randomly
- Modest = the differences between the test group and the control group were small
In other words, “significant modest differences” means “the sample sizes were large, and the test group reliably got slightly better results than placebo”
We don’t understand how it works, but it works: True or False
Broadly False. When it works, we generally have an idea how.
Placebo is, of course, the main explanation. And even in examples such as the above, how is placebo acupuncture given?
By inserting acupuncture needles off-target rather than in accord with established meridians and points (the lines and dots that, per Traditional Chinese Medicine, indicate the flow of qi, our body’s vital energy, and welling-points of such).
So, if a patient feels that needles are being inserted randomly, they may no longer have the same confidence that they aren’t in the control group receiving placebo, which could explain the “modest” difference, without there being anything “to” acupuncture beyond placebo. After all, placebo works less well if you believe you are only receiving placebo!
Indeed, a (Korean, for the record) group of researchers wrote about this—and how this confounding factor cuts both ways:
❝Given the current research evidence that sham acupuncture can exert not only the originally expected non-specific effects but also sham acupuncture-specific effects, it would be misleading to simply regard sham acupuncture as the same as placebo.
Therefore, researchers should be cautious when using the term sham acupuncture in clinical investigations.❞
Source: Sham Acupuncture Is Not Just a Placebo
It’s well-backed by modern science, per neurology, cardiology, immunology, etc: True or False?
False, for the most part.
While yes, the meridians and points of acupuncture charts broadly correspond to nerves and vasculature, there is no evidence that inserting needles into those points does anything for one’s qi, itself a concept that has not made it into Western science—as a unified concept, anyway…
Note that our bodies are indeed full of energy. Electrical energy in our nerves, chemical energy in every living cell, kinetic energy in all our moving parts. Even, to stretch the point a bit, gravitational potential energy based on our mass.
All of these things could broadly be described as qi, if we so wish. Indeed, the ki in the Japanese martial art of aikido is the latter kinds; kinetic energy and gravitational potential energy based on our mass. Same goes, therefore for the ki in kiatsu, a kind of Japanese massage, while the ki in reiki, a Japanese spiritual healing practice, is rather more mystical.
The qi in Chinese qigong is mostly about oxygen, thus indirectly chemical energy, and the electrical energy of the nerves that are receiving oxygenated blood at higher or lower levels.
On the other hand, the efficacy of the use of acupuncture for various kinds of pain is well-enough evidenced. Indeed, even the UK’s famously thrifty NHS (that certainly would not spend money on something it did not find to work) offers it as a complementary therapy for some kinds of pain:
❝Western medical acupuncture (dry needling) is the use of acupuncture following a medical diagnosis. It involves stimulating sensory nerves under the skin and in the muscles.
This results in the body producing natural substances, such as pain-relieving endorphins. It’s likely that these naturally released substances are responsible for the beneficial effects experienced with acupuncture.❞
Source: NHS | Acupuncture
Meanwhile, the NIH’s National Cancer Institute recommends it… But not as a cancer treatment.
Rather, they recommend it as a complementary therapy for pain management, and also against nausea, for which there is also evidence that it can help.
Frustratingly, while they mention that there is lots of evidence for this, they don’t actually link the studies they’re citing, or give enough information to find them. Instead, they say things like “seven randomized clinical trials found that…” and provide links that look reassuring until one finds, upon clicking on them, that it’s just a link to the definition of “randomized clinical trial”:
Source: NIH | Nactional Cancer Institute | Acupuncture (PDQ®)–Patient Version
However, doing our own searches finds many studies (mostly in specialized, potentially biased, journals such as the Journal of Acupuncture and Meridian Studies) finding significant modest outperformance of [what passes for] placebo.
Sometimes, the existence of papers with promising titles, and statements of how acupuncture might work for things other than relief of pain and nausea, hides the fact that the papers themselves do not, in fact, contain any evidence to support the hypothesis. Here’s an example:
❝The underlying mechanisms behind the benefits of acupuncture may be linked with the regulation of the hypothalamic-pituitary-gonadal (adrenal) axis and activation of the Wnt/β-catenin and OPG/RANKL/RANK signaling pathways.
In summary, strong evidence may still come from prospective and well-designed clinical trials to shed light on the potential role of acupuncture in preserving bone loss❞
Source: Acupuncture for Osteoporosis: a Review of Its Clinical and Preclinical Studies
So, here they offered a very sciencey hypothesis, and to support that hypothesis, “strong evidence may still come”.
“We must keep faith” is not usually considered evidence worthy of inclusion in a paper!
PS: the above link is just to the abstract, because the “Full Text” link offered in that abstract leads to a completely unrelated article about HIV/AIDS-related cryptococcosis, in a completely different journal, nothing to do with acupuncture or osteoporosis).
Again, this is not the kind of professionalism we expect from peer-reviewed academic journals.
Bottom line:
Acupuncture reliably performs slightly better than sham acupuncture for the management of pain, and may also help against nausea.
Beyond placebo and the stimulation of endorphin release, there is no consistently reliable evidence that is has any other discernible medical effect by any mechanism known to Western science—though there are plenty of hypotheses.
That said, absence of evidence is not evidence of absence, and the logistical difficulty of testing acupuncture against placebo makes for slow research. Maybe one day we’ll know more.
For now:
- If you find it helps you: great! Enjoy
- If you think it might help you: try it! By a licensed professional with a good reputation, please.
- If you are not inclined to having needles put in you unnecessarily: skip it! Extant science suggests that at worst, you’ll be missing out on slight relief of pain/nausea.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: