Edamame vs Pistachios – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing edamame to pistachios, we picked the pistachios.
Why?
Of these two small green proteinous snacks, they’re both very nutritionally dense but there is a winner:
In terms of macros, pistachios have about 2x the protein, 8x the fat (and/but: healthy fats!), and a little over 2x the carbs, as well as 2x the fiber, giving pistachios an easy first-round win.
In the category of vitamins, edamame has more of vitamins A, B9, C, and K, while pistachios have more of vitamins B1, B2, B3, B5, B6, and E, winning again.
Looking at minerals, edamame is not higher in any minerals, while pistachios have more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, winning their third round by a country mile.
In other considerations, edamame does have more polyphenols, though not by much, so there’s a small point in edamame’s favor.
Adding up the section makes for a clear overall win for pistachios, but do enjoy either or both (unless you have a soy and/or nut allergy, in which case, avoid your allergen(s) of course), as diversity is good, and edamame really is great too, it just doesn’t look it when sitting next to pistachios!
Want to learn more?
You might like:
Why You Should Diversify Your Nuts
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How To Walk Away From Alzheimer’s

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We have written before avoiding Alzheimer’s in many different ways, for example:
Alzheimer’s Causative Factors To Avoid
…and regular readers will also be aware of our dictum “what’s good for the heart, is good for the brain”, which is because the heart feeds the brain, with oxygen and nutrients, and also ultimately clears away detritus like beta-amyloid (associated with Alzheimer’s).
For much more detail on this, see: What’s Your Vascular Dementia Risk? ← includes actual numbers and a risk calculator tool and things like that
So, it’s no surprise of course that exercise is protective against dementia, and as per the above, typically the most important thing here is heart health, so getting regular cardiovascular exercise, such walking, running, or dancing is great. Cycling too. Things like that.
Beyond cardio
First, some background. A previous (2023) study concluded:
❝Among older adults, more time spent in sedentary behaviors was significantly associated with higher incidence of all-cause dementia. Future research is needed to determine whether the association between sedentary behavior and risk of dementia is causal.❞
Source: Sedentary Behavior and Incident Dementia Among Older Adults
We’re not going to go deeply into that paper, because our interest today is about the answer to that call of “future research is needed”, because a team of scientists have now delivered on that.
In terms of how recent this new research is, it was published today (at time of writing), in the Journal of the Alzheimer’s Association.
In it, Dr. Marissa Gogniat et al. examined the relationship between sedentary behavior and cognitive decline and neurodegeneration, in 404 adults aged 50+.
A note on “cognitive decline” and “neurodegeneration”: those two terms are often used interchangeably, because they are usually strongly associated with each other so if one goes up or down then so does the other, but technically:
- cognitive decline = a decline of cognitive abilities, as measured by cognitive performance tests
- neurodegeneration = physical degeneration of neural tissue, typically specifically in the brain, as measured by various physical markers of neurodegeneration (tests range from brain scans to blood markers to biopsies and more, but the point is that it’s all physical stuff)
While based on the one-line summary we gave (“examined the relationship between sedentary behavior and cognitive decline / neurodegeneration”), this can sound a bit like a “examined whether water is wet” study, but in fact it becomes interesting when physical exercise is controlled for, since they found:
❝Reducing your risk for Alzheimer’s disease is not just about working out once a day. Minimizing the time spent sitting, even if you do exercise daily, reduces the likelihood of developing Alzheimer’s disease.❞
~ Dr. Marissa Gogniat
Too vague? Here’s the less vague version:
❝In cross-sectional models, greater sedentary time related to a smaller AD-neuroimaging signature (β = -0.0001, p = 0.01) and worse episodic memory (β = -0.001, p = 0.003). Associations differed by APOE-ε4 status. In longitudinal models, greater sedentary time related to faster hippocampal volume reductions (β = -0.1, p = 0.008) and declines in naming (β = -0.001, p = 0.03) and processing speed (β = -0.003, p = 0.02; β = 0.01, p = 0.01).❞
In other words:
- Those are very significant findings, statistically speaking; the causal association cannot be reasonably denied without some strong new evidence for why
- Greater sedentary behavior is related to neurodegeneration and worse cognition.
- Sedentary behavior is an independent* risk factor for Alzheimer’s disease.
- Associations differed by APOE-ε4 carrier status in cross-sectional models.
*as in, the sedentary risk factor stands (so to speak) regardless of whether you exercise a lot
With regard to “Associations differed by APOE-ε4 carrier status in cross-sectional models.”, that’s a little complicated, as …
❝Interestingly, we only found a sedentary time x APOE-ε4 status interaction on occipital volume longitudinally (which did not survive correction for multiple comparisons) and no interactions on cognition. The significant effect on occipital lobe volume was driven by APOE-ε4 non-carriers, which does not align with our cross-sectional findings. APOE-ε4 carriers are thought to have accelerated gray matter volume loss, starting possibly in middle age. Therefore, while increased sedentary time may impact gray matter volume among APOE-ε4 carriers, this effect may be masked by the cumulative effect of APOE-ε4 on brain volume over the lifespan that is captured at baseline.❞
In other words: in all likelihood, having the APOE-ε4 mutation probably means it’s extra important for you to not be sedentary in your lifestyle, and (good news) being non-sedentary is probably disproportionately impactful for you in a positive way, but (bad news) the APOE-ε4 mutation causes such an increased risk already, that it’s difficult to 100% ascertain that statistically, without larger samples starting earlier in life.
You can read the paper in full here:
“What if have to spend a lot of time sitting down?”
A valid question, relevant for many.
For this, check out:
Stand Up For Your Health (Or Don’t) ← our main feature on this also includes more things you can do if you must sit, to make sitting less bad!
Take care!
Share This Post
-

Do We Simply Not Care About Old People?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The covid-19 pandemic would be a wake-up call for America, advocates for the elderly predicted: incontrovertible proof that the nation wasn’t doing enough to care for vulnerable older adults.
The death toll was shocking, as were reports of chaos in nursing homes and seniors suffering from isolation, depression, untreated illness, and neglect. Around 900,000 older adults have died of covid-19 to date, accounting for 3 of every 4 Americans who have perished in the pandemic.
But decisive actions that advocates had hoped for haven’t materialized. Today, most people — and government officials — appear to accept covid as a part of ordinary life. Many seniors at high risk aren’t getting antiviral therapies for covid, and most older adults in nursing homes aren’t getting updated vaccines. Efforts to strengthen care quality in nursing homes and assisted living centers have stalled amid debate over costs and the availability of staff. And only a small percentage of people are masking or taking other precautions in public despite a new wave of covid, flu, and respiratory syncytial virus infections hospitalizing and killing seniors.
In the last week of 2023 and the first two weeks of 2024 alone, 4,810 people 65 and older lost their lives to covid — a group that would fill more than 10 large airliners — according to data provided by the CDC. But the alarm that would attend plane crashes is notably absent. (During the same period, the flu killed an additional 1,201 seniors, and RSV killed 126.)
“It boggles my mind that there isn’t more outrage,” said Alice Bonner, 66, senior adviser for aging at the Institute for Healthcare Improvement. “I’m at the point where I want to say, ‘What the heck? Why aren’t people responding and doing more for older adults?’”
It’s a good question. Do we simply not care?
I put this big-picture question, which rarely gets asked amid debates over budgets and policies, to health care professionals, researchers, and policymakers who are older themselves and have spent many years working in the aging field. Here are some of their responses.
The pandemic made things worse. Prejudice against older adults is nothing new, but “it feels more intense, more hostile” now than previously, said Karl Pillemer, 69, a professor of psychology and gerontology at Cornell University.
“I think the pandemic helped reinforce images of older people as sick, frail, and isolated — as people who aren’t like the rest of us,” he said. “And human nature being what it is, we tend to like people who are similar to us and be less well disposed to ‘the others.’”
“A lot of us felt isolated and threatened during the pandemic. It made us sit there and think, ‘What I really care about is protecting myself, my wife, my brother, my kids, and screw everybody else,’” said W. Andrew Achenbaum, 76, the author of nine books on aging and a professor emeritus at Texas Medical Center in Houston.
In an environment of “us against them,” where everybody wants to blame somebody, Achenbaum continued, “who’s expendable? Older people who aren’t seen as productive, who consume resources believed to be in short supply. It’s really hard to give old people their due when you’re terrified about your own existence.”
Although covid continues to circulate, disproportionately affecting older adults, “people now think the crisis is over, and we have a deep desire to return to normal,” said Edwin Walker, 67, who leads the Administration on Aging at the Department of Health and Human Services. He spoke as an individual, not a government representative.
The upshot is “we didn’t learn the lessons we should have,” and the ageism that surfaced during the pandemic hasn’t abated, he observed.
Ageism is pervasive. “Everyone loves their own parents. But as a society, we don’t value older adults or the people who care for them,” said Robert Kramer, 74, co-founder and strategic adviser at the National Investment Center for Seniors Housing & Care.
Kramer thinks boomers are reaping what they have sown. “We have chased youth and glorified youth. When you spend billions of dollars trying to stay young, look young, act young, you build in an automatic fear and prejudice of the opposite.”
Combine the fear of diminishment, decline, and death that can accompany growing older with the trauma and fear that arose during the pandemic, and “I think covid has pushed us back in whatever progress we were making in addressing the needs of our rapidly aging society. It has further stigmatized aging,” said John Rowe, 79, professor of health policy and aging at Columbia University’s Mailman School of Public Health.
“The message to older adults is: ‘Your time has passed, give up your seat at the table, stop consuming resources, fall in line,’” said Anne Montgomery, 65, a health policy expert at the National Committee to Preserve Social Security and Medicare. She believes, however, that baby boomers can “rewrite and flip that script if we want to and if we work to change systems that embody the values of a deeply ageist society.”
Integration, not separation, is needed. The best way to overcome stigma is “to get to know the people you are stigmatizing,” said G. Allen Power, 70, a geriatrician and the chair in aging and dementia innovation at the Schlegel-University of Waterloo Research Institute for Aging in Canada. “But we separate ourselves from older people so we don’t have to think about our own aging and our own mortality.”
The solution: “We have to find ways to better integrate older adults in the community as opposed to moving them to campuses where they are apart from the rest of us,” Power said. “We need to stop seeing older people only through the lens of what services they might need and think instead of all they have to offer society.”
That point is a core precept of the National Academy of Medicine’s 2022 report Global Roadmap for Healthy Longevity. Older people are a “natural resource” who “make substantial contributions to their families and communities,” the report’s authors write in introducing their findings.
Those contributions include financial support to families, caregiving assistance, volunteering, and ongoing participation in the workforce, among other things.
“When older people thrive, all people thrive,” the report concludes.
Future generations will get their turn. That’s a message Kramer conveys in classes he teaches at the University of Southern California, Cornell, and other institutions. “You have far more at stake in changing the way we approach aging than I do,” he tells his students. “You are far more likely, statistically, to live past 100 than I am. If you don’t change society’s attitudes about aging, you will be condemned to lead the last third of your life in social, economic, and cultural irrelevance.”
As for himself and the baby boom generation, Kramer thinks it’s “too late” to effect the meaningful changes he hopes the future will bring.
“I suspect things for people in my generation could get a lot worse in the years ahead,” Pillemer said. “People are greatly underestimating what the cost of caring for the older population is going to be over the next 10 to 20 years, and I think that’s going to cause increased conflict.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-
Going to the dentist is expensive. Here are 3 things you can do to protect your oral health – and 3 things to avoid
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Around one in three Australians delayed their visit to a dentist in the last financial year – or didn’t go at all – due to cost.
Given it doesn’t look like dental treatment is being added to Medicare any time soon, what can you do?
Most oral and dental diseases are preventable, if you take care of your teeth and mouth. In-between visits to the dentist, here’s what you can do to avoid preventable issues – and blow-out costs.

Jiri Hera/Shutterstock What causes diseases in your mouth?
More than 1,000 species of microbes live in the mouth. Most dental and oral diseases are due to an imbalance or overgrowth in these microbes within the plaque (or “biofilm”).
Plaque gathers on the hard surfaces inside the mouth (your teeth), as well as soft surfaces (such as your tongue). Removing plaque manually with brushing and flossing is the most effective way to maintain oral health.
Plaque starts to form immediately after brushing, which is why you should remove it regularly.
Things to do
1. Brush twice a day
Use a toothbrush with soft bristles (either electric or manual). Soft bristles remove plaque without damaging the teeth or gums. A fluoridated toothpaste will help strengthen the teeth.
Brush for at least two minutes, using a sweeping and scrubbing motion, away from the gums. It’s a good idea to start at the back teeth and work your way through to the front teeth. Don’t forget to scrub the biting surface of the teeth.
2. Floss
Don’t skip this step – it’s crucial to clean in-between the teeth where a toothbrush can’t reach. Once a day should be enough.
Whether you use floss, a pick, a bottle brush or other devices may depend on the space between your teeth.
3. Clean your tongue
To completely remove the microbes, it’s also important to clean your tongue regularly (twice daily). You can use a toothbrush while you’re already brushing, or a special tongue scraper – just don’t brush or scrape too hard.
Brushing twice a day is important to remove bacteria in the mouth and on the teeth. PeopleImages.com – Yuri A/Shutterstock Things to avoid
1. Sugary drinks and refined food
What we eat and drink can affect the mouth’s pH.
When bacteria in the mouth break down sugars, they produce acids. The acidity can dissolve minerals in the teeth and lead to decay.
Refined foods – such as white bread, cakes and pastries – can easily be broken down by the mouth’s bacteria. So, having a lot of them, as well as sugary drinks, can damage the teeth and cause cavities.
Water is the best choice to drink with your meals. Sparkling and soda water are acidic and can lead to mineral loss from the teeth, even when they are unflavoured. There is evidence flavoured sparkling water can be as harmful as orange juice.
2. Tobacco and vaping
Smoking or using smokeless tobacco (such as chewed tobacco or snuff pouches) is linked to oral cancer.
Nicotine is also known to increase the severity of gum diseases – even when inflammation isn’t visible.
This is true for both smoking and smokeless tobacco (such as chewed tobacco or snuff pouches).
Vaping also increases your risk of developing cavities and gum disease.
3. Too much alcohol, tea and coffee
Drinking a lot of coffee, tea or red wine can stain your teeth. So if you’re concerned about your teeth appearing yellow or brown, it’s best to limit your intake.
Drinking alcohol is also linked to an increased risk of developing oral cancers, which most commonly affect the tongue, floor of the mouth, cheek and palate.
Drinks that are fizzy and sugary can damage the teeth. Svetlana Foote/Shutterstock Your mouth’s health is linked to your overall health
Leaving oral diseases untreated (such as gum disease) has been linked to developing other conditions, such as liver disease, and pre-existing conditions getting worse.
This is particularly evident if you have diabetes. Evidence shows it’s easier to manage blood sugar levels when gum diseases are properly treated.
You can keep an eye on symptoms such as bleeding gums, which may be an early sign of gum disease. If symptoms worry you, talk to your GP or diabetes educator. They may be able to refer you to a dentist if needed.
Dileep Sharma, Professor and Head of Discipline – Oral Health, University of Newcastle
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post





Related Posts
-
You can train your nose – and 4 other surprising facts about your sense of smell
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Would you give up your sense of smell to keep your hair? What about your phone?
A 2022 US study compared smell to other senses (sight and hearing) and personally prized commodities (including money, a pet or hair) to see what people valued more.
The researchers found smell was viewed as much less important than sight and hearing, and valued less than many commodities. For example, half the women surveyed said they’d choose to keep their hair over sense of smell.
Smell often goes under the radar as one of the least valued senses. But it is one of the first sensory systems vertebrates developed and is linked to your mental health, memory and more.
Here are five fascinating facts about your olfactory system.
DimaBerlin/Shutterstock 1. Smell is linked to memory and emotion
Why can the waft of fresh baking trigger joyful childhood memories? And why might a certain perfume jolt you back to a painful breakup?
Smell is directly linked to both your memory and emotions. This connection was first established by American psychologist Donald Laird in 1935 (although French novelist Marcel Proust had already made it famous in his reverie about the scent of madeleines baking.)
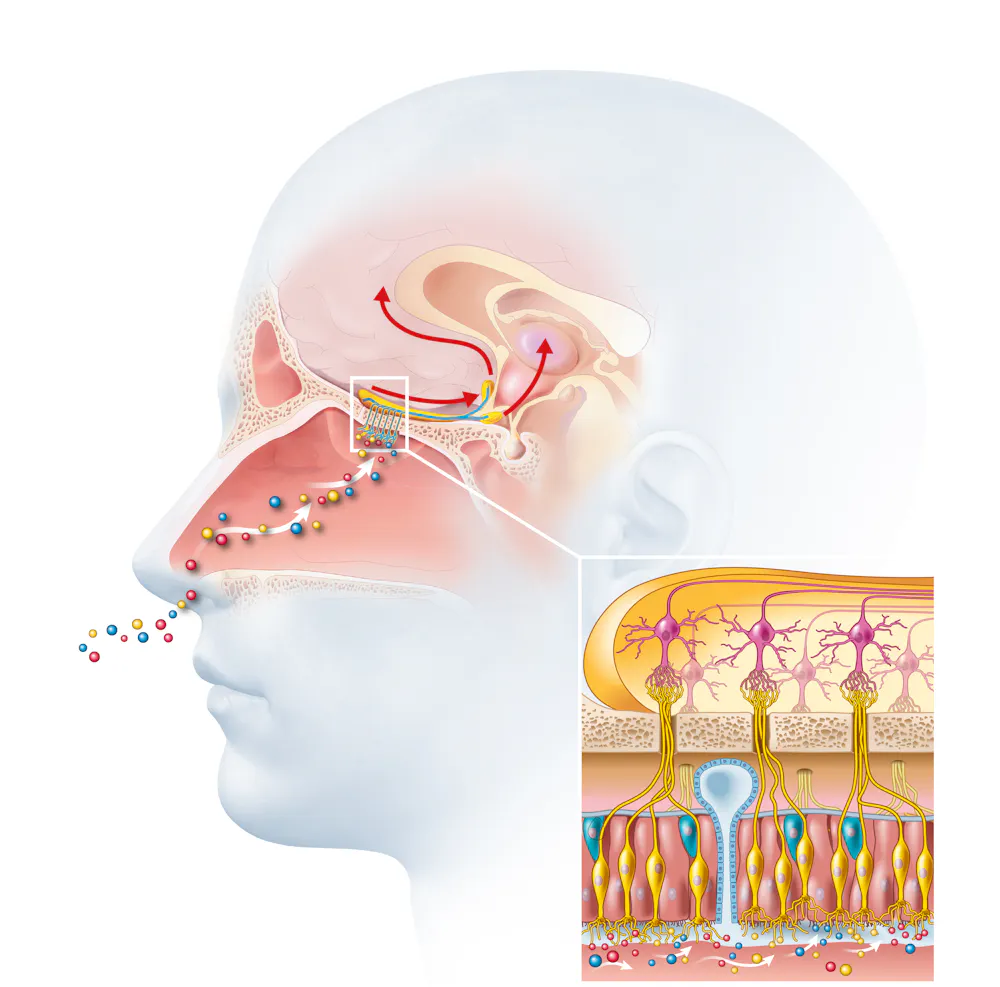
Odours are first captured by special olfactory nerve cells inside your nose. These cells extend upwards from the roof of your nose towards the smell-processing centre of your brain, called the olfactory bulb.
Smells are first detected by nerve cells in the nose. Axel_Kock/Shutterstock From the olfactory bulb they form direct connection with the brain’s limbic system. This includes the amygdala, where emotions are generated, and the hippocampus, where memories are created.
Other senses – such as sight and hearing – aren’t directly connected to the lymbic system.
One 2004 study used functional magnetic resonance imaging to demonstrate odours trigger a much stronger emotional and memory response in the brain than a visual cue.
2. Your sense of smell constantly regenerates
You can lose your ability to smell due to injury or infection – for example during and after a COVID infection. This is known as olfactory dysfunction. In most cases it’s temporary, returning to normal within a few weeks.
This is because every few months your olfactory nerve cells die and are replaced by new cells.
We’re not entirely sure how this occurs, but it likely involves your nose’s stem cells, the olfactory bulb and other cells in the olfactory nerves.
Other areas of your nervous system – including your brain and spinal cord – cannot regenerate and repair after an injury.
Constant regeneration may be a protective mechanism, as the olfactory nerves are vulnerable to damage caused by the external environment, including toxins (such as cigarette smoke), chemicals and pathogens (such as the flu virus).
But following a COVID infection some people might continue to experience a loss of smell. Studies suggest the virus and a long-term immune response damages the cells that allow the olfactory system to regenerate.
3. Smell is linked to mental health
Around 5% of the global population suffer from anosmia – total loss of smell. An estimated 15-20% suffer partial loss, known as hyposmia.
Given smell loss is often a primary and long-term symptom of COVID, these numbers are likely to be higher since the pandemic.
Yet in Australia, the prevalence of olfactory dysfunction remains surprisingly understudied.
Losing your sense of smell is shown to impact your personal and social relationships. For example, it can mean you miss out on shared eating experiences, or cause changes in sexual desire and behaviour.
In older people, declining ability to smell is associated with a higher risk of depression and even death, although we still don’t know why.
Losing your sense of smell can have a major impact on mental health. Halfpoint/Shutterstock 4. Loss of smell can help identify neurodegenerative diseases
Partial or full loss of smell is often an early indicator for a range of neurodegenerative diseases, including Alzheimer’s and Parkinson’s diseases.
Patients frequently report losing their sense of smell years before any symptoms show in body or brain function. However many people are not aware they are losing their sense of smell.
There are ways you can determine if you have smell loss and to what extent. You may be able to visit a formal smell testing centre or do a self-test at home, which assesses your ability to identify household items like coffee, wine or soap.
5. You can train your nose back into smelling
“Smell training” is emerging as a promising experimental treatment option for olfactory dysfunction. For people experiencing smell loss after COVID, it’s been show to improve the ability to detect and differentiate odours.
Smell training (or “olfactory training”) was first tested in 2009 in a German psychology study. It involves sniffing robust odours — such as floral, citrus, aromatic or fruity scents — at least twice a day for 10—20 seconds at a time, usually over a 3—6 month period.
Participants are asked to focus on the memory of the smell while sniffing and recall information about the odour and its intensity. This is believed to help reorganise the nerve connections in the brain, although the exact mechanism behind it is unclear.
Some studies recommend using a single set of scents, while others recommend switching to a new set of odours after a certain amount of time. However both methods show significant improvement in smelling.
This training has also been shown to alleviate depressive symptoms and improve cognitive decline both in older adults and those suffering from dementia.
Just like physiotherapy after a physical injury, olfactory training is thought to act like rehabilitation for your sense of smell. It retrains the nerves in your nose and the connections it forms within the brain, allowing you to correctly detect, process and interpret odours.
Lynn Nazareth, Research Scientist in Olfactory Biology, CSIRO
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Surviving A Heart Attack? Stroke? There’s An App For That
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
❝Stopped.❞
~ The last words of Dr. Joseph Henry Green, President of the Royal College of Surgeons, who had been taking his own pulse
Sometimes, self-diagnosis isn’t so clear as that, though, especially when it comes to life-threatening issues with the heart and brain (i.e. things we can’t readily look at, and diagnose with the same ease we might diagnose a broken arm or such). Indeed, many people have a heart attack or stroke and, upon finding that they are not dead, conclude “I guess I’m fine after all” and continue about their day
Unfortunately, it’s often the case that in fact they still needed medical attention within the hour (literally: the hour after a heart attack or stroke is called “the golden hour” by doctors in the field, as medical treatments are most effective then, and less likely to help so much afterwards).
As a result, a lot of people die because they didn’t seek medical attention because they dismissed their own experience once the immediate symptoms abated.
About The “Emergency Call for Heart Attack and Stroke” (ECHAS) App
This is a smartphone app that can be used at home to identify the signs of heart attacks and strokes, including:
- A virtual exam using questions similar to those asked in ERs.
- A finger-tapping test to detect one-sided body weakness.
- A risk score to advise whether to call 911, a hotline, or a doctor.
In a moderate-size (n=202) study, it successfully detected strokes in under 2 minutes and heart attacks in 1 minute, and when we say “successfully”, it was 100% accurate in identifying patients who were later admitted to the hospital. Obviously, we cannot say about the patients who didn’t go to hospital, because there was (consequently) no further data for them, but we can conclude:
- there were no false positives (that’s the “100% accurate in identifying patients who were later admitted to the hospital” part)
- while we can’t say for sure there were no false negatives, it is promising that there were no reports of “app said patient was fine, patient then deteriorated/died”, which would have been picked up. So, it looks promisingly like there were no false negatives either.
In terms of ease of use, it was rated by the study participants as very easy to use, making it suitable for people without medical training, and for that matter, people without medical training in the middle of a medical crisis who thus might not be at their best when using it.
You can read the study paper in full, here: Assessment of the Sensitivity of a Smartphone App to Assist Patients in the Identification of Stroke and Myocardial Infarction: Cross-Sectional Study
Sounds great; where can I get it?
At time of writing, it’s not publicly available just yet, but the researchers want to trial it on a much larger scale, so we’ll keep an eye out for invitations to that trial (probably in a huge, crowdsourced data way, like ZOE and 1 Million Nights and such) and advise you to do so, too.
In all likelihood, it’ll appear soon for iPhone and Android in their respective app stores.
In the meantime, you might want to check out:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What’s the link between talcum powder and cancer?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
More than 1,300 Victorians have joined a class action against Johnson & Johnson alleging its talcum powder products left them with ovarian cancer, mesothelioma (cancer affecting the lungs) and other cancers affecting the reproductive organs.
This follows lawsuits in the United Kingdom and the United States, including a prominent case in California. In December 2025, Johnson & Johnson was forced to pay two women US$40 million after a jury found its baby powder was dangerous and that it had failed to warn consumers.
Talc is a naturally occurring mineral mined in many parts of the world. People can come into contact with it during mining and processing, industrial applications, and more commonly, through its use in cosmetics and body powders.
People use talc on their genitals to absorb moisture, reduce friction, disguise odours, or to reduce skin rashes and chafing. Talc increases the opaqueness of face powders and cosmetics, leaving skin feeling smooth and soft.
So how is it linked to cancer? And what does the scientific evidence say?
Contamination with asbestos
Since the 1970s, questions have emerged about whether talc could be contaminated with asbestos. Asbestos is a cancer-causing agent that can affect the lungs when inhaled.
Talc and asbestos are minerals often found close to each other in the Earth, so there is potential for talc to be contaminated with asbestos during the mining process.
Since the 1970s, manufacturers have attempted to produce pure talcum powder free from asbestos. However, it’s unclear how routinely samples are tested and the extent of contamination over the past 50 years.
In 2023, Johnson & Johnson stopped selling talc in its products worldwide, including in Australia, switching instead to a cornflour base. Other manufacturers still sell talcum powder and it’s still used in cosmetics, as well as industrially.
What does the science say about the cancer link?
Two cancers have a possible link with talc use:
- lung cancer, due to the potential to inhale talc particles, which can occur with some types of jobs
- ovarian cancer, due to regular use of talcum powder in the genital area.
Some human studies have found products containing talc are linked with higher rates of ovarian cancer. Other studies have found no link.
Studies that examined the use of talc on the genital area found no evidence to suggest a link between talc and uterine or cervical cancer.
But there are several challenges to overcome when studying the link between talcum powder and cancer. It can be difficult to recall details about talc use (brand, amount, and so on) many years later. Some people who developed cancer will have died before being identified and studied, so won’t be included.
However, when researchers investigated how often participants used talc powder and compared those who used it frequently with those who didn’t, they found an increased risk of ovarian cancer among frequent users.
So what does it all mean?
When there are differing results from multiple studies, those results can be summarised together to answer the research question. So what does all the currently available evidence say about the relationship between talc usage and ovarian cancer?
This summary study concludes there appears to be a weak risk of some types of ovarian cancer, meaning it’s linked to a small increase in risk, but the reasons why remain unclear.
The evidence suggests talc does not increase the risk of other gynaecological cancers, such as uterine and cervical.
Talc contaminated with asbestos is clearly linked to an increased risk of lung cancer. However, cosmetic use of talc doesn’t seem to increase the risk of lung cancer because users don’t breathe it in.
In 2024 the World Health Organization (WHO) updated its advice to say that talc is “probably carcinogenic” which means it probably causes cancer in humans. This is the second-highest risk level for cancer, which includes the herbicide glyphosate (Roundup) and red meat.
If you use talcum powder and are concerned about an increased risk of cancer, it’s recommended you stop using it or limit how much you use. As with all decisions in life, consider the balance between potential harms and benefits, especially if you’ve used talc for a long time and want to minimise your risk of getting cancer.
Tam Ha, Associate Professor of Cancer Epidemiology, University of Wollongong
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: