Edam vs Gouda – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing edam to gouda, we picked the edam.
Why?
There’s not a lot between them, but there are some differences:
In terms of macros, their numbers are all close enough that one may beat the other by decimal place rounding, so we’ll call this a tie. Same goes for their fat type breakdowns; per 100g they both have 18g saturated, 8g monounsaturated, and 1g polyunsaturated.
In the category of vitamins, edam has slightly more of vitamins A, B1, B2, and B3, while gouda has slightly more of vitamins B5 and B9. A modest 4:2 win for edam.
When it comes to minerals, edam has more calcium, iron, and potassium, while gouda is not higher in any minerals. A more convincing win for edam.
In short, enjoy either or both in moderation, but if you’re going to choose one over the other, edam is the way to go.
Want to learn more?
You might like to read:
Can Saturated Fats Be Healthy?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

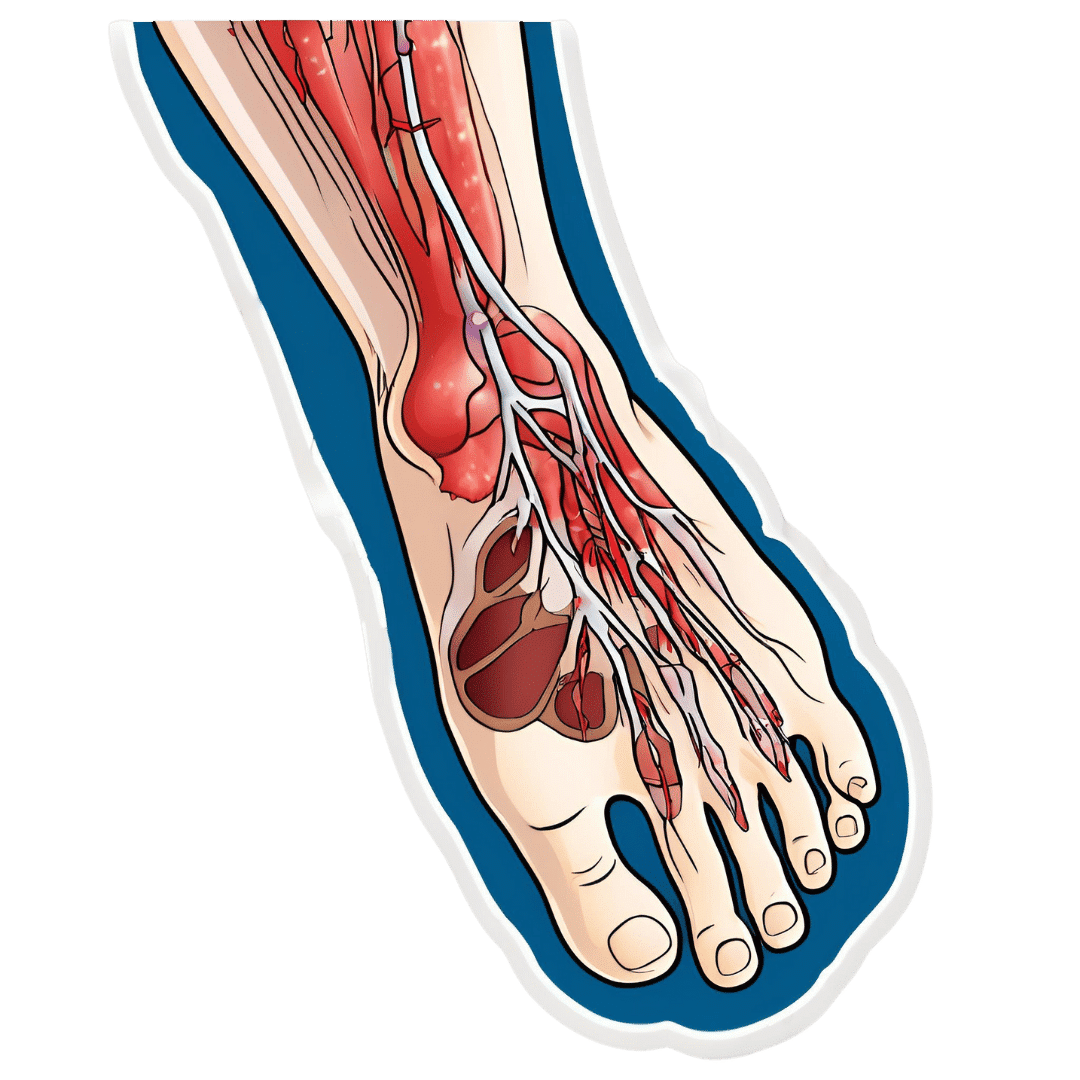
How To Stay A Step Ahead Of Peripheral Artery Disease

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Far less well-known than Coronary Artery Disease, it can still result in loss of life and limb (not in that order). Fortunately, there are ways to be on your guard:
What it is
Peripheral Artery Disease (PAD) is the same thing as Coronary Artery Disease (CAD), just, in the periphery—which by definition means “outside of the heart and brain”, but in practice, it starts with the extremities. And of the extremities, it tends to start with the feet and legs, for the simple reason that if someone’s circulation is sluggish, then because of gravity, that’s where’s going to get blocked first.
In both CAD and PAD, the usual root cause is atherosclerosis, that is to say, the build-up of fatty material inside the arteries, usually commensurate to LDL (“bad”) cholesterol, especially in men (high LDL is still a predictor of cardiovascular disease in women though, just more modestly so, at least pre-menopause or in cases of treated menopause whereby HRT has returned hormones to pre-menopause levels).
See also: Demystifying Cholesterol
And for that about sex differences: His & Hers: The Hidden Complexities of Statins and Cardiovascular Disease (CVD)
Why it is
This one’s straightforward, as it’s the same things as any kind of cardiovascular disease: high blood pressure, high cholesterol, older age, obesity, smoking, drinking, diabetes, and genetic factors (so, a risk factor is: family history of heart disease).
However, while those are the main causes and/or risk factors, it absolutely can still strike other people, so it’s as well to be watch out for…
What to look out for
Many people first notice signs and symptoms that turn out to be PAD when they experience pain or numbness in the foot or feet, and/or a discoloration of the feet (especially toes), and slow wound healing.
At that stage, chances are you will need to go urgently to a specialist, and surgery is a likely necessity. With a little luck, it’ll be a minimally-invasive surgery to unblock an artery; failing that, an amputation will be in order.
At that stage, under 50% will be alive 5 years from diagnosis:
You probably want to avoid those. Good news is, you can, by catching it earlier!
What to look out for before that
The most common test for PAD is one you can do at home, but enlisting a nurse to do it for you will help ensure accurate readings. It’s called the Ankle-Brachial Index (ABI) test, and it involves comparing the blood pressure in your ankle with the blood pressure in your arm, and expressing them as a ratio.
Here’s how to do it (instructions and a video demonstration if you want it):
Do Try This At Home: ABI Test For Clogged Arteries
If you need a blood pressure monitor, by the way, here’s an example product on Amazon.
- A healthy ABI score is between 1.0 and 1.4; anything outside this range may indicate arterial problems.
- Low ABI scores (below 0.8) suggest plaque is likely obstructing blood flow
- High ABI scores (above 1.4) may indicate artery hardening
Do note also that yes, if you have plaque obstructing blood flow and hardened arteries, your scores may cancel out and give you a “healthy” score, despite your arteries being very much not healthy.
For this reason, this test can be used to raise the alarm, but not to give the “all clear”.
There are other tests that clinicians can do for you, but you can’t do at home unless you have an MRI machine, a CT scanner, an x-ray machine, a doppler-and-ultrasound machine, etc. We’ll not go into those in detail here, but ask your doctor about them if you’re concerned.
What to do about it
In the mid-to-late stages of the disease, the options are medication and surgery, respectively, but your doctor will advise about those in that eventuality.
In the early stages of the disease, the first-line recommend treatment is exercise, of which, especially walking:
Lower Extremity Peripheral Artery Disease: Diagnosis and Treatment
Given that this more often happens when someone hasn’t been walking so much, it can be a walk-rest-walk approach at first (a treadmill on a low setting can be very useful for this):
See also: Exercise Comparison Head-to-Head: Treadmill vs Road
Take care!
Share This Post
-

The Sweet Truth About Glycine
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Make Your Collagen Work Better

This is Dr. James Nicolantonio. He’s a doctor of pharmacy, and a research scientist. He has a passion for evidence-based nutrition, and has written numerous books on the subject.
Controversy! Dr. DiNicolatonio’s work has included cardiovascular research, in which field he has made the case for increasing (rather than decreasing) the recommended amount of salt in our diet. This, of course, goes very much against the popular status quo.
We haven’t reviewed that research so we won’t comment on it here, but we thought it worth a mention as a point of interest. We’ll investigate his claims in that regard another time, though!
Today, however, we’ll be looking at his incisive, yet not controversial, work pertaining to collagen and glycine.
A quick recap on collagen
We’ve written about collagen before, and its importance for maintaining… Well, pretty much most of our body, really, buta deficiency in collagen can particularly weaken bones and joints.
On a more surface level, collagen’s also important for healthy elastic skin, and many people take it for that reason alone,
Since collagen is found only in animals, even collagen supplements are animal-based (often marine collagen or bovine collagen). However, if we don’t want to consume those, we can (like most animals) synthesize it ourselves from the relevant amino acids, which we can get from plants (and also laboratories, in some cases).
You can read our previous article about this, here:
We Are Such Stuff As Fish Are Made Of
What does he want us to know about collagen?
We’ll save time and space here: first, he’d like us to know the same as what we said in our article above
However, there is also more:
Let’s assume that your body has collagen to process. You either consumed it, or your body has synthesized it. We’ll skip describing the many steps of collagen synthesis, fascinating as that is, and get to the point:
When our body weaves together collagen fibrils out of the (triple-helical) collagen molecules…
- the cross-linking of the collagen requires lysyl oxidase
- the lysyl oxidase (which we make inside us) deanimates some other amino acids yielding aldehydes that allow the stable cross-links important for the high tensile strength of collagen, but to do that, it requires copper
- in order to use the copper it needs to be in its reduced cuprous form and that requires vitamin C
- but moving it around the body requires vitamin A
So in other words: if you are taking (or synthesizing) collagen, you also need copper and vitamins A and C.
However! Just to make things harder, if you take copper and vitamin C together, it’ll reduce the copper too soon in the wrong place.
Dr. DiNicolantonio therefore advises taking vitamin C after copper, with a 75 minutes gap between them.
What does he want us to know about glycine?
Glycine is one of the amino acids that makes up collagen. Specifically, it makes up every third amino acid in collagen, and even more specifically, it’s also the rate-limiting factor in the formation of glutathione, which is a potent endogenous (i.e., we make it inside us) antioxidant that works hard to fight inflammation inside the body.
What this means: if your joints are prone to inflammation, being glycine-deficient means a double-whammy of woe.
As well as being one of the amino acids most key to collagen production, glycine has another collagen-related role:
First, the problem: as we age, glycated collagen accumulates in the skin and cartilage (that’s bad; there is supposed to be collagen there, but not glycated).
More on glycation and what it is and why it is so bad:
Are You Eating Advanced Glycation End-Products? The Trouble Of The AGEs
Now, the solution: glycine suppresses advanced glycation end products, including the glycation of collagen.
See for example:
With these three important functions of glycine in mind…
Dr. DiNicolantonio therefore advises getting glycine at a dose of 100mg/kg/day. So, if you’re the same size as this rather medium-sized writer, that means 7.2g/day.
Where can I get it?
Glycine is found in many foods, including gelatin for those who eat that, eggs for the vegetarians, and spinach for vegans.
However, if you’d like to simply take it as a supplement, here’s an example product on Amazon
(the above product is not clear whether it’s animal-derived or not, so if that’s important to you, shop around. This writer got some locally that is certified vegan, but is in Europe rather than N. America, which won’t help most of our subscribers)
Note: pure glycine is a white crystalline powder that has the same sweetness as glucose. Indeed, that is how it got its name, from the Greek “γλυκύς”, pronounced /ɡly.kýs/, meaning “sweet”. Yes, same etymology as glucose.
So don’t worry that you’ve been conned if you order it and think “this is sugar!”; it just looks and tastes the same.
That does mean you should buy from a reputable source though, as a con would be very easy!
this does also mean that if you like a little sugar/sweetener in your tea or coffee, glycine can be used as a healthy substitute.
If you don’t like sweet tastes, then, condolences. This writer pours two espresso coffees (love this decaffeinated coffee that actually tastes good), puts the glycine in the first, and then uses the second to get rid of the sweet taste of the first. So that’s one way to do it.
Enjoy (if you can!)
Share This Post
-
Dandelion Greens vs Mustard Greens – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing dandelion greens to mustard greens, we picked the dandelions.
Why?
Despite our best efforts to find something to unseat dandelion greens from the “most nutritious greens” throne, they still come out on top:
In terms of macros, dandelion greens have more fiber, carbs, and protein, making them the most nutritionally dense option in this category.
In the category of vitamins, dandelion greens have more of vitamins B1, B2, B3, B6, B7, B9, C, E, K, and choline, while mustard greens have more vitamin B5 (the vitamin that’s found in all foods). A very clear win for dandelion greens here.
Looking at minerals, dandelion greens have more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, and zinc, while mustard greens have (slightly) more selenium. Another easy win for dandelion greens.
When it comes to polyphenols, we weren’t able to get figures for mustard greens, but we know that dandelion greens have lots and have beaten every other kind of greenery we’ve pitted them against so far. Probably mustard greens are good for this too, but we can’t comment without data.
Adding up the sections (skipping over polyphenols, on account of the absence of data for mustard greens) makes for an overall strong win for dandelion greens, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Share This Post


Related Posts
-

Yoga for Osteoporosis – by Dr. Loren Fishman
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is not your average yoga book. In fact, the yoga poses themselves do not start until chapter nine. So, what’s going on for the first eight chapters?
Written by an MD and professor of physical medicine and rehabilitation, we are first treated to a very in-depth explanation of the anatomy, physiology, histology, pathology, and epidemiology of osteoporosis and many related issues, bones in good health, factors that affect same, how exercise works for bones in far more detail than this reviewer has seen in any book about exercise or osteoporosis, the physics at hand, and an overview of what yoga has going for it in this regard, since usually there is the concern: we want high-impact work to strengthen bones, but in the case of osteoporosis, that can break them, so instead, yoga’s dynamic tension comes into (safe) play.
When we say “more detail”, you will learn like a medical student the many different kinds of cells involved, each with wildly different structures as well as functions, how they react to different stimuli, how they interact with what we eat, and how to leverage all this information to our advantage. We also learn about how bone density, while important, is not the whole story, as bone quality matters a lot too, and this latter category is harder to measure, and/but can indeed be measured (and improved) in various ways.
The yoga itself is presented as various series of many well-illustrated poses, and a six-lesson course to progress through.
The style of the book is clinical and dense (with many scientific references), while still being perfectly comprehensible if one reads it in a methodical cover-to-cover fashion, and thus does not miss important information required for comprehension of later topics.
Bottom line: this is best book on this topic that this reviewer has encountered by far, and is highly recommended to anyone who cares about building and maintaining bone strength.
Click here to check out Yoga For Osteoporosis, and keep your bones safe!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Banana vs Mango – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing banana to mango, we picked the banana.
Why?
In terms of macros, banana has more fiber, carbs, and protein, making it the more nutrient-dense option in this regard.
In the category of vitamins, banana has more of vitamins B1, B2, B5, B6, B7, and choline, while mango has more of vitamins A, B3 B9, C, E, and K; a 6:6 tie here.
When it comes to minerals, banana has more iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while mango has more calcium and copper. A second win for bananas.
Adding up the sections makes for an overall win for bananas, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
What Do The Different Kinds Of Fiber Do? 30 Foods That Rank Highest
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

To tackle gendered violence, we also need to look at drugs, trauma and mental health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
After several highly publicised alleged murders of women in Australia, the Albanese government this week pledged more than A$925 million over five years to address men’s violence towards women. This includes up to $5,000 to support those escaping violent relationships.
However, to reduce and prevent gender-based and intimate partner violence we also need to address the root causes and contributors. These include alcohol and other drugs, trauma and mental health issues.
Why is this crucial?
The World Health Organization estimates 30% of women globally have experienced intimate partner violence, gender-based violence or both. In Australia, 27% of women have experienced intimate partner violence by a co-habiting partner; almost 40% of Australian children are exposed to domestic violence.
By gender-based violence we mean violence or intentionally harmful behaviour directed at someone due to their gender. But intimate partner violence specifically refers to violence and abuse occurring between current (or former) romantic partners. Domestic violence can extend beyond intimate partners, to include other family members.
These statistics highlight the urgent need to address not just the aftermath of such violence, but also its roots, including the experiences and behaviours of perpetrators.
What’s the link with mental health, trauma and drugs?
The relationships between mental illness, drug use, traumatic experiences and violence are complex.
When we look specifically at the link between mental illness and violence, most people with mental illness will not become violent. But there is evidence people with serious mental illness can be more likely to become violent.
The use of alcohol and other drugs also increases the risk of domestic violence, including intimate partner violence.
About one in three intimate partner violence incidents involve alcohol. These are more likely to result in physical injury and hospitalisation. The risk of perpetrating violence is even higher for people with mental ill health who are also using alcohol or other drugs.
It’s also important to consider traumatic experiences. Most people who experience trauma do not commit violent acts, but there are high rates of trauma among people who become violent.
For example, experiences of childhood trauma (such as witnessing physical abuse) can increase the risk of perpetrating domestic violence as an adult.

Childhood trauma can leave its mark on adults years later. Roman Yanushevsky/Shutterstock Early traumatic experiences can affect the brain and body’s stress response, leading to heightened fear and perception of threat, and difficulty regulating emotions. This can result in aggressive responses when faced with conflict or stress.
This response to stress increases the risk of alcohol and drug problems, developing PTSD (post-traumatic stress disorder), and increases the risk of perpetrating intimate partner violence.
How can we address these overlapping issues?
We can reduce intimate partner violence by addressing these overlapping issues and tackling the root causes and contributors.
The early intervention and treatment of mental illness, trauma (including PTSD), and alcohol and other drug use, could help reduce violence. So extra investment for these are needed. We also need more investment to prevent mental health issues, and preventing alcohol and drug use disorders from developing in the first place.
Early intervention and treatment of mental illness, trauma and drug use is important. Okrasiuk/Shutterstock Preventing trauma from occuring and supporting those exposed is crucial to end what can often become a vicious cycle of intergenerational trauma and violence. Safe and supportive environments and relationships can protect children against mental health problems or further violence as they grow up and engage in their own intimate relationships.
We also need to acknowledge the widespread impact of trauma and its effects on mental health, drug use and violence. This needs to be integrated into policies and practices to reduce re-traumatising individuals.
How about programs for perpetrators?
Most existing standard intervention programs for perpetrators do not consider the links between trauma, mental health and perpetrating intimate partner violence. Such programs tend to have little or mixed effects on the behaviour of perpetrators.
But we could improve these programs with a coordinated approach including treating mental illness, drug use and trauma at the same time.
Such “multicomponent” programs show promise in meaningfully reducing violent behaviour. However, we need more rigorous and large-scale evaluations of how well they work.
What needs to happen next?
Supporting victim-survivors and improving interventions for perpetrators are both needed. However, intervening once violence has occurred is arguably too late.
We need to direct our efforts towards broader, holistic approaches to prevent and reduce intimate partner violence, including addressing the underlying contributors to violence we’ve outlined.
We also need to look more widely at preventing intimate partner violence and gendered violence.
We need developmentally appropriate education and skills-based programs for adolescents to prevent the emergence of unhealthy relationship patterns before they become established.
We also need to address the social determinants of health that contribute to violence. This includes improving access to affordable housing, employment opportunities and accessible health-care support and treatment options.
All these will be critical if we are to break the cycle of intimate partner violence and improve outcomes for victim-survivors.
The National Sexual Assault, Family and Domestic Violence Counselling Line – 1800 RESPECT (1800 737 732) – is available 24 hours a day, seven days a week for any Australian who has experienced, or is at risk of, family and domestic violence and/or sexual assault.
If this article has raised issues for you, or if you’re concerned about someone you know, call Lifeline on 13 11 14. In an emergency, call 000.
Siobhan O’Dean, Postdoctoral Research Associate, The Matilda Centre for Research in Mental Health and Substance Use, University of Sydney; Lucinda Grummitt, Postdoctoral Research Fellow, The Matilda Centre for Research in Mental Health and Substance Use, University of Sydney, and Steph Kershaw, Research Fellow, The Matilda Centre for Research in Mental Health and Substance Use, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: