Are You Eating AGEs?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Trouble of the AGEs
Advanced Glycation End-Products (AGEs) are the result of the chemical process of glycation, which can occur in your body in response to certain foods you ate, or you can consume them directly, if you eat animal products that contained them (because we’re not special and other animals glycate too, especially mammals such as pigs, cows, and sheep).
As a double-whammy, if you cook animal products (especially without water, such as by roasting or frying), extra AGEs will form during cooking.
When proteinous and/or fatty food turns yellow/golden/brown during cooking, that’s generally glycation.
If there’s starch present, some or all of that yellow/golden/brown stuff will be a Maillard Reaction Product (MRP), such as acrylamide. That’s not exactly a health food, but it’s nowhere near being even in the same ballpark of badness.
In short, during cooking:
- Proteinous/fatty food turns yellow/golden/brown = probably an AGE
- Starchy food turns yellow/golden/brown = probably a MRP
The AGEs are far worse.
What’s so bad about AGEs?
Let’s do a quick tour of some studies:
- The role of advanced glycation end-products in retinal ageing and disease
- Advanced glycation end-products and their circulating receptors predict cardiovascular disease mortality in older women
- Elevated serum advanced glycation end-products in obese indicate risk for the metabolic syndrome: a link between healthy and unhealthy obesity?
- Increased levels of serum advanced glycation end-products in women with polycystic ovary syndrome
- Advanced glycation end-products and their involvement in liver disease
- Effects of advanced glycation end-products on renal fibrosis and oxidative stress
- Role of advanced glycation end-products and oxidative stress in vascular complications in diabetes
- Cancer malignancy is enhanced by advanced glycation end-products
- Advanced glycation end-products in the pathogenesis of Alzheimer’s disease
We could keep going, but you probably get the picture!
What should we do about it?
There are three main ways to reduce serum AGE levels:
Reduce or eliminate consumption of animal products
Especially mammalian animal products, such as from pigs, cows, and sheep, especially their meat. Processed versions are even worse! So, steak is bad, but bacon and sausages are literally top-tier bad.
Cook wet
Dry cooking (which includes frying, and especially includes deep fat frying, which is worse than shallow frying which is worse than air frying) produces far more AGEs than cooking with methods that involve water (boiling, steaming, slow-cooking, etc).
As a bonus, adding acidic ingredients (e.g. vinegar, lemon juice, tomato juice) can halve the amount of AGEs produced.
Consume antioxidants
Our body does have some ability to deal with AGEs, but that ability has its limits, and our body can be easily overwhelmed if we consume foods that are bad for it. So hopefully you’ll tend towards a plant-based diet, but whether you do or don’t:
You can give your body a hand by consuming antioxidant foods and drinks (such as berries, tea/coffee, and chocolate), and/or taking supplements.
Want to know more about the science of this?
Check out…
Advanced Glycation End-Products in Foods and a Practical Guide to Their Reduction in the Diet
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Hidden Weapon Against Depression (How To Do Behavioral Activation)

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Tracey Marks, psychiatrist, explains:
A cycle of action
Depression is:
- not fun
- self-reinforcing in nature
That is to say: depression disrupts thoughts, feelings, behaviors, and by extension, physical wellbeing. The resultant withdrawal from activities further removes psychological rewards, and worsens depression in a spiralling feedback loop.
Behavioral activation (BA) is an underused but effective intervention that encourages re-engaging in meaningful activities (no matter how little you feel like doing them) to break the cycle of depression.
This is very different from CBT, because instead of changing thoughts directly, it modifies behavior to indirectly improve thinking and self-perception. That said, there’s no reason you can’t do both if you want to, but let’s be reasonable; a person in the throes of depression is usually not leaping at every opportunity with full enthusiasm, so maybe one thing at a time is sufficient.
How it works: even small constructive activities provide positive reinforcement, and can start a healthier loop. Additionally, if applicable (and it’s best if it is), exercise also helps by boosting brain-derived neurotrophic factor (BDNF).
Step-by-step:
- Monitor activity: keep track for a week, noting morning/afternoon/evening activities and mood ratings (e.g. 1–10, or if you use a bullet-journalling app*, then whatever scale it uses is fine), focusing on intentional activities rather than basic bodily functions
- Review activity: identify what boosted or lowered mood, which activities increased connection, and which gave a sense of accomplishment
- Reflect on values: reconnect with core values that give meaning; use assessments or workbooks if needed
- Plan activities: list items from the tracker, your values, essential daily living tasks, and an activity menu for new ideas
- Schedule and commit: use the tracker to plan; expect gradual progress, with motivation and energy increasing over time
*This writer—who has found BA immensely useful personally for getting out of depressive episodes—uses Daylio, which has a customizable 1–5 scale (as well as customizable activities** to track). Personally I modified “3” on the scale to be able to mark two different kinds of “middling” days moodwise; I draw a distinction between days that are middling because they were emotionally flat, and days that were middling because they had a mixture of highs and lows that, for bullet-journalling purposes, cancels out to “middling”. That way, I still get my overall mood chart in the graph, but I can also scroll through my days and see if, for example, I have been emotionally flat for a time (big warning sign of depression) rather than “my day was mixed in nature” (perfectly normal healthy part of the human experience).
**As with Dr. Marks’ advice, I do mostly track intentional activities (e.g. gardening, exercise, wash hair, meditation, see sunrise, see friends, etc), though I also track my sleep (e.g. good sleep, bad sleep, medium sleep, wake early), and some physiological things such as crying, and cramps (because if I track crying for several days and then cramps, I can probably attribute it at least in part to hormones), because these things have bearing on how I then interpret the data—which is part of how the “monitor” and “review” parts of BA work.
One of the great things about BA is that you can do it by yourself, but you also can enlist help, e.g. from a partner, friends, family, etc. When experiencing depression, it’s easy to imagine that either everyone hates you or, at best, nobody cares—but usually there will be people who will be glad to help if given the opportunity.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Behavioral Activation Against Depression & Anxiety
Take care!
Share This Post
-

Say That Again: Using Hearing Aids Can Be Frustrating for Older Adults, but Necessary
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It was an every-other-day routine, full of frustration.
Every time my husband called his father, who was 94 when he died in 2022, he’d wait for his dad to find his hearing aids and put them in before they started talking.
Even then, my father-in-law could barely hear what my husband was saying. “What?” he’d ask over and over.
Then, there were the problems my father-in-law had replacing the devices’ batteries. And the times he’d end up in the hospital, unable to understand what people were saying because his hearing aids didn’t seem to be functioning. And the times he’d drop one of the devices and be unable to find it.
How many older adults have problems of this kind?
There’s no good data about this topic, according to Nicholas Reed, an assistant professor of epidemiology at Johns Hopkins Bloomberg School of Public Health who studies hearing loss. He did a literature search when I posed the question and came up empty.
Reed co-authored the most definitive study to date of hearing issues in older Americans, published in JAMA Open Network last year. Previous studies excluded people 80 and older. But data became available when a 2021 survey by the National Health and Aging Trends Study included hearing assessments conducted at people’s homes.
The results, based on a nationally representative sample of 2,803 people 71 and older, are eye-opening. Hearing problems become pervasive with advancing age, exceeding 90% in people 85 and older, compared with 53% of 71- to 74-year-olds. Also, hearing worsens over time, with more people experiencing moderate or severe deficits once they reach or exceed age 80, compared with people in their 70s.
However, only 29% of those with hearing loss used hearing aids. Multiple studies have documented barriers that inhibit use. Such devices, which Medicare doesn’t cover, are pricey, from nearly $1,000 for a good over-the-counter set (OTC hearing aids became available in 2022) to more than $6,000 for some prescription models. In some communities, hearing evaluation services are difficult to find. Also, people often associate hearing aids with being old and feel self-conscious about wearing them. And they tend to underestimate hearing problems that develop gradually.
Barbara Weinstein, a professor of audiology at the City University of New York Graduate Center and author of the textbook “Geriatric Audiology,” added another concern to this list when I reached out to her: usability.
“Hearing aids aren’t really designed for the population that most needs to use them,” she told me. “The move to make devices smaller and more sophisticated technologically isn’t right for many people who are older.”
That’s problematic because hearing loss raises the risk of cognitive decline, dementia, falls, depression, and social isolation.
What advice do specialists in hearing health have for older adults who have a hard time using their hearing aids? Here are some thoughts they shared.
Consider larger, customized devices. Many older people, especially those with arthritis, poor fine motor skills, compromised vision, and some degree of cognitive impairment, have a hard time manipulating small hearing aids and using them properly.
Lindsay Creed, associate director of audiology practices at the American Speech-Language-Hearing Association, said about half of her older clients have “some sort of dexterity issue, whether numbness or reduced movement or tremor or a lack of coordination.” Shekinah Mast, owner of Mast Audiology Services in Seaford, Delaware, estimates nearly half of her clients have vision issues.
For clients with dexterity challenges, Creed often recommends “behind-the-ear hearing aids,” with a loop over the ear, and customized molds that fit snugly in the ear. Customized earpieces are larger than standardized models.
“The more dexterity challenges you have, the better you’ll do with a larger device and with lots of practice picking it up, orienting it, and putting it in your ear,” said Marquitta Merkison, associate director of audiology practices at ASHA.
For older people with vision issues, Mast sometimes orders hearing aids in different colors for different ears. Also, she’ll help clients set up stands at home for storing devices, chargers, and accessories so they can readily find them each time they need them.
Opt for ease of use. Instead of buying devices that require replacing tiny batteries, select a device that can be charged overnight and operate for at least a day before being recharged, recommended Thomas Powers, a consultant to the Hearing Industries Association. These are now widely available.
People who are comfortable using a smartphone should consider using a phone app to change volume and other device settings. Dave Fabry, chief hearing health officer at Starkey, a major hearing aid manufacturer, said he has patients in their 80s and 90s “who’ve found that being able to hold a phone and use larger visible controls is easier than manipulating the hearing aid.”
If that’s too difficult, try a remote control. GN ReSound, another major manufacturer, has designed one with two large buttons that activate the volume control and programming for its hearing aids, said Megan Quilter, the company’s lead audiologist for research and development.
Check out accessories. Say you’re having trouble hearing other people in restaurants. You can ask the person across the table to clip a microphone to his shirt or put the mike in the center of the table. (The hearing aids will need to be programmed to allow the sound to be streamed to your ears.)
Another low-tech option: a hearing aid clip that connects to a piece of clothing to prevent a device from falling to the floor if it becomes dislodged from the ear.
Wear your hearing aids all day. “The No. 1 thing I hear from older adults is they think they don’t need to put on their hearing aids when they’re at home in a quiet environment,” said Erika Shakespeare, who owns Audiology and Hearing Aid Associates in La Grande, Oregon.
That’s based on a misunderstanding. Our brains need regular, not occasional, stimulation from our environments to optimize hearing, Shakespeare explained. This includes noises in seemingly quiet environments, such as the whoosh of a fan, the creak of a floor, or the wind’s wail outside a window.
“If the only time you wear hearing aids is when you think you need them, your brain doesn’t know how to process all those sounds,” she told me. Her rule of thumb: “Wear hearing aids all your waking hours.”
Consult a hearing professional. Everyone’s needs are different, so it’s a good idea to seek out an audiologist or hearing specialist who, for a fee, can provide guidance.
“Most older people are not going to know what they need” and what options exist without professional assistance, said Virginia Ramachandran, the head of audiology at Oticon, a major hearing aid manufacturer, and a past president of the American Academy of Audiology.
Her advice to older adults: Be “really open” about your challenges.
If you can’t afford hearing aids, ask a hearing professional for an appointment to go over features you should look for in over-the-counter devices. Make it clear you want the appointment to be about your needs, not a sales pitch, Reed said. Audiology practices don’t routinely offer this kind of service, but there’s good reason to ask since Medicare started covering once-a-year audiologist consultations last year.
We’re eager to hear from readers about questions you’d like answered, problems you’ve been having with your care, and advice you need in dealing with the health care system. Visit http://kffhealthnews.org/columnists to submit your requests or tips.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-
Soy Allergy? No Problem! Turn Any Legume Into Tofu (Here’s How)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Legumes have similar chemical composition, which means they can generally be used in the same ways as each other:
Variety is the spice of life
In the video, he demonstrates this with green peas, red lentils, and green lentils, and mentions that it is the same for chickpeas too. The process is:
- Soak 100g dried legumes overnight in plenty of water.
- Drain and blend with 250ml fresh water until smooth.
- Pour into a nonstick frying pan, add ½ tsp salt, and stir.
- Cook until it thickens into a paste, then cook for another 2–3 minutes on low heat.
- Transfer to a 500ml mold, smooth the top, and set in the fridge for 1 hour.
- If properly set, it can be eaten as-is or fried into crispy cubes.
- Stir-fry tofu with: ginger, spring onions, garlic, and chili.
- Sauce: suggestions include soy sauce, rice wine vinegar, mirin, sesame oil.
- Garnish with: sesame and coriander seeds
Science behind it: heating alters protein bonds and starches, forming a thick paste that sets.
Note: legumes contain natural toxins that are destroyed by cooking. For some, like those mentioned above, frying for a few minutes is sufficient. However, kidney beans are high in phytohemagglutinin, which requires at least 20 minutes of cooking to be safe, making them unsuitable for this process.
For more on all of this, plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Six Ways To Eat For Healthier Skin
Take care!
Share This Post


Related Posts
-
I’ve recovered from a cold but I still have a hoarse voice. What should I do?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cold, flu, COVID and RSV have been circulating across Australia this winter. Many of us have caught and recovered from one of these common upper respiratory tract infections.
But for some people their impact is ongoing. Even if your throat isn’t sore anymore, your voice may still be hoarse or croaky.
So what happens to the voice when we get a virus? And what happens after?
Here’s what you should know if your voice is still hoarse for days – or even weeks – after your other symptoms have resolved.
Why does my voice get croaky during a cold?
A healthy voice is normally clear and strong. It’s powered by the lungs, which push air past the vocal cords to make them vibrate. These vibrations are amplified in the throat and mouth, creating the voice we hear.
The vocal cords are two elastic muscles situated in your throat, around the level of your laryngeal prominence, or Adam’s apple. (Although everyone has one, it tends to be more pronounced in males.) The vocal cords are small and delicate – around the size of your fingernail. Any small change in their structure will affect how the voice sounds.
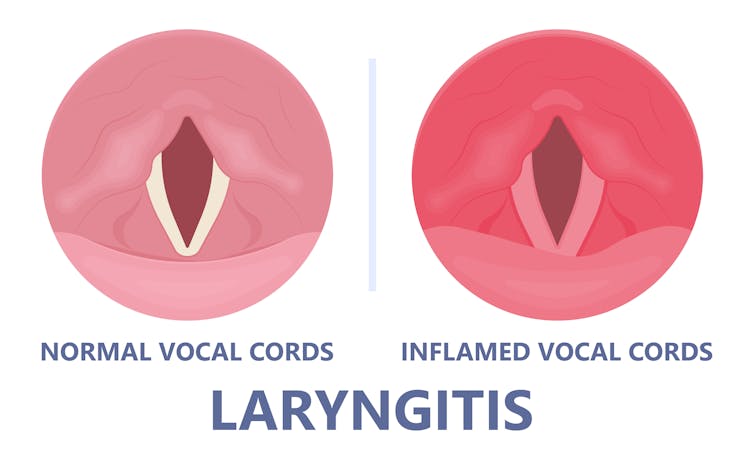
When the vocal cords become inflamed – known as laryngitis – your voice will sound different. Laryngitis is a common part of upper respiratory tract infections, but can also be caused through misuse.

Viruses such as the common cold can inflame the vocal cords. Pepermpron/Shutterstock Catching a virus triggers the body’s defence mechanisms. White blood cells are recruited to kill the virus and heal the tissues in the vocal cords. They become inflamed, but also stiffer. It’s harder for them to vibrate, so the voice comes out hoarse and croaky.
In some instances, you may find it hard to speak in a loud voice or have a reduced pitch range, meaning you can’t go as high or loud as normal. You may even “lose” your voice altogether.
Coughing can also make things worse. It is the body’s way of trying to clear the airways of irritation, including your own mucus dripping onto your throat (post-nasal drip). But coughing slams the vocal cords together with force.
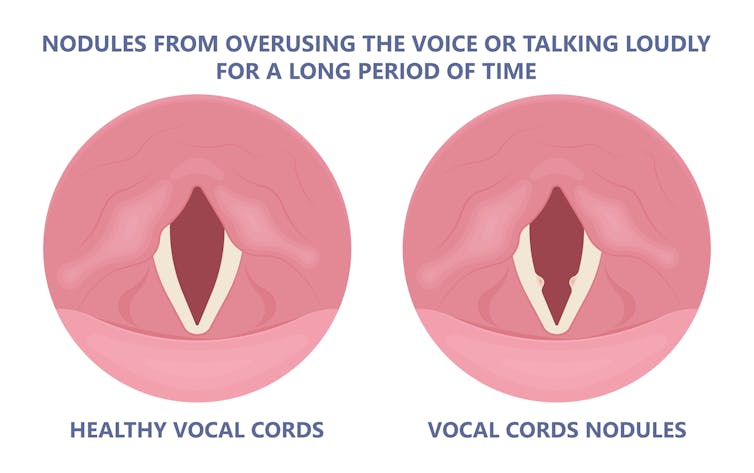
Chronic coughing can lead to persistent inflammation and even thicken the vocal cords. This thickening is the body trying to protect itself, similar to developing a callus when a pair of new shoes rubs.
Thickening on your vocal cords can lead to physical changes in the vocal cords – such as developing a growth or “nodule” – and further deterioration of your voice quality.
Coughing and exertion can cause inflamed vocal cords to thicken and develop nodules. Pepermpron/Shutterstock How can you care for your voice during infection?
People who use their voices a lot professionally – such as teachers, call centre workers and singers – are often desperate to resume their vocal activities. They are more at risk of forcing their voice before it’s ready.
The good news is most viral infections resolve themselves. Your voice is usually restored within five to ten days of recovering from a cold.
Occasionally, your pharmacist or doctor may prescribe cough suppressants to limit additional damage to the vocal cords (among other reasons) or mucolytics, which break down mucus. But the most effective treatments for viral upper respiratory tract infections are hydration and rest.
Drink plenty of water, avoid alcohol and exposure to cigarette smoke. Inhaling steam by making yourself a cup of hot water will also help clear blocked noses and hydrate your vocal cords.
Rest your voice by talking as little as possible. If you do need to talk, don’t whisper – this strains the muscles.
Instead, consider using “confidential voice”. This is a soft voice – not a whisper – that gently vibrates your vocal cords but puts less strain on your voice than normal speech. Think of the voice you use when communicating with someone close by.
During the first five to ten days of your infection, it is important not to push through. Exerting the voice by talking a lot or loudly will only exacerbate the situation. Once you’ve recovered from your cold, you can speak as you would normally.
What should you do if your voice is still hoarse after recovery?
If your voice hasn’t returned to normal after two to three weeks, you should seek medical attention from your doctor, who may refer you to an ear nose and throat specialist.
If you’ve developed a nodule, the specialist would likely refer you to a speech pathologist who will show you how to take care of your voice. Many nodules can be treated with voice therapy and don’t require surgery.
You may have also developed a habit of straining your vocal cords, if you forced yourself to speak or sing while they were inflamed. This can be a reason why some people continue to have a hoarse voice even when they’ve recovered from the cold.
In those cases, a speech pathologist may play a valuable role. They may teach you to exercises that make voicing more efficient. For example, lip trills (blowing raspberries) are a fun and easy way you can learn to relax the voice. This can help break the habit of straining your voice you may have developed during infection.
Yeptain Leung, Postdoctoral Research and Lecturer of Speech Pathology, School of Health Sciences, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
“Not Just Measles”: Whooping Cough Cases Are Soaring as Vaccine Rates Decline
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In the past six months, two babies in Louisiana have died of pertussis, the disease commonly known as whooping cough.
Washington state recently announced its first confirmed death from pertussis in more than a decade.
Idaho and South Dakota each reported a death this year, and Oregon last year reported two as well as its highest number of cases since 1950.
While much of the country is focused on the spiraling measles outbreak concentrated in the small, dusty towns of West Texas, cases of pertussis have skyrocketed by more than 1,500% nationwide since hitting a recent low in 2021 amid the COVID-19 pandemic. Deaths tied to the disease are also up, hitting 10 last year, compared with about two to four in previous years. Cases are on track to exceed that total this year.
Doctors, researchers and public health experts warn that the measles outbreak, which has grown to more than 600 cases, may just be the beginning. They say outbreaks of preventable diseases could get much worse with falling vaccination rates and the Trump administration slashing spending on the country’s public health infrastructure.
National rates for four major vaccines, which had held relatively steady in the years before the COVID-19 pandemic, have fallen significantly since, according to a ProPublica analysis of the most recent federal kindergarten vaccination data. Not only have vaccination rates for measles, mumps and rubella fallen, but federal data shows that so have those for pertussis, diphtheria, tetanus, hepatitis B and polio.
In addition, public health experts say that growing pockets of unvaccinated populations across the country place babies and young children in danger should there be a resurgence of these diseases.
Many medical authorities view measles, which is especially contagious, as the canary in the coal mine, but pertussis cases may also be a warning, albeit one that has attracted far less attention.
“This is not just measles,” said Dr. Adam Ratner, a pediatric infectious diseases doctor in New York City and author of the book “Booster Shots: The Urgent Lessons of Measles and the Uncertain Future of Children’s Health.” “It’s a bright-red warning light.”
At least 36 states have witnessed a drop in rates for at least one key vaccine from the 2013-14 to the 2023-24 school years. And half of states have seen an across-the-board decline in all four vaccination rates. Wisconsin, Utah and Alaska have experienced some of the most precipitous drops during that time, with declines of more than 10 percentage points in some cases.
“There is a direct correlation between vaccination rates and vaccine-preventable disease outbreak rates,” said a spokesperson for the Utah Department of Health and Human Services. “Decreases in vaccination rates will likely lead to more outbreaks of vaccine-preventable diseases in Utah.”
But statewide figures alone don’t provide a full picture. Tucked inside each state are counties and communities with far lower vaccination rates that drive outbreaks.
For example, the whooping cough vaccination rate for kindergartners in Washington state in 2023-24 was 90.2%, slightly below the U.S. rate of 92.3%, federal data shows. But the statewide rate for children 19 to 35 months last year was 65.4%, according to state data. In four counties, that rate was in the 30% range. In one county, it was below 12%.
“My concern is that there is going to be a large outbreak of not just measles, but other vaccine-preventable diseases as well, that’s going to end up causing a lot of harm, and possibly deaths in children and young adults,” said Dr. Anna Durbin, a professor in the Department of International Health at the Johns Hopkins Bloomberg School of Public Health who has spent her career studying vaccines. “And it’s completely preventable.”
The dramatic cuts to public health funding and staffing could heighten the risk. And the elevation of Robert F. Kennedy Jr., a longtime vaccine critic, to the secretary of the federal Department of Health and Human Services, several experts said, has only compounded matters.
The Trump administration has eliminated 20,000 jobs at agencies within HHS, which includes the Centers for Disease Control and Prevention, the nation’s public health agency. And late last month, the administration also cut $11 billion from state and local public health agencies on the front lines of protecting Americans from outbreaks; the administration said the money was no longer necessary after the end of the pandemic.
Several city and county public health officials had to move quickly to lay off nurses, epidemiologists and disease inspectors. Some ceased vaccination clinics, halted wastewater surveillance programs and even terminated a contract with the courier service that transports specimens to state labs to test for infectious diseases. One Minnesota public health agency, which had provided 1,400 shots for children at clinics last year, immediately stopped those clinics when the directive arrived, court records show.
A federal judge temporarily barred HHS from enacting the cuts, but the ruling, which came more than a week after the grants were terminated, was too late for programs that had already been canceled and employees who had already been laid off. Lawyers for HHS have asked the judge to reconsider her decision in light of a recent Supreme Court ruling that allowed the Department of Education to terminate grants for teacher training while that case is being argued in lower courts. The judge in the HHS case has not yet ruled on the motion.
But in tiny storefronts and cozy homes, at school fairs and gas stations, many residents in West Texas, near where the measles outbreak has taken hold, appear unfazed.
“I don’t need a vaccine,” one man sitting on his porch said recently. “I don’t get sick.”
“It’s measles. It’s been around forever,” said a woman making her way to her car. “I don’t think it’s a big deal.”
When asked why they weren’t planning on vaccinating their baby, a husband walking alongside his wife who was 27 weeks pregnant simply said, “It’s God’s will.”
In word and deed, Kennedy has sown doubt about immunizations.
In response to the measles outbreak, Kennedy initially said in a column he wrote for Fox News that the decision to vaccinate is a “personal one.” HHS sent doses of vitamin A alongside vaccines to Texas, and Kennedy praised the use of cod liver oil. Only the vaccine prevents measles.
About a week later, in an interview on Fox News, while Kennedy encouraged vaccines, he said he was a “freedom of choice person.” At the same time, he emphasized the risks of the vaccine.
Only after the second measles death in Texas did Kennedy post on X, formerly known as Twitter, that the “most effective way to prevent the spread of measles is the MMR vaccine.”
But even that is not the unequivocal message that the head of HHS should be sending, said Ratner, the infectious diseases doctor in New York. It is, he said, a tepid recommendation at best.
“It gives the impression that these things are equivalent, that you can choose one or the other, and that is disingenuous,” he said. “We don’t have a treatment for measles. We have vitamin A, which we can give to kids with measles, that decreases but doesn’t eliminate the risk of severe outcomes. It doesn’t do anything for prevention of measles.”
In the past, Kennedy has been a fierce critic of the vaccine. In a foreword to a 2021 book on measles released by the nonprofit that he founded, Kennedy wrote, “Measles outbreaks have been fabricated to create fear that in turn forces government officials to ‘do something.’ They then inflict unnecessary and risky vaccines on millions of children for the sole purpose of fattening industry profits.”
A spokesperson for HHS said, “Secretary Kennedy is not anti-vaccine — he is pro-safety, pro-transparency and pro-accountability.” Kennedy, the spokesperson said, responded to the measles outbreak with “clear guidance that vaccines are the most effective way to prevent measles” and under his leadership, the CDC updated its pediatric patient management protocol for measles to include physician-administered vitamin A.
Kennedy, the spokesperson added, “is uniquely qualified to lead HHS at this pivotal moment.”
Late last month, leaders at the CDC ordered staff to bury a risk assessment that emphasized the need for vaccines in response to the measles outbreak — in spite of the fact the CDC has long promoted vaccinations as a cornerstone of public health. While a CDC spokesperson acknowledged that vaccines offer the best protection from measles, she also repeated a line Kennedy had used: “The decision to vaccinate is a personal one.”
Among the approximately 2,400 jobs eliminated at the CDC was a team in the Immunization Services Division that partnered with organizations to promote access to and confidence in vaccines in communities where coverage lagged.
The National Institutes of Health, which is also under HHS, recently ended funding for studies that examine vaccine hesitancy. In early April, researchers, the American Public Health Association and one of the largest unions in the country sued the NIH and its director, Jay Bhattacharya, along with HHS and Kennedy, alleging they terminated grants “without scientifically-valid explanation or cause.” The government hasn’t filed a response in the case.
The NIH cancellation notices stated that the agency’s policy was not to prioritize research that focuses on “gaining scientific knowledge on why individuals are hesitant to be vaccinated and/or explore ways to improve vaccine interest and commitment.”
“These grants are being canceled in the midst of an outbreak, a vaccine-preventable outbreak,” said Rupali Limaye, an associate professor at George Mason University who has spent the past decade studying vaccine hesitancy. “We need to better understand why people are not accepting vaccines now more than ever. This outbreak is still spreading.”
That vaccines prevent diseases is settled science. For decades, there was a societal understanding that getting vaccinated benefited not only the person who got the shot, but also the broader community, especially babies or people with weakened immune systems, like those in chemotherapy.
An investment in public health and a sustained, large-scale approach to vaccines is what helped the country declare the elimination of the measles in 2000, said Lori Tremmel Freeman, the CEO of the National Association of County and City Health Officials.
But she has watched both deteriorate over the last few months. Nearly every morning since notices of the federal funding cuts began going out to local public health agencies, she has woken up to texts from panicked public health workers. She has led daily calls with local health departments and sat in on multiple emergency board meetings.
Freeman has compiled a list of more than 100 direct consequences of the cuts, including one rural health department in the Midwest that can no longer carry out immunization services. That’s vital because there are no hospitals in the county and all public health duties fall to the health department.
“It’s relentless,” she said. “It feels like a barrage and assault on public health.”
More than 1,600 miles away from Washington, D.C., in Lubbock, Texas, the director of the city’s health department, Katherine Wells, sighed last week when she saw the most recent measles numbers. She would have to alert her staff to work late again.
“There’s a lot of cases,” she said, “and we continue to see more and more cases.”
She didn’t know it at the time, but that night would mark the state’s second measles death this year. An earlier death in February was the country’s first in a decade. Both children were not vaccinated.
Kennedy said he traveled to Gaines County to comfort the family who lost their 8-year-old daughter and while there met with the family of the 6-year-old girl who died in February.
He also visited with two local doctors he described as “extraordinary healers,” he said in his post on X. The men, he claimed, have “treated and healed some 300 measles-stricken Mennonite children” using aerosolized budesonide — typically used to prevent symptoms of asthma — and clarithromycin — an antibiotic. Medical experts said neither is an effective measles treatment.
State health officials have traced about two-thirds of the measles cases in Texas to Gaines County, which sits on the western edge of the state.
Seminole, one of the county’s only two incorporated towns, has emerged as the epicenter of the outbreak, with Tina Siemens acting as a community ambassador of sorts.
Siemens, a tall woman with glasses and a short blonde bob, runs a museum that combines the area’s Native American history and Mennonite community with traditional skills like calligraphy and canning fruit.
On a recent Tuesday, atop the museum’s dark coffee table, notes scrawled onto white paper listed the latest shipments of vitamin C and Alaskan cod liver oil.
The supplies, Siemens said, were for one of the local doctors who met with Kennedy.
As measles tears through the community, Siemens said families have to decide whether to get vaccinated.
“In America, we have a choice,” she said, echoing Kennedy’s messaging. “The cod liver oil that was flown in, the vitamin C that was flown in, was a great help.”
Dr. Philip Huang, director and health authority for the Dallas County Health and Human Services Department, is working to keep the measles outbreak from reaching his community, just five hours east of Seminole. He wrote letters to the public school superintendents and leaders of private schools that had large numbers of unvaccinated or undervaccinated students offering to set up mobile vaccine clinics for them.
“Overall, the rates can look OK,” he said, “but when you’ve got these pockets of unvaccinated, that’s where the vulnerability lies.”
Huang has had to lay off 11 full-time employees, 10 temporary workers and cancel more than 50 vaccine clinics following the HHS cuts. The systemic dismantling of the CDC and other federal health agencies, he said, will have a grave and lasting impact.
“This is setting us back decades,” Huang said. “Everyone should be extremely concerned about what’s going on.”
Across the country, pediatricians are petrified, said Dr. Susan Kressly, who serves as president of the American Academy of Pediatrics, the largest professional organization of pediatricians in the country.
“Many of us are losing sleep,” Kressly said. “If we lose that progress, children will pay the price.”
She’s carefully watching the spread of several vaccine-preventable diseases, including an increase in whooping cases that far outpace the typical peaks seen every few years. Although the whooping cough vaccine isn’t as effective as the ones for measles and protection wanes over time, the CDC says it remains the best way to prevent the disease.
Babies under the age of 1 are among the most at risk of severe complications from whooping cough, including slowed or stopped breathing and pneumonia, according to the CDC. About one-third of infants who get whooping cough end up in the hospital. Newborns are especially vulnerable because the CDC doesn’t recommend the first shot until two months. That’s why experts recommend pregnant mothers and anyone who will be around the baby to get vaccinated.
The number of whooping cough cases dropped significantly during the pandemic, but it exploded in recent years. In 2021, the CDC reported 2,116 cases; last year, there were 35,435.
The numbers this year appear set to eclipse 2024. So far in 2025, 7,111 cases have been reported, which is more than double this time last year. Cases tend to spike in the summer and fall, which adds to experts’ concern about high numbers so early in the year.
States on the Pacific Coast and in the Midwest have reported the most cases this year, with Washington leading the country with 742 cases so far, more than five times as many as at this time last year.
The Washington child who died of whooping cough had no underlying medical conditions, according to a spokesperson for the Spokane Regional Health District. The death was announced in February but occurred in November.
While Washington’s overall vaccination rate for whooping cough has remained relatively steady over the last decade at around 90%, pockets of low vaccination rates have allowed the disease to take root and put the wider community at risk, said Dr. Tao Sheng Kwan-Gett, a pediatrician and chief health officer of the Washington State Department of Health.
This is the time to strengthen the public health system, he said, to build trust in those areas and make it easier for children to get their routine vaccines.
“But instead, we’re seeing the exact opposite happen,” he said. “We’re weakening our public health system, and that will put us on a path towards more illness and shorter lives.”
Washington was one of 23 states and the District of Columbia that sued HHS and Kennedy following the $11 billion cuts, which rescinded approximately $118 million from the state. Doing so, the state said in court records, would impact 150 full-time employees and cause an immediate reduction in the agency’s ability to respond to outbreaks.
Washington’s Care-A-Van, a mobile health clinic that travels across the state to provide vaccinations, conduct blood pressure screenings and distribute opioid overdose kits, was a key element in the department’s vaccination efforts.
But that, too, has been diminished.
An alert on the department’s website cataloged the impact.
“Attention,” it began.
As a result of the unexpected decision to terminate grant funding, “all Care-A-Van operations have been paused indefinitely, including the cancellation of more than 104 upcoming clinics across the state.”
The department had anticipated providing approximately 2,000 childhood vaccines as part of that effort.
The frustration came through in Kwan-Gett’s voice. Many people think that federal cuts to public health mean shrinking the federal workforce, he said, but those clawbacks also get passed down to states and cities and counties. The less federal support that trickles down to the local level, the less protected communities will be.
“It really breaks my heart,” he said, “when I see children suffering from preventable diseases like whooping cough and measles when we have the tools to prevent them.”
ProPublica is a Pulitzer Prize-winning investigative newsroom. Sign up for The Big Story newsletter to receive stories like this one in your inbox.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Climate Change Threatens the Mental Well-Being of Youths. Here’s How To Help Them Cope.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve all read the stories and seen the images: The life-threatening heat waves. The wildfires of unprecedented ferocity. The record-breaking storms washing away entire neighborhoods. The melting glaciers, the rising sea levels, the coastal flooding.
As California wildfires stretch into the colder months and hurricane survivors sort through the ruins left by floodwaters, let’s talk about an underreported victim of climate change: the emotional well-being of young people.
A nascent but growing body of research shows that a large proportion of adolescents and young adults, in the United States and abroad, feel anxious and worried about the impact of an unstable climate in their lives today and in the future.
Abby Rafeek, 14, is disquieted by the ravages of climate change, both near her home and far away. “It’s definitely affecting my life, because it’s causing stress thinking about the future and how, if we’re not addressing the problem now as a society, our planet is going to get worse,” says Abby, a high school student who lives in Gardena, California, a city of 58,000 about 15 miles south of downtown Los Angeles.
She says wildfires are a particular worry for her. “That’s closer to where I live, so it’s a bigger problem for me personally, and it also causes a lot of damage to the surrounding areas,” she says. “And also, the air gets messed up.”
In April, Abby took a survey on climate change for kids ages 12-17 during a visit to the emergency room at Children’s Hospital of Orange County.
Rammy Assaf, a pediatric emergency physician at the hospital, adapted the survey from one developed five years ago for adults. He administered his version last year to over 800 kids ages 12-17 and their caregivers. He says initial results show climate change is a serious cause of concern for the emotional security and well-being of young people.
Assaf has followed up with the kids to ask more open-ended questions, including whether they believe climate change will be solved in their lifetimes; how they feel when they read about extreme climate events; what they think about the future of the planet; and with whom they are able to discuss their concerns.
“When asked about their outlook for the future, the first words they will use are helpless, powerless, hopeless,” Assaf says. “These are very strong emotions.”
Assaf says he would like to see questions about climate change included in mental health screenings at pediatricians’ offices and in other settings where children get medical care. The American Academy of Pediatrics recommends that counseling on climate change be incorporated into the clinical practice of pediatricians and into medical school curriculums, but not with specific regard to mental health screening.
Assaf says anxiety about climate change intersects with the broader mental health crisis among youth, which has been marked by a rise in depression, loneliness, and suicide over the past decade, though there are recent signs it may be improving slightly.
A 2022 Harris Poll of 1,500 U.S. teenagers found that 89% of them regularly think about the environment, “with the majority feeling more worried than hopeful.” In addition, 69% said they feared they and their families would be affected by climate change in the near future. And 82% said they expected to have to make key life decisions — including where to live and whether to have children — based on the state of the environment.
And the impact is clearly not limited to the U.S. A 2021 survey of 10,000 16- to 25-year-olds across 10 countries found “59% were very or extremely worried and 84% were at least moderately worried” about climate change.
Susan Clayton, chair of the psychology department at the College of Wooster in Ohio, says climate change anxiety may be more pronounced among younger people than adults. “Older adults didn’t grow up being as aware of climate change or thinking about it very much, so there’s still a barrier to get over to accept it’s a real thing,” says Clayton, who co-created the adult climate change survey that Assaf adapted for younger people.
By contrast, “adolescents grew up with it as a real thing,” Clayton says. “Knowing you have the bulk of your life ahead of you gives you a very different view of what your life will be like.” She adds that younger people in particular feel betrayed by their government, which they don’t think is taking the problem seriously enough, and “this feeling of betrayal is associated with greater anxiety about the climate.”
Abby believes climate change is not being addressed with sufficient resolve. “I think if we figure out how to live on Mars and explore the deep sea, we could definitely figure out how to live here in a healthy environment,” she says.
If you are a parent whose children show signs of climate anxiety, you can help.
Louise Chawla, professor emerita in the environmental design program at the University of Colorado-Boulder, says the most important thing is to listen in an open-ended way. “Let there be space for kids to express their emotions. Just listen to them and let them know it’s safe to express these emotions,” says Chawla, who co-founded the nonprofit Growing Up Boulder, which works with the city’s schools to encourage kids to engage civically, including to help shape their local environment.
Chawla and others recommend family activities that reinforce a commitment to the environment. They can be as simple as walking or biking and participating in cleanup or recycling efforts. Also, encourage your children to join activities and advocacy efforts sponsored by environmental, civic, or religious organizations.
Working with others can help alleviate stress and feelings of powerlessness by reassuring kids they are not alone and that they can be proactive.
Worries about climate change should be seen as a learning opportunity that might even lead some kids to their life’s path, says Vickie Mays, professor of psychology and health policy at UCLA, who teaches a class on climate change and mental health — one of eight similar courses offered recently at UC campuses.
“We should get out of this habit of ‘everything’s a mental health problem,’” Mays says, “and understand that often a challenge, a stress, a worry can be turned into advocacy, activism, or a reach for new knowledge to change the situation.”
This article was produced by KFF Health News, which publishes California Healthline, an editorially independent service of the California Health Care Foundation.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: