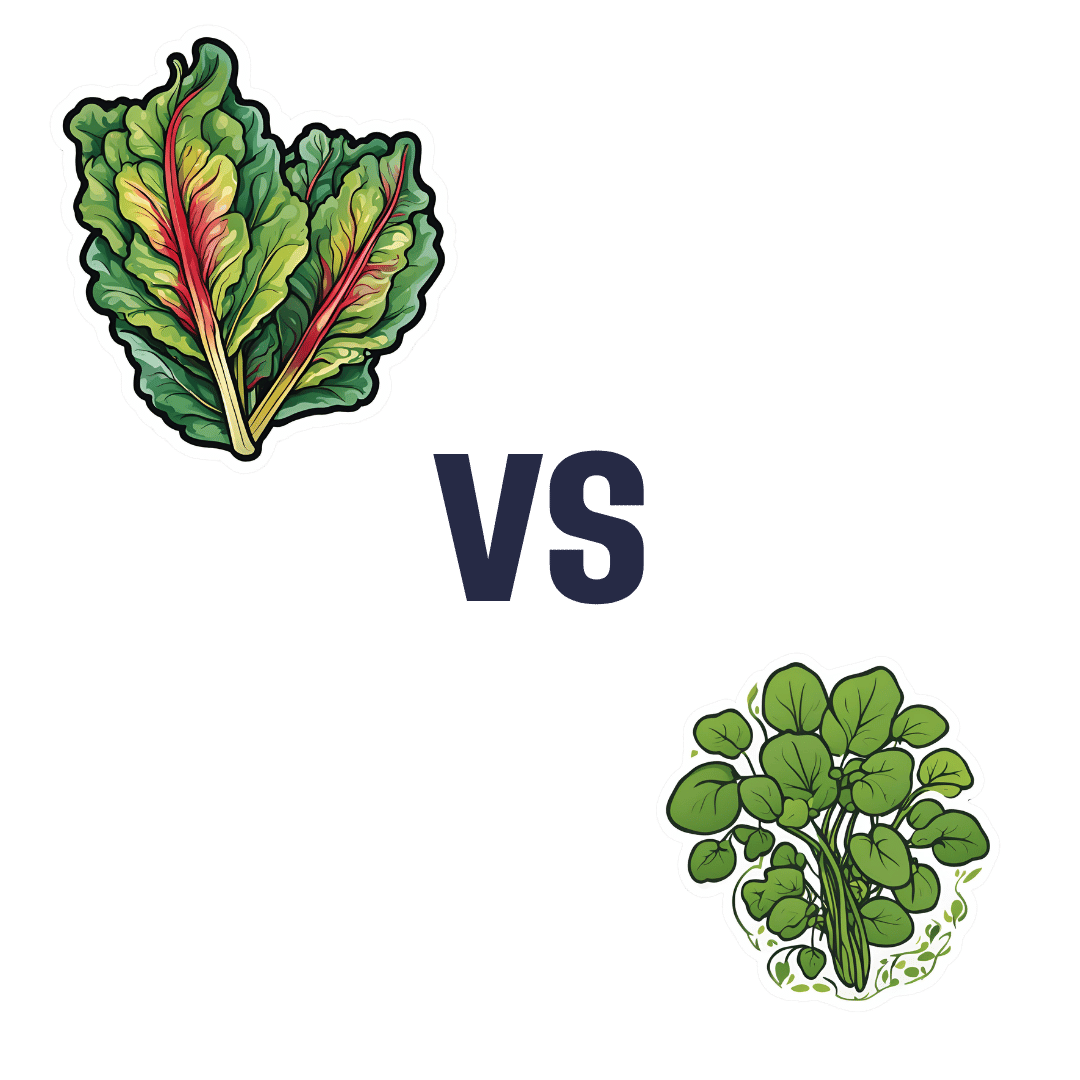
Chard vs Watercress – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing chard to watercress, we picked the chard.
Why?
In terms of macros, chard has more than 3x the fiber as well as slightly more carbs, while watercress has a tiny bit more protein. Given the relative sizes of the numbers involved, we say this one adds up to a modest first-round win for chard.
In the category of vitamins, chard has more of vitamins A, B3, B7, B9, E, and K, while watercress has more of vitamins B1, B2, B5, B6, and C, giving chard a marginal 6:5 win here.
Looking at minerals, chard has more copper, iron, magnesium, manganese, potassium, and zinc, while watercress has more calcium and phosphorus, yielding to chard a 6:2 win in this round.
In other considerations, chard is also notably higher in polyphenols, including top-tier ones like kaempferol and quercetin, so that’s another round in its favor.
Adding up the sections makes for a clear overall win for chard, but by all means enjoy either or both, as diversity is best!
Want to learn more?
You might like:
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Insights into Osteoporosis

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I would like to see some articles on osteoporosis❞
You might enjoy this mythbusting main feature we did a few weeks ago!
Share This Post
-

Why scrapping the term ‘long COVID’ would be harmful for people with the condition
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The assertion from Queensland’s chief health officer John Gerrard that it’s time to stop using the term “long COVID” has made waves in Australian and international media over recent days.
Gerrard’s comments were related to new research from his team finding long-term symptoms of COVID are similar to the ongoing symptoms following other viral infections.
But there are limitations in this research, and problems with Gerrard’s argument we should drop the term “long COVID”. Here’s why.
A bit about the research
The study involved texting a survey to 5,112 Queensland adults who had experienced respiratory symptoms and had sought a PCR test in 2022. Respondents were contacted 12 months after the PCR test. Some had tested positive to COVID, while others had tested positive to influenza or had not tested positive to either disease.
Survey respondents were asked if they had experienced ongoing symptoms or any functional impairment over the previous year.
The study found people with respiratory symptoms can suffer long-term symptoms and impairment, regardless of whether they had COVID, influenza or another respiratory disease. These symptoms are often referred to as “post-viral”, as they linger after a viral infection.
Gerrard’s research will be presented in April at the European Congress of Clinical Microbiology and Infectious Diseases. It hasn’t been published in a peer-reviewed journal.
After the research was publicised last Friday, some experts highlighted flaws in the study design. For example, Steven Faux, a long COVID clinician interviewed on ABC’s television news, said the study excluded people who were hospitalised with COVID (therefore leaving out people who had the most severe symptoms). He also noted differing levels of vaccination against COVID and influenza may have influenced the findings.
In addition, Faux pointed out the survey would have excluded many older people who may not use smartphones.
The authors of the research have acknowledged some of these and other limitations in their study.
Ditching the term ‘long COVID’
Based on the research findings, Gerrard said in a press release:
We believe it is time to stop using terms like ‘long COVID’. They wrongly imply there is something unique and exceptional about longer term symptoms associated with this virus. This terminology can cause unnecessary fear, and in some cases, hypervigilance to longer symptoms that can impede recovery.
But Gerrard and his team’s findings cannot substantiate these assertions. Their survey only documented symptoms and impairment after respiratory infections. It didn’t ask people how fearful they were, or whether a term such as long COVID made them especially vigilant, for example.

Tens of thousands of Australians, and millions of people worldwide, have long COVID.
New Africa/ShutterstockIn discussing Gerrard’s conclusions about the terminology, Faux noted that even if only 3% of people develop long COVID (the survey found 3% of people had functional limitations after a year), this would equate to some 150,000 Queenslanders with the condition. He said:
To suggest that by not calling it long COVID you would be […] somehow helping those people not to focus on their symptoms is a curious conclusion from that study.
Another clinician and researcher, Philip Britton, criticised Gerrard’s conclusion about the language as “overstated and potentially unhelpful”. He noted the term “long COVID” is recognised by the World Health Organization as a valid description of the condition.
A cruel irony
An ever-growing body of research continues to show how COVID can cause harm to the body across organ systems and cells.
We know from the experiences shared by people with long COVID that the condition can be highly disabling, preventing them from engaging in study or paid work. It can also harm relationships with their friends, family members, and even their partners.
Despite all this, people with long COVID have often felt gaslit and unheard. When seeking treatment from health-care professionals, many people with long COVID report they have been dismissed or turned away.
Last Friday – the day Gerrard’s comments were made public – was actually International Long COVID Awareness Day, organised by activists to draw attention to the condition.
The response from people with long COVID was immediate. They shared their anger on social media about Gerrard’s comments, especially their timing, on a day designed to generate greater recognition for their illness.
Since the start of the COVID pandemic, patient communities have fought for recognition of the long-term symptoms many people faced.
The term “long COVID” was in fact coined by people suffering persistent symptoms after a COVID infection, who were seeking words to describe what they were going through.
The role people with long COVID have played in defining their condition and bringing medical and public attention to it demonstrates the possibilities of patient-led expertise. For decades, people with invisible or “silent” conditions such as ME/CFS (myalgic encephalomyelitis/chronic fatigue syndrome) have had to fight ignorance from health-care professionals and stigma from others in their lives. They have often been told their disabling symptoms are psychosomatic.
Gerrard’s comments, and the media’s amplification of them, repudiates the term “long COVID” that community members have chosen to give their condition an identity and support each other. This is likely to cause distress and exacerbate feelings of abandonment.
Terminology matters
The words we use to describe illnesses and conditions are incredibly powerful. Naming a new condition is a step towards better recognition of people’s suffering, and hopefully, better diagnosis, health care, treatment and acceptance by others.
The term “long COVID” provides an easily understandable label to convey patients’ experiences to others. It is well known to the public. It has been routinely used in news media reporting and and in many reputable medical journal articles.
Most importantly, scrapping the label would further marginalise a large group of people with a chronic illness who have often been left to struggle behind closed doors.

Deborah Lupton, SHARP Professor, Vitalities Lab, Centre for Social Research in Health and Social Policy Centre, and the ARC Centre of Excellence for Automated Decision-Making and Society, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

More Salt, Not Less?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I’m curious about the salt part – learning about LMNT and what they say about us needing more salt than what’s recommended by the government, would you mind looking into that? From a personal experience, I definitely noticed a massive positive difference during my 3-5 day water fasts when I added salt to my water compared to when I just drank water. So I’m curious what the actual range for salt intake is that we should be aiming for.❞
That’s a fascinating question, and we’ll have to tackle it in several parts:
When fasting
3–5 days is a long time to take only water; we’re sure you know most people fast from food for much less time than that. Nevertheless, when fasting, the body needs more water than usual—because of the increase in metabolism due to freeing up bodily resources for cellular maintenance. Water is necessary when replacing cells (most of which are mostly water, by mass), and for ferrying nutrients around the body—as well as escorting unwanted substances out of the body.
Normally, the body’s natural osmoregulatory process handles this, balancing water with salts of various kinds, to maintain homeostasis.
However, it can only do that if it has the requisite parts (e.g. water and salts), and if you’re fasting from food, you’re not replenishing lost salts unless you supplement.
Normally, monitoring our salt intake can be a bit of a guessing game, but when fasting for an entire day, it’s clear how much salt we consumed in our food that day: zero
So, taking the recommended amount of sodium, which varies but is usually in the 1200–1500mg range (low end if over aged 70+; high end if aged under 50), becomes sensible.
More detail: How Much Sodium You Need Per Day
See also, on a related note:
When To Take Electrolytes (And When We Shouldn’t!)
When not fasting
Our readers here are probably not “the average person” (since we have a very health-conscious subscriber-base), but the average person in N. America consumes about 9g of salt per day, which is several multiples of the maximum recommended safe amount.
The WHO recommends no more than 5g per day, and the AHA recommends no more than 2.3g per day, and that we should aim for 1.5g per day (this is, you’ll note, consistent with the previous “1200–1500mg range”).
Read more: Massive efforts needed to reduce salt intake and protect lives
Questionable claims
We can’t speak for LMNT (and indeed, had to look them up to discover they are an electrolytes supplement brand), but we can say that sometimes there are articles about such things as “The doctor who says we should eat more salt, not less”, and that’s usually about Dr. James DiNicolantonio, a doctor of pharmacy, who wrote a book that, because of this question today, we’ve now also reviewed:
Spoiler, our review was not favorable.
The body knows
Our kidneys (unless they are diseased or missing) do a full-time job of getting rid of excess things from our blood, and dumping them into one’s urine.
That includes excess sugar (which is how diabetes was originally diagnosed) and excess salt. In both cases, they can only process so much, but they do their best.
Dr. DiNicolantino recognizes this in his book, but chalks it up to “if we do take too much salt, we’ll just pass it in urine, so no big deal”.
Unfortunately, this assumes that our kidneys have infinite operating capacity, and they’re good, but they’re not that good. They can only filter so much per hour (it’s about 1 liter of fluids). Remember we have about 5 liters of blood, consume 2–3 liters of water per day, and depending on our diet, several more liters of water in food (easy to consume several more liters of water in food if one eats fruit, let alone soups and stews etc), and when things arrive in our body, the body gets to work on them right away, because it doesn’t know how much time it’s going to have to get it done, before the next intake comes.
It is reasonable to believe that if we needed 8–10g of salt per day, as Dr. DiNicolantonio claims, our kidneys would not start dumping once we hit much, much lower levels in our blood (lower even than the daily recommended intake, because not all of the salt in our body is in our blood, obviously).
See also: How Too Much Salt Can Lead To Organ Failure
Lastly, a note about high blood pressure
This is one where the “salt’s not the bad guy” crowd have at least something close to a point, because while salt is indeed still a bad guy (if taken above the recommended amounts, without good medical reason), when it comes to high blood pressure specifically, it’s not the worst bad guy, nor is it even in the top 5:
Hypertension: Factors Far More Relevant Than Salt
Thanks for writing in with such an interesting question!
Share This Post



Related Posts
-

Avocado or Papaya – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing avocado to papaya, we picked the avocado.
Why?
Both are great! But…
In terms of macros, avocado has 4x the fiber and 4x the protein as well as 56x the fat (famously healthy fats, mostly monounsaturated, including a complement of omega-3s), while papaya has slightly more carbs. An easy first-round win for avocado.
In the category of vitamins, avocado has more of vitamins B1, B2, B3, B5, B6, B7, B9, E, and K, while papaya has more of vitamins A and C; another clear win for avocado.
Looking at minerals, avocado has more copper, iron, magnesium, manganese, phosphorus, potassium, and zinc, while papaya has more calcium and selenium; a third win in a row for avocado.
Adding up the sections makes for a clear overall win for avocado, but by all means enjoy either or both, as diversity is good!
Want to learn more?
You might like:
What Omega-3 Fatty Acids Really Do For Us
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How Many Steps Per Day To Beat Alzheimer’s? (A Lot Fewer Than You Might Think)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Walking is good for the health” is not, of course, breaking news.
“Exercise helps keep Alzheimer’s at bay”, meanwhile, is something that probably most people don’t know, but regular 10almonds readers certainly will.
There are numerous reasons, and the first and foremost is that “what’s good for your heart is good for your brain” (because the heart feeds the brain, and also ultimately clears away detritus, including the amyloid-β famously associated with Alzheimer’s).
For more on how this works, see: What’s Your Vascular Dementia Risk? ← includes actual numbers and a risk calculator tool and things like that
How many steps?
We previously wrote about merely moving one’s body enough to not be considered to have a “sedentary lifestyle” is already hugely beneficial.
How To Walk Away From Alzheimer’s ← this is less about how much you exercise or how intensely, and more about how much time you spend simply “not sitting”. So, for example, walking.
Most recently, researchers (Dr. Wendy Yau et al.) found that regular walking, even in modest amounts, help build cognitive resilience and delay symptom onset in preclinical Alzheimer’s disease.
How modest? To put it in numbers,
- walking under 3,000 steps/day meant faster buildup of amyloid-β and tau proteins, and quicker cognitive and functional decline.
- walking 3,000–5,000 steps/day delayed cognitive decline by about 3 years.
- walking 5,000–7,500 steps/day delayed decline by about 7 years.
In other words, even a day in which you just amble around the house, perhaps doing some housework, can probably clock up 3,000 steps per day, and is already beneficial.
Of course, more is better; as you can clearly see, there’s a dose-dependent response, at least up as far as 7,500 steps/day.
To quote Dr. Yau herself,
❝Every step counts—and even small increases in daily activities can build over time to create sustained changes in habit and health.❞
Read the paper in full: Physical activity as a modifiable risk factor in preclinical Alzheimer’s disease
As for that “build over time” part, this is very important too. For example another study recently found that being physically active over long periods (not just sporadically) was mostly strongly linked to maintaining better cognitive health. and that the more often and longer people stayed active, the stronger the protective effect became—which means that yes, those benefits grew over time.
You can read that paper in full too, here: Long-term cumulative physical activity associated with less cognitive decline: Evidence from a 16-year cohort study
So with that in mind, you might want to check out: No-Exercise Exercise! ← for ways to get that regular physical activity in, without it feeling like you are doing so
There are more things you can do too, of course; exercise is not the only tool available (albeit it is a critical one).
For a more comprehensive overview of anti-Alzheimer’s tools, enjoy: How To Reduce Your Alzheimer’s Risk
Want to learn more?
You might like this book that we reviewed a little while back:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Avoid This Food To Avoid IBS
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you have inflammatory bowel syndrome (IBS), including ulcerative colitis, Crohn’s disease, or similar, then suddenly a lot of common dietary advice gets flipped on its head:
While resistant starches and the like (so, doing the job of fiber; see: When Is A Fiber Not A Fiber? When It’s A Resistant Starch) making it to the end parts of our digestive tract is good for our bacteria there, in the case of people with IBS or similar, it can be a bit too good for our bacteria there.
As a result, a common understanding is “if you have IBS, you mustn’t eat fiber” which is understandable—but incorrect—advice. More on that in the “Learn more” bit at the bottom, but for now…
What’s the actual biggest driver of IBS?
Another reason to skip red meat
Researchers (Dr. Chunbao Li et al.) noted that relevant epidemiological studies (of which, The China Study is the most famous, but there are countless others) have long shown a strong association between red meat consumption and the development of IBS, and wanted to ascertain how exactly this happened.
This is critical, because while epidemiological studies can present an overwhelming amount of evidence for association/correlation, they cannot outright prove causality.
So, they did a mouse study (mice are opportunistic omnivores like us, indeed often eating our* food, and as a result, have very similar gut microbiota), experimenting with dietary modifications, and then measuring colonic inflammation.
*The mice may disagree, and contest that it is we who are eating their food. But they are free to argue that in their own publication.
What they (the researchers, not the mice) did: they fed the mice red meat diets (beef, pork, lamb) or control for 2 weeks, followed by an induction of colitis.
What they found: red meat diets (all of them) worsened colonic inflammation, increased pro-inflammatory cytokines, and caused neutrophil and macrophage infiltration.
Specifically: red meat intake (any) decreased beneficial bacteria (Streptococcus, Akkermansia, Faecalibacterium, Lactococcus) and increased harmful ones (Clostridium, Mucispirillum).
There were some differences between the three red meats (beef, pork, lamb), but the differences pertained more to variations within:
- which beneficial bacteria were decreased the most
- which harmful bacteria were increased the most
You can see the exact results (including: per meat type and per bacterial strain) in the paper, here: Red Meat Diet Exacerbates Colitis by Promoting the Accumulation of Myeloid Cells and Disrupting Gut Microbiota
This dysbiosis (that is to say: disruption of the gut microbiome) then led to an overproduction of pro-inflammatory cytokines and infiltration of immune cells in the colon.
In other words, it inflamed the bowel—that is to say, promoted inflammatory bowel syndrome.
Want to learn more?
Check out:
Fruit, Fiber, & Leafy Greens… On A Low-FODMAP Diet!
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: