Chair Stretch Workout Guide
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝The 3 most important exercises don’t work if you can’t get on the floor. I’m 78, and have knee replacements. What about 3 best chair yoga stretches? Love your articles!❞
Here are six!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Parsley vs Spinach – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing parsley to spinach, we picked the parsley.
Why?
First of all, writer’s anecdote: today’s choice brought to you by a real decision here in my household! You see, a certain dish I sometimes prepare (it’s just a wrap-based dish, nothing fancy) requires a greenery component, and historically I’ve used kale or spinach. Of those two, I prefer kale while my son, who lives (and dines) with me, prefers spinach. However, we both like parsley equally, so I’m going to use that today. But I was curious about how it performed nutritionally, hence today’s comparison!
Ok, now for the stats…
In terms of macros, the only difference is that parsley has more fiber and carbs, for an approximately equal glycemic index, so we’ll go with the one with the highest total fiber, which is parsley.
In the category of vitamins, parsley has more of vitamins B3, B5, B7, B9, C, and K, while spinach has more of vitamins A, B2, B6, E, and choline. So, a marginal 6:5 win for parsley (and in the margins of difference are also in parsley’s favor, for example parsley has 13x the vitamin C, and 2x or 3x the other vitamins it won with, while spinach boasts 2x for some vitamins, and only 1.2x or 1.5x the others).
When it comes to minerals, parsley has more iron, phosphorus, potassium, and zinc, while spinach has more copper, magnesium, manganese, and selenium. So, a 4:4 tie on these.
In terms of phytochemicals, parsley has a much higher polyphenol content (that’s good) while spinach has a much higher oxalate content (that’s neutral for most people, but bad if you have certain kidney problems). So, another win for parsley.
Adding up the sections makes a clear overall win for parsley, but by all means enjoy either or both, unless you are avoiding oxalates, in which case, the oxalates in spinach can be reduced by cooking, but honestly, for most dishes you might as well just pick a different greens option (like parsley, or collard greens if you want something closer to the culinary experience of eating spinach).
Want to learn more?
You might like:
Invigorating Sabzi Khordan ← another great way to enjoy parsley as main ingredient rather than just a seasoning
Enjoy!
Share This Post
-

How Does One Test Acupuncture Against Placebo Anyway?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Pinpointing The Usefulness Of Acupuncture

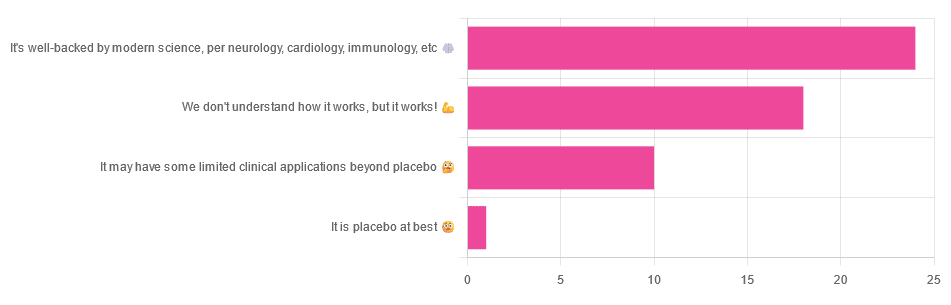
We asked you for your opinions on acupuncture, and got the above-depicted, below-described, set of answers:
- A little under half of all respondents voted for “It’s well-backed by modern science, per neurology, cardiology, immunology, etc”
- Slightly fewer respondents voted for “We don’t understand how it works, but it works!”
- A little under a fifth of respondents voted for “It may have some limited clinical applications beyond placebo”
- One (1) respondent voted for for “It’s placebo at best”
When we did a main feature about homeopathy, a couple of subscribers wrote to say that they were confused as to what homeopathy was, so this time, we’ll start with a quick definition first.
First, what is acupuncture? For the convenience of a quick definition so that we can move on to the science, let’s borrow from Wikipedia:
❝Acupuncture is a form of alternative medicine and a component of traditional Chinese medicine in which thin needles are inserted into the body.
Acupuncture is a pseudoscience; the theories and practices of TCM are not based on scientific knowledge, and it has been characterized as quackery.❞
Now, that’s not a promising start, but we will not be deterred! We will instead examine the science itself, rather than relying on tertiary sources like Wikipedia.
It’s worth noting before we move on, however, that there is vigorous debate behind the scenes of that article. The gist of the argument is:
- On one side: “Acupuncture is not pseudoscience/quackery! This has long been disproved and there are peer-reviewed research papers on the subject.”
- On the other: “Yes, but only in disreputable quack journals created specifically for that purpose”
The latter counterclaim is a) potentially a “no true Scotsman” rhetorical ploy b) potentially true regardless
Some counterclaims exhibit specific sinophobia, per “if the source is Chinese, don’t believe it”. That’s not helpful either.
Well, the waters sure are muddy. Where to begin? Let’s start with a relatively easy one:
It may have some clinical applications beyond placebo: True or False?
True! Admittedly, “may” is doing some of the heavy lifting here, but we’ll take what we can get to get us going.
One of the least controversial uses of acupuncture is to alleviate chronic pain. Dr. Vickers et al, in a study published under the auspices of JAMA (a very respectable journal, and based in the US, not China), found:
❝Acupuncture is effective for the treatment of chronic pain and is therefore a reasonable referral option. Significant differences between true and sham acupuncture indicate that acupuncture is more than a placebo.
However, these differences are relatively modest, suggesting that factors in addition to the specific effects of needling are important contributors to the therapeutic effects of acupuncture❞
Source: Acupuncture for Chronic Pain: Individual Patient Data Meta-analysis
If you’re feeling sharp today, you may be wondering how the differences are described as “significant” and “relatively modest” in the same text. That’s because these words have different meanings in academic literature:
- Significant = p<0.05, where p is the probability of the achieved results occurring randomly
- Modest = the differences between the test group and the control group were small
In other words, “significant modest differences” means “the sample sizes were large, and the test group reliably got slightly better results than placebo”
We don’t understand how it works, but it works: True or False
Broadly False. When it works, we generally have an idea how.
Placebo is, of course, the main explanation. And even in examples such as the above, how is placebo acupuncture given?
By inserting acupuncture needles off-target rather than in accord with established meridians and points (the lines and dots that, per Traditional Chinese Medicine, indicate the flow of qi, our body’s vital energy, and welling-points of such).
So, if a patient feels that needles are being inserted randomly, they may no longer have the same confidence that they aren’t in the control group receiving placebo, which could explain the “modest” difference, without there being anything “to” acupuncture beyond placebo. After all, placebo works less well if you believe you are only receiving placebo!
Indeed, a (Korean, for the record) group of researchers wrote about this—and how this confounding factor cuts both ways:
❝Given the current research evidence that sham acupuncture can exert not only the originally expected non-specific effects but also sham acupuncture-specific effects, it would be misleading to simply regard sham acupuncture as the same as placebo.
Therefore, researchers should be cautious when using the term sham acupuncture in clinical investigations.❞
Source: Sham Acupuncture Is Not Just a Placebo
It’s well-backed by modern science, per neurology, cardiology, immunology, etc: True or False?
False, for the most part.
While yes, the meridians and points of acupuncture charts broadly correspond to nerves and vasculature, there is no evidence that inserting needles into those points does anything for one’s qi, itself a concept that has not made it into Western science—as a unified concept, anyway…
Note that our bodies are indeed full of energy. Electrical energy in our nerves, chemical energy in every living cell, kinetic energy in all our moving parts. Even, to stretch the point a bit, gravitational potential energy based on our mass.
All of these things could broadly be described as qi, if we so wish. Indeed, the ki in the Japanese martial art of aikido is the latter kinds; kinetic energy and gravitational potential energy based on our mass. Same goes, therefore for the ki in kiatsu, a kind of Japanese massage, while the ki in reiki, a Japanese spiritual healing practice, is rather more mystical.
The qi in Chinese qigong is mostly about oxygen, thus indirectly chemical energy, and the electrical energy of the nerves that are receiving oxygenated blood at higher or lower levels.
On the other hand, the efficacy of the use of acupuncture for various kinds of pain is well-enough evidenced. Indeed, even the UK’s famously thrifty NHS (that certainly would not spend money on something it did not find to work) offers it as a complementary therapy for some kinds of pain:
❝Western medical acupuncture (dry needling) is the use of acupuncture following a medical diagnosis. It involves stimulating sensory nerves under the skin and in the muscles.
This results in the body producing natural substances, such as pain-relieving endorphins. It’s likely that these naturally released substances are responsible for the beneficial effects experienced with acupuncture.❞
Source: NHS | Acupuncture
Meanwhile, the NIH’s National Cancer Institute recommends it… But not as a cancer treatment.
Rather, they recommend it as a complementary therapy for pain management, and also against nausea, for which there is also evidence that it can help.
Frustratingly, while they mention that there is lots of evidence for this, they don’t actually link the studies they’re citing, or give enough information to find them. Instead, they say things like “seven randomized clinical trials found that…” and provide links that look reassuring until one finds, upon clicking on them, that it’s just a link to the definition of “randomized clinical trial”:
Source: NIH | Nactional Cancer Institute | Acupuncture (PDQ®)–Patient Version
However, doing our own searches finds many studies (mostly in specialized, potentially biased, journals such as the Journal of Acupuncture and Meridian Studies) finding significant modest outperformance of [what passes for] placebo.
Sometimes, the existence of papers with promising titles, and statements of how acupuncture might work for things other than relief of pain and nausea, hides the fact that the papers themselves do not, in fact, contain any evidence to support the hypothesis. Here’s an example:
❝The underlying mechanisms behind the benefits of acupuncture may be linked with the regulation of the hypothalamic-pituitary-gonadal (adrenal) axis and activation of the Wnt/β-catenin and OPG/RANKL/RANK signaling pathways.
In summary, strong evidence may still come from prospective and well-designed clinical trials to shed light on the potential role of acupuncture in preserving bone loss❞
Source: Acupuncture for Osteoporosis: a Review of Its Clinical and Preclinical Studies
So, here they offered a very sciencey hypothesis, and to support that hypothesis, “strong evidence may still come”.
“We must keep faith” is not usually considered evidence worthy of inclusion in a paper!
PS: the above link is just to the abstract, because the “Full Text” link offered in that abstract leads to a completely unrelated article about HIV/AIDS-related cryptococcosis, in a completely different journal, nothing to do with acupuncture or osteoporosis).
Again, this is not the kind of professionalism we expect from peer-reviewed academic journals.
Bottom line:
Acupuncture reliably performs slightly better than sham acupuncture for the management of pain, and may also help against nausea.
Beyond placebo and the stimulation of endorphin release, there is no consistently reliable evidence that is has any other discernible medical effect by any mechanism known to Western science—though there are plenty of hypotheses.
That said, absence of evidence is not evidence of absence, and the logistical difficulty of testing acupuncture against placebo makes for slow research. Maybe one day we’ll know more.
For now:
- If you find it helps you: great! Enjoy
- If you think it might help you: try it! By a licensed professional with a good reputation, please.
- If you are not inclined to having needles put in you unnecessarily: skip it! Extant science suggests that at worst, you’ll be missing out on slight relief of pain/nausea.
Take care!
Share This Post
-
5 Ways To Beat Afternoon Energy Slumps
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

This is Nisha Vora, of Rainbow Plant Life fame. After graduating from Harvard Law School, she realized she hated being a lawyer, and pivoted completely to become what she now is 12 years later, a chef and health coach.
Here are her tips for boosting energy through the day:
Caffeine timing
If you don’t do caffeine at all, no need to change that, but if you do, Vora advises that midday is the best time for it, with a very good rationale:
- of course it should not be too late in the day, because the elimination half-life of caffeine (4–8 hours to eliminate just half of the caffeine, depending on genes, call it 6 hours as an average though honestly for most people it will either be 4 or 8, not 6) is such that it can easily interfere with sleep for most people
- because caffeine is an adenosine blocker, not an adenosine inhibitor, taking caffeine in the morning means either there’s no adenosine to block, or it’ll just “save” that adenosine for later, i.e. when the caffeine is eliminated, then the adenosine will kick in, meaning that your morning sleepiness has now been deferred to the afternoon, rather than eliminated.
Another reminder that caffeine is the “payday loan” of energy. So, midday it is. No morning sleepiness to defer, and yet also not so late as to interfere with sleep.
See also: Calculate (And Enjoy) The Perfect Night’s Sleep
Simplify what can be simplified
This one’s not from a physiological basis, but rather, that a lot of the time most of us have much of our energy being taken by constant task-switching (what gets called multitasking, but as our brain is a single processor, it really means switching rapidly between different kinds of cognition, which is not efficient). In order to avoid that energy drain, try to streamline things and make a particular effort to not only single-task, but to do so without distractions.
Counterpoint: if you have unmedicated ADHD, then chances are you’ll do better with a single small distraction chosen by you, than trying to go without distractions, because your brain will find distractions anyway, so you might as well choose one (for many people it is background music, or a podcast or TV show that one doesn’t may attention to but it’s there) as a matter of harm reduction, and that way you’ll do better at focusing on your primary task than if your brain were reaching out for every and any possible distraction.
Manage your blood sugars
In particular, she advocates for avoiding sugary breakfasts, opting instead for protein, fat, and fiber-rich options. For more in this regard, see:
10 Ways To Balance Your Blood Sugars
Walk after meals
You don’t have to don hiking boots and “I am just going outside and may be some time“; rather, even a 2–5 minute walk after a meal helps regulate digestion and glucose levels, avoiding postprandial energy slumps.
So,
- if you have a treadmill, after eating is a great time to use it for a few minutes
- if you have stairs, now’s a great time to go up and down them a few times
One last technique for when everything else fails
We’ll quote her directly on this one:
❝Despite my best efforts, soemtimes I just have one of those days. Maybe I didn’t sleep well or I’m distracted by my never ending thoughts. If I need to be productive or energized on those days, I will do something that I absolutely hate:
I will take a cold shower.
And I hate it because I’m already always cold all the time, so why would I want to get a cold shower?
Well, it’s because cold water immersion has been shown to dramatically boost your dopamine levels, which gives you more energy and motivation.
In the moment though, it’s mostly painful and I hate everything and everyone around me.
But I know that if I can suffer through two minutes of a cold shower, I will feel so refreshed.❞
There are more benefits than just that, though, see:
A Cold Shower A Day Keeps The Doctor Away?
Want more from Nisha Vora?
We reviewed one of her books a while back:
The Vegan Instant Pot Cookbook – by Nisha Vora
Enjoy!
Share This Post



Related Posts
-

Are Brain Chips Safe?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Ready For Cyborgization?

In yesterday’s newsletter, we asked you for your views on Brain-Computer Interfaces (BCIs), such as the Utah Array and Neuralink’s chips on/in brains that allow direct communication between brains and computers, so that (for example) a paralysed person can use a device to communicate, or manipulate a prosthetic limb or two.
We didn’t get as many votes as usual; it’s possible that yesterday’s newsletter ended up in a lot of spam filters due to repeated use of a word in “extra ______ olive oil” in its main feature!
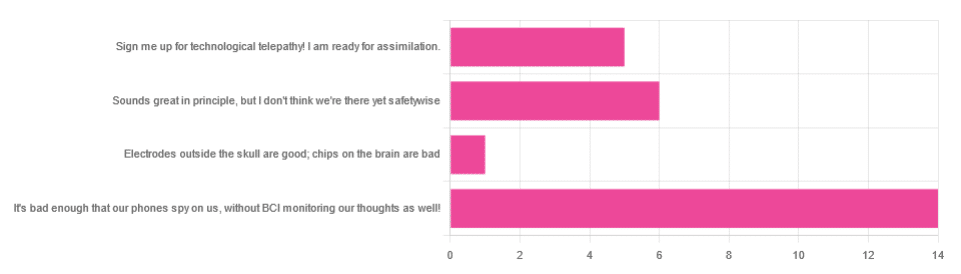
However, of the answers we did get…
- About 54% said “It’s bad enough that our phones spy on us, without BCI monitoring our thoughts as well!”
- About 23% said “Sounds great in principle, but I don’t think we’re there yet safetywise”
- About 19% said “Sign me up for technological telepathy! I am ready for assimilation”
- One (1) person said “Electrode outside the skull are good; chips on the brain are bad”
But what does the science say?
We’re not there yet safetywise: True or False?
True, in our opinion, when it comes to the latest implants, anyway. While it’s very difficult to prove a negative (it could be that everything goes perfectly in human trials), “extraordinary claims require extraordinary evidence”, and so far this seems to be lacking.
The stage before human trials is usually animal trials, starting with small creatures and working up to non-human primates if appropriate, before finally humans.
- Good news: the latest hot-topic BCI device (Neuralink) was tested on animals!
- Bad news: to say it did not go well would be an understatement
The Gruesome Story of How Neuralink’s Monkeys Actually Died
The above is a Wired article, and we tend to go for more objective sources, however we chose this one because it links to very many objective sources, including an open letter from the Physicians’ Committee for Responsible Medicine, which basically confirms everything in the Wired article. There are lots of links to primary (medical and legal) sources, too.
Electrodes outside the skull are good; chips on/in the brain are bad: True or False?
True or False depending on how they’re done. The Utah Array (an older BCI implant, now 20 years old, though it’s been updated many times since) has had a good safety record, after being used by a few dozen people with paralysis to control devices:
How the Utah Array is advancing BCI science
The Utah Array works on the same general principle as Neuralink, but the mechanics of its implementation are very different:
- The Utah Array involves a tiny bundle of microelectrodes (held together by a rigid structure that looks a bit like a nanoscale hairbrush) put in place by a brain surgeon, and that’s that.
- The Neuralink has a dynamic web of electrodes, implanted by a little robot that acts like a tiny sewing machine to implant many polymer threads, each containing its own a bunch of electrodes.
In theory, the latter is much more advanced. In practice, so far, the former has a much better safety record.
I am right to be a little worried about giving companies access to my brain: True or False?
True or False, depending on the nature of your concern.
For privacy: current BCI devices have quite simple switches operated consciously by the user. So while technically any such device that then runs its data through Bluetooth or WiFi could be hacked, this risk is no greater than using a wireless mouse and/or keyboard, because it has access to about the same amount of information.
For safety: yes, probably there is cause to be worried. Likely the first waves of commercial users of any given BCI device will be severely disabled people who are more likely to waive their rights in the hope of a life-changing assistance device, and likely some of those will suffer if things go wrong.
Which on the one hand, is their gamble to make. And on the other hand, makes rushing to human trials, for companies that do that, a little more predatory.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What is reformer pilates? And is it worth the cost?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Reformer pilates is steadily growing in popularity, with new studios opening regularly in major cities all over the world.
But what exactly is reformer pilates? And how does it compare with regular pilates and other types of exercise?
Classes aren’t cheap so let’s look at the potential benefits and drawbacks to help you decide if it’s right for you.

Ahmet Kurt/Unsplash Pilates with special equipment
Pilates is a mode of exercise that focuses on core stability and flexibility, while also addressing muscular strength and endurance, balance and general fitness. At first glance, it might look a bit like yoga, with some more traditional weight training components thrown in.
Reformer pilates uses a piece of equipment called a “reformer”. This looks like a narrow bed that slides along a carriage, has straps to hold onto, and has adjustable springs that add resistance to movement. You perform pilates on the reformer to target specific muscle groups and movement patterns.
The reformer was first designed to help people recover from injuries. However, it has now become common for general fitness and even sports performance.
Unlike normal pilates, also known as “mat pilates”, which only uses your body weight, the reformer adds resistance, meaning you can change the difficulty according to your current level of fitness.
This not only provides a way to overload your muscles, but can make the exercise session more aerobically demanding, which has been proposed to improve cardiovascular fitness.
Mat pilates uses your body weight. Kampus Productions/Pexels What are the benefits of reformer pilates?
Despite being around for decades, there is surprisingly little research looking at the benefits of reformer pilates. However, what we have seen so far suggests it has a similar effect to other modes of exercise.
Reformer pilates has been shown to help with weight loss, cause some small increases in muscle mass, and enhance cognitive function. All of these benefits are commonly seen when combining weight training and cardio into the same routine.
Similarly, among older adults, it has been shown to improve strength, enhance flexibility and may even reduce the risk of falling.
From a rehabilitation perspective, there is some evidence indicating reformer pilates can improve shoulder health and function, reduce lower back pain and increase flexibility.
Finally, there is some evidence suggesting a single session of reformer pilates can improve two key markers of cardiovascular health, being flow-mediated dilation and pulse wave velocity, while also improving cholesterol and insulin levels. This suggests reformer pilates could lead to long-term improvements in heart and metabolic health, although more research is needed to confirm this.
Reformer pilates was first designed to help people recover from injuries. Kampus Productions/Pexels However, there are some key things to consider when discussing these benefits. Most of this research is quite exploratory and comes from a very small number of studies. So we do not know whether these findings will apply to everyone.
Very few studies compared reformer pilates to other types of exercise. Therefore, while it can improve most aspects of health and function, it’s unlikely reformer pilates provides the optimal mode of exercise for each individual component of physical fitness.
Traditional weight training, for example, will likely cause larger improvements in strength than reformer pilates. Similarly, stretching will probably make you more flexible. And running or cycling will make you fitter.
However, if you want a type of exercise that gives you broad overall health benefits, it could be a good option.
What are the downsides of reformer pilates
Reformer pilates is not for everyone.
First and foremost, classes can be expensive compared to other fitness options. You need to be doing at least two to three sessions per week of any type of exercise to maximise the benefits. So even if you can find a class for A$20 or $30, paying for two or three classes a week (or buying a weekly or monthly subscription) is a significant outlay.
Second, it’s not as accessible as other exercise. Even if you can afford it, not every town or suburb has a reformer pilates studio.
Cost and access are major barriers. Or you might get better results with specific modes of exercises. Karolina Grabowska/Pexels Third, the effectiveness of your workout is likely to be impacted by how competent your instructor is. There are a host of different pilates qualifications you can get in Australia, and some take much less time than others. With this in mind, it might be best to look for accredited pilates instructors, although this will further reduce the number of options you have available.
Finally, there is a learning curve. While you will get better over time, the exercise will likely be less effective during those first few weeks (or months) when you are getting used to the machine and the movements.
Is it right for you?
Reformer pilates can be a great addition to your fitness routine, especially if you’re looking for a low-impact way to build strength and flexibility.
But if you have more specific goals, you might need a more specific mode of exercise. For example, if you need to get stronger to improve your ability to manage your daily life, then strength training is probably your best bet. Likewise, if your goal is to run a marathon, you will get more specific benefits from running.
The cost and availability of reformer pilates make it less accessible for some people. With this in mind, if you are after similar benefits at a lower price point, mat pilates might be a better option. Not only does it have evidence suggesting it can improve strength and fitness, but it is something you can do at home if you find a good resource (YouTube could be a good starting point here).
Hunter Bennett, Lecturer in Exercise Science, University of South Australia; Jacinta Brinsley, Exercise Physiologist and Postdoctoral Researcher in the Alliance for Research in Nutrition, Exercise and Activity, University of South Australia, and Lewis Ingram, Lecturer in Physiotherapy, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What are nootropics and do they really boost your brain?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Humans have long been searching for a “magic elixir” to make us smarter, and improve our focus and memory. This includes traditional Chinese medicine used thousands of years ago to improve cognitive function.
Now we have nootropics, also known as smart drugs, brain boosters or cognitive enhancers.
You can buy these gummies, chewing gums, pills and skin patches online, or from supermarkets, pharmacies or petrol stations. You don’t need a prescription or to consult a health professional.
But do nootropics actually boost your brain? Here’s what the science says.
LuckyStep/Shutterstock What are nootropics and how do they work?
Romanian psychologist and chemist Cornelius E. Giurgea coined the term nootropics in the early 1970s to describe compounds that may boost memory and learning. The term comes from the Greek words nӧos (thinking) and tropein (guide).
Nootropics may work in the brain by improving transmission of signals between nerve cells, maintaining the health of nerve cells, and helping in energy production. Some nootropics have antioxidant properties and may reduce damage to nerve cells in the brain caused by the accumulation of free radicals.
But how safe and effective are they? Let’s look at four of the most widely used nootropics.
1. Caffeine
You might be surprised to know caffeine is a nootropic. No wonder so many of us start our day with a coffee. It stimulates our nervous system.
Caffeine is rapidly absorbed into the blood and distributed in nearly all human tissues. This includes the brain where it increases our alertness, reaction time and mood, and we feel as if we have more energy.
For caffeine to have these effects, you need to consume 32-300 milligrams in a single dose. That’s equivalent to around two espressos (for the 300mg dose). So, why the wide range? Genetic variations in a particular gene (the CYP1A2 gene) can affect how fast you metabolise caffeine. So this can explain why some people need more caffeine than others to recognise any neurostimulant effect.
Unfortunately too much caffeine can lead to anxiety-like symptoms and panic attacks, sleep disturbances, hallucinations, gut disturbances and heart problems.
So it’s recommended adults drink no more than 400mg caffeine a day, the equivalent of up to three espressos.
Caffeine can make you feel alert and can boost your mood. That makes it a nootropic. LHshooter/Shutterstock 2. L-theanine
L-theanine comes as a supplement, chewing gum or in a beverage. It’s also the most common amino acid in green tea.
Consuming L-theanine as a supplement may increase production of alpha waves in the brain. These are associated with increased alertness and perception of calmness.
However, it’s effect on cognitive functioning is still unclear. Various studies including those comparing a single dose with a daily dose for several weeks, and in different populations, show different outcomes.
But taking L-theanine with caffeine as a supplement improved cognitive performance and alertness in one study. Young adults who consumed L-theanine (97mg) plus caffeine (40mg) could more accurately switch between tasks after a single dose, and said they were more alert.
Another study of people who took L-theanine with caffeine at similar doses to the study above found improvements in several cognitive outcomes, including being less susceptible to distraction.
Although pure L-theanine is well tolerated, there are still relatively few human trials to show it works or is safe over a prolonged period of time. Larger and longer studies examining the optimal dose are also needed.
The amino acid L-theanine is also in green tea. grafvision/Shutterstock 3. Ashwaghanda
Ashwaghanda is a plant extract commonly used in Indian Ayurvedic medicine for improving memory and cognitive function.
In one study, 225-400mg daily for 30 days improved cognitive performance in healthy males. There were significant improvements in cognitive flexibility (the ability to switch tasks), visual memory (recalling an image), reaction time (response to a stimulus) and executive functioning (recognising rules and categories, and managing rapid decision making).
There are similar effects in older adults with mild cognitive impairment.
But we should be cautious about results from studies using Ashwaghanda supplements; the studies are relatively small and only treated participants for a short time.
Ashwaghanda is a plant extract commonly used in Ayurvedic medicine. Agnieszka Kwiecień, Nova/Wikimedia, CC BY-SA 4. Creatine
Creatine is an organic compound involved in how the body generates energy and is used as a sports supplement. But it also has cognitive effects.
In a review of available evidence, healthy adults aged 66-76 who took creatine supplements had improved short-term memory.
Long-term supplementation may also have benefits. In another study, people with fatigue after COVID took 4g a day of creatine for six months and reported they were better able to concentrate, and were less fatigued. Creatine may reduce brain inflammation and oxidative stress, to improve cognitive performance and reduce fatigue.
Side effects of creatine supplements in studies are rarely reported. But they include weight gain, gastrointestinal upset and changes in the liver and kidneys.
Where to now?
There is good evidence for brain boosting effects of caffeine and creatine. But the jury is still out on the efficacy, optimal dose and safety of most other nootropics.
So until we have more evidence, consult your health professional before taking a nootropic.
But drinking your daily coffee isn’t likely to do much harm. Thank goodness, because for some of us, it is a magic elixir.
Nenad Naumovski, Professor in Food Science and Human Nutrition, University of Canberra; Amanda Bulman, PhD candidate studying the effects of nutrients on sleep, University of Canberra, and Andrew McKune, Professor, Exercise Science, University of Canberra
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: