Cantaloupe vs Cucumber – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cantaloupe to cucumber, we picked the cucumber.
Why?
In terms of macros, both are of course 90–95% water, with just enough fiber to hold them together. However, it’s cantaloupe that’s 90% water and cucumber that’s 95% water, because cantaloupe has more than 2x the carbs and 144x the sugar (whence the sweetness). Now, it’s a fruit and so this sugar isn’t really anything to worry about if you’re eating it in solid form (as opposed to as juice), but by the numbers, it does mean that cucumber has the much lower glycemic index (cucumber has a GI of 21, while cantaloupe has a GI of 65), so we’ll give cucumber the win in this category.
In the category of vitamins, cantaloupe has more of vitamins A, B3, B6, B9, C, and E, while cucumber has more of vitamins B2, B5, and K, so cantaloupe scores a 6:3 win in this round.
When it comes to minerals, cantaloupe has more potassium and selenium, while cucumber has more calcium, iron, magnesium, manganese, phosphorus, and zinc, so another win for cucumber here.
Looking at polyphenols, cantaloupe has almost nothing (trace amounts of some lignans), while cucumber has more of the same lignans that cantaloupe has, plus highly beneficial flavones apigenin and luteolin, and famously good flavonols like kaempferol and quercetin. So, one more win for cucumber here.
Plus, and it’s not yet known the mechanism of action for this one, but cucumber extract beats glucosamine and chondroitin for reducing joint inflammation, at 1/135th of the dose.
Adding up the sections makes for a very clear overall win for cucumber, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Lupus Sex Differences Are Not What You Might Think

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

This is Dr. Seyhan Yazar, a medical scientist and Research Fellow, whose lab (the Yazar Lab) “focuses on uncovering the complex interplay between genetic susceptibility and environmental triggers in autoimmune diseases”, of which, lupus is one.
So, what does she want us to know?
Sex? It’s not about the X
First, a recap on how lupus works: lupus is an autoimmune disease where the immune system attacks its own tissues, causing inflammation and organ damage (to oversimplify it in very few words).
Next, how lupus is currently treated: mostly with immunosuppressant drugs, which reduce symptoms but have significant side effects, not least of all the fact that your immune system will be suppressed, leaving you vulnerable to infections, cancer, aging, and the like. So, there’s really a “damned if you do, damned if you don’t” aspect here (because untreated lupus will run your immune system into the ground with its chronic inflammation, which will also leave you vulnerable to the aforementioned things).
See also: How to Prevent (or Reduce) Inflammation
Finally, onto the new science from Dr. Yazar: while it’s well-known that lupus disproportionately affects women (with women’s lupus risk being 9x that of men’s, all other things being equal), it hasn’t been known entirely what’s going on with that and how, but Dr. Yazar’s work shines new light on this!
She and her team analyzed over a million (for the curious: 1,267,758) individual immune cells from 982 healthy people, to identify sex-specific genetic switches that shape male and female immune systems differently.
In the immune cell analysis, women had higher levels of B cells and regulatory T cells, with immune activity more strongly biased towards inflammatory pathways, creating a more vigilant immune system that will often better fight infections, but at a cost: it also raises the risk of “friendly fire” against healthy tissues, and that’s what happens in the case of lupus.
On the flipside, men had more monocytes and immune activity focused more on cellular maintenance rather than inflammation, which will tend to reduce autoimmune risk but at its own cost: it raises the risk (and severity) of infections and some cancers.
Notably, these results showed that the sex-specific immune differences aren’t driven by X or Y chromosomes as often assumed, but instead by autosomes—the non-sex chromosomes shared by all sexes.
This is very consistent with what we know of many sex-related disease risk factors being hormonally mediated, rather than mediated by genes.
You can read Dr. Yazar’s paper on all of this, here: The impact of sex on the immune system explored at the single-cell level
As for what can be done about this, the same principle applies as we talked about in Alzheimer’s Sex Differences May Not Be What They Appear but the opposite way around, meaning the solution may be the same as what we talked about in The Hormone Therapy That Reduces Breast Cancer Risk & More.
But! That last part is not yet proven, and is rather more simply a promising avenue for the next leg of the research, so please don’t take that as medical advice.
Want to learn more?
For a much more in-depth treatment of lupus management, you might like this excellent book we reviewed a while back:
The “et al.” in question? Jemima Albayda, MD; Divya Angra, MD; Alan N. Baer, MD; Sasha Bernatsky, MD, PhD; George Bertsias, MD, PhD; Ashira D. Blazer, MD; Ian Bruce, MD; Jill Buyon, MD; Yashaar Chaichian, MD; Maria Chou, MD; Sharon Christie, Esq; Angelique N. Collamer, MD; Ashté Collins, MD; Caitlin O. Cruz, MD; Mark M. Cruz, MD; Dana DiRenzo, MD; Jess D. Edison, MD; Titilola Falasinnu, PhD; Andrea Fava, MD; Cheri Frey, MD; Neda F. Gould, PhD; Nishant Gupta, MD; Sarthak Gupta, MD; Sarfaraz Hasni, MD; David Hunt, MD; Mariana J. Kaplan, MD; Alfred Kim, MD; Deborah Lyu Kim, DO; Rukmini Konatalapalli, MD; Fotios Koumpouras, MD; Vasileios C. Kyttaris, MD; Jerik Leung, MPH; Hector A. Medina, MD; Timothy Niewold, MD; Julie Nusbaum, MD; Ginette Okoye, MD; Sarah L. Patterson, MD; Ziv Paz, MD; Darryn Potosky, MD; Rachel C. Robbins, MD; Neha S. Shah, MD; Matthew A. Sherman, MD; Yevgeniy Sheyn, MD; Julia F. Simard, ScD; Jonathan Solomon, MD; Rodger Stitt, MD; George Stojan, MD; Sangeeta Sule, MD; Barbara Taylor, CPPM, CRHC; George Tsokos, MD; Ian Ward, MD; Emma Weeding, MD; Arthur Weinstein, MD; Sean A. Whelton, MD
The reason we mention this is to render it clear that this isn’t one man’s opinions (as happens with many books about certain topics), but rather, a panel of that many doctors all agreeing that this is correct and good, evidence-based, up-to-date (as of the publication of this latest revised edition all so recently) information.
Want to learn less?
If the aforementioned 848-page opus seems a little too overwhelming, then you might prefer:
The Lupus Solution – by Dr. Tiffany Caplan & Dr. Brent Caplan ← a much slimmer tome; just 182 pages 🙂
Take care!
Share This Post
-

The Brain’s Way of Healing – by Dr. Norman Doidge
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what this book isn’t: any sort of wishy-washy “think yourself better” fluff, and nor is it a “tapping into your Universal Divine Essence” thing.
In contrast, Dr. Norman Doidge sticks with science, and the only “vibrational frequencies” involved are the sort that come from an MRI machine or similar.
The author makes bold claims of the potential for leveraging neuroplasticity to heal many chronic diseases. All of them are neurological in whole or in part, ranging from chronic pain to Parkinson’s.
How well are these claims backed up, you ask?
The book makes heavy use of case studies. In science, case studies rarely prove anything, so much as indicate a potential proof of principle. Clinical trials are what’s needed to become more certain, and for Dr. Doidge’s claims, these are so far sadly lacking, or as yet inconclusive.
Where the book’s strengths lie is in describing exactly what is done, and how, to effect each recovery. Specific exercises to do, and explanations of the mechanism of action. To that end, it makes them very repeatable for any would-be “citizen scientist” who wishes to try (in the cases that they don’t require special equipment).
Bottom line: this book would be more reassuring if its putative techniques had enjoyed more clinical studies… But in the meantime, it’s a fair collection of promising therapeutic approaches for a number of neurological disorders.
Click here to check out The Brain’s Way of Healing, and learn more!
Share This Post
-

The Lupus Encyclopedia – by Dr. Donald Thomas
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, a note on the authorship: while this is broadly by Donald E. Thomas Jr. MD FACP FACR, there were more contributors, namely:
Jemima Albayda, MD; Divya Angra, MD; Alan N. Baer, MD; Sasha Bernatsky, MD, PhD; George Bertsias, MD, PhD; Ashira D. Blazer, MD; Ian Bruce, MD; Jill Buyon, MD; Yashaar Chaichian, MD; Maria Chou, MD; Sharon Christie, Esq; Angelique N. Collamer, MD; Ashté Collins, MD; Caitlin O. Cruz, MD; Mark M. Cruz, MD; Dana DiRenzo, MD; Jess D. Edison, MD; Titilola Falasinnu, PhD; Andrea Fava, MD; Cheri Frey, MD; Neda F. Gould, PhD; Nishant Gupta, MD; Sarthak Gupta, MD; Sarfaraz Hasni, MD; David Hunt, MD; Mariana J. Kaplan, MD; Alfred Kim, MD; Deborah Lyu Kim, DO; Rukmini Konatalapalli, MD; Fotios Koumpouras, MD; Vasileios C. Kyttaris, MD; Jerik Leung, MPH; Hector A. Medina, MD; Timothy Niewold, MD; Julie Nusbaum, MD; Ginette Okoye, MD; Sarah L. Patterson, MD; Ziv Paz, MD; Darryn Potosky, MD; Rachel C. Robbins, MD; Neha S. Shah, MD; Matthew A. Sherman, MD; Yevgeniy Sheyn, MD; Julia F. Simard, ScD; Jonathan Solomon, MD; Rodger Stitt, MD; George Stojan, MD; Sangeeta Sule, MD; Barbara Taylor, CPPM, CRHC; George Tsokos, MD; Ian Ward, MD; Emma Weeding, MD; Arthur Weinstein, MD; Sean A. Whelton, MD
The reason we mention this is to render it clear that this isn’t one man’s opinions (as happens with many books about certain topics), but rather, a panel of that many doctors all agreeing that this is correct and good, evidence-based, up-to-date (as of the publication of this latest revised edition last year) information.
And if you have lupus, you’ll be aware there are a lot of doctors who don’t know a tremendous amount about it, hence the value of this “…for patients and healthcare providers” tome.
It is what it claims to be: a very comprehensive guide. It’s not light reading, and it is 848 pages of information-dense text and diagrams. If you want to know something, anything, about lupus, then if science knows it, then chances are it is in this book, or this book will at least point you directly to a paper you can read about your specific query.
The style is, nevertheless, about as readable for the layperson as possible, which is quite an achievement for a book with this amount of dense scientific information. For that, the author thanks his husband, for being the non-doctor beta-reader to screen it for readability—quite a service, with all those doctors writing!
Bottom line: if you or someone you love has lupus, this book should absolutely be in your collection.
Click here to check out The Lupus Encyclopedia, and have everything at your fingertips!
Share This Post


Related Posts
-
Is thunderstorm asthma becoming more common?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When spring arrives, so do warnings about thunderstorm asthma. But a decade ago, most of us hadn’t heard of it.
So where did thunderstorm asthma come from? Is it a new phenomenon?
In 2016, the world’s most catastrophic thunderstorm asthma event took Melbourne by surprise. An increase in warnings and monitoring is partly a response to this.
But there are also signs climate change may be exacerbating the likelihood of thunderstorm asthma, with more extreme weather, extended pollen seasons and a rise in Australians reporting hay fever.
A landmark catastrophe
The first time many Australians heard of thunderstorm asthma was in November 2016, when a major event rocked Melbourne.
During a late night storm, an estimated 10,000 people were rushed to hospitals with severe asthma attacks. With thousands of calls on emergency lines, ambulances and emergency departments were unprepared to handle the rapid increase in people needing urgent medical care. Tragically, ten of those people died.
This was the most catastrophic thunderstorm asthma event in recorded history and the first time deaths have ever occurred anywhere in the world.
In response, the Victorian Department of Health implemented initiatives, including public awareness campaigns and improvements to health and emergency services, to be ready for future thunderstorm asthma events.
A network of pollen monitoring stations was also set up across the state to gather data that helps to predict future events.
A problem for decades
While this event was unexpected, it wasn’t the first time we’d had thunderstorm asthma in Australia – we’ve actually known about it for decades.
Melbourne reported its first instance of thunderstorm asthma back in 1984, only a year after this phenomenon was first discovered in Birmingham in the United Kingdom.
Thunderstorm asthma has since been reported in other parts of Australia, including Canberra and New South Wales. But it is still most common in Melbourne. Compared to any other city (or country) the gap is significant: over a quarter of all known events worldwide have occurred in Melbourne.
Why Melbourne?
Melbourne’s location makes it a hotspot for these kinds of events. Winds coming from the north of Melbourne tend to be dry and hot as they come from deserts in the centre of Australia, while winds from the south are cooler as they come from the ocean.
When hot and cool air mix above Melbourne, it creates the perfect conditions for thunderstorms to form.
Northern winds also blow a lot of pollen from farmlands into the city, in particular grass pollen. This is not only the most common cause of seasonal hay fever in Melbourne but also a major trigger of thunderstorm asthma.
Why grass pollen?
There’s a particular reason grass pollen is the main culprit behind thunderstorm asthma in Australia. During storms there is a lot of moisture in the air. Grass pollen will absorb this moisture, making it swell up like a water balloon.
If pollen absorbs too much water whilst airborne, it can burst or “rupture,” releasing hundreds of microscopic particles into the air that can be swept by powerful winds.
Normally, when you breathe in pollen it gets stuck in your upper airway – for example, your nose and throat. This is what causes typical hay fever symptoms such as sneezing or runny nose.
But the microscopic particles released from ruptured grass pollen are much smaller and don’t get stuck as easily in the upper airway. Instead, they can travel deep into your airways until they reach your lungs. This may trigger more severe symptoms, such as wheezing or difficulty breathing, even in people with no prior history of asthma.
So who is at risk?
You might think asthma is the biggest risk factor for thunderstorm asthma. In fact, the biggest risk factor is hay fever.
Up to 99% of patients who went to the emergency department during the Melbourne 2016 event had hay fever, while a majority (60%) had no prior diagnosis of asthma.
Every single person hospitalised was allergic to at least one type of grass pollen. All had a sensitivity to ryegrass.
Is thunderstorm asthma becoming more common?
Thunderstorm asthma events are rare, with just 26 events officially recorded worldwide.
However there is evidence these events could become more frequent and severe in coming years, due to climate change. Higher temperatures and pollution could be making plants produce more pollen and pollen seasons last much longer.
Extreme weather events, including thunderstorms, are also expected to become more common and severe.
In addition, there are signs rates that hay fever may be increasing. The number of Australians reporting allergy symptoms have risen from 15% in 2008 to 24% in 2022. Similar trends in other countries has been linked to climate change.
How can I prepare?
Here are three ways you can reduce your risk of thunderstorm asthma:
- stock up on allergy medication and set up an asthma action plan with your GP
- check daily pollen forecasts for the estimated pollen level and risk of a thunderstorm asthma event in your local area
- on days with high pollen or a high risk of thunderstorm asthma, spend less time outside or wear a surgical face mask to reduce your symptoms.
Kira Morgan Hughes, PhD Candidate in Allergy and Asthma, School of Life and Environmental Sciences, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Is it OK if my child eats lots of fruit but no vegetables?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Does it seem like most vegetables you serve your children end up left on the plate, or worse, strewn across the floor? But mention dessert, and your fruit skewers are polished off in an instant.
Or maybe the carrot and cucumber sticks keep coming home in your child’s lunchbox untouched, yet the orange slices are nowhere to be seen.
If you’re facing these struggles with your child, you’re not alone. Many children prefer fruit to vegetables.
So if your child eats lots of fruit but minimal or no vegetables, is that OK? And how can you get them to eat more veggies?
Children have an innate preference for fruit
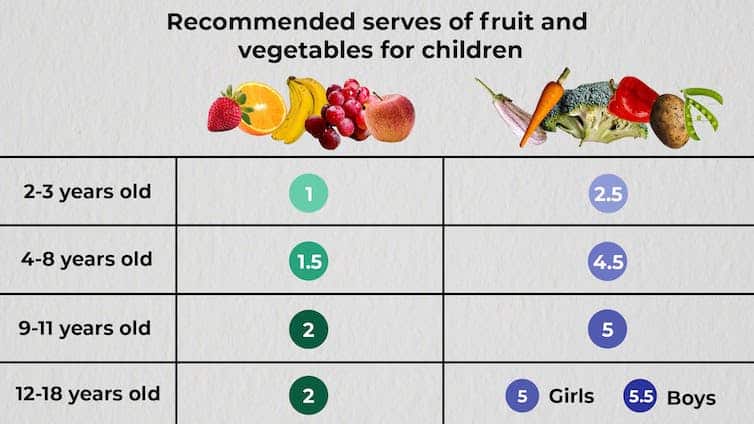
The Australian Dietary Guidelines’ recommended daily intakes for vegetables and fruit depend on a child’s age.

Fruit and vegetable serving sizes by age. The Conversation.
National Health and Medical Research Council, CC BY-SAConsumption among Australian children falls well below recommendations. Around 62.6% of children aged over two meet the recommended daily fruit intake, but only 9% meet the recommended vegetable intake.
This is not surprising given children have a natural preference for fruit. At least in part, this is due to its sweetness and texture, whether crispy, crunchy or juicy. The texture of fruit has been linked to a positive sensory experience among children.
Vegetables, on the other hand, are more of an acquired taste, and certain types, such as cruciferous vegetables, can be perceived by children as bitter.
The reason children often prefer fruit over vegetables could also be related to the parents’ preferences. Some research has even suggested we develop food preferences before birth based on what our mother consumes during pregnancy.
Balance is key
So, a preference for fruit is common. But is it OK if your child eats lots of fruit but little to no vegetables? This is a question we, as dietitians, get asked regularly.
You might be thinking, at least my child is eating fruit. They could be eating no veggies and no fruit. This is true. But while it’s great your child loves fruit, vegetables are just as important as part of a balanced eating pattern.
Vegetables provide us with energy, essential vitamins and minerals, as well as water and fibre, which help keep our bowels regular. They also support a strong immune system.
If your child is only eating fruit, they are missing some essential nutrients. But the same is true if they are eating only veggies.
Fruit likewise provides the body with a variety of essential vitamins and minerals, as well as phytochemicals, which can help reduce inflammation.
Evidence shows healthy consumption of fruit and vegetables protects against chronic diseases including high blood pressure, heart disease and stroke.
Consumed together, fruit and vegetables in a variety of colours provide different nutrients we need, some of which we can’t get from other foods. We should encourage kids to eat a “rainbow” of fruit and vegetables each day to support their growth and development.
What if my child eats too much fruit?
If your child is eating slightly more fruit than what’s recommended each day, it’s not usually a problem.
Fruit contains natural sugar which is good for you. But too much of a good thing, even if it’s natural, can create problems. Fruit also contains virtually no fat and very little to no protein, both essential for a growing child.
When overindulging in fruit starts to displace other food groups such as vegetables, dairy products and meat, that’s when things can get tricky.
6 tips to get your kids to love vegetables
1. Get them involved
Take your child with you when you go shopping. Let them choose new vegetables. See if you can find vegetables even you haven’t tried, so you’re both having a new experience. Then ask them to help you with preparing or cooking the vegetables using a recipe you have chosen together. This will expose your child to veggies in a positive way and encourage them to eat more.
2. Sensory learning
Try to expose your child to vegetables rather than hiding them. Kids are more likely to eat veggies when they see, smell and feel them. This is called sensory learning.
3. Have fun with food
Use colourful vegetables of different sizes and textures. Make them fun by creating scenes or faces on your child’s plate. Add edible flowers or mint for decoration. You can even serve this with a side of veggie-based dip such as hummus or guacamole for some bonus healthy fats.
4. Teach them to grow their own
Teach your child how to grow their own vegetables. Evidence shows kids are more inclined to try the food they have helped and watched grow. You don’t need to have a big backyard to do this. A windowsill with a pot plant is a perfect start.
5. Lead by example
Your child learns from you, and your eating habits will influence theirs. Ensure they see you eating and enjoying veggies, whether in meals or as snacks.
6. Practise persistence
If your child refuses a particular vegetable once, don’t give up. It can take many attempts to encourage children to try a new food.

Yasmine Probst, Associate Professor, School of Medical, Indigenous and Health Sciences, University of Wollongong; Olivia Wills, Accredited Practising Dietitian, PhD candidate, University of Wollongong, and Shoroog Allogmanny, Accredited Practising Dietitian, PhD candidate, University of Wollongong
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Visceral Fat: Why It Matters & How To Improve It
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Ruth Machin demystifies it:
At the core of things
Visceral fat is fat stored deep inside your abdominal cavity, underneath your abdominal wall muscles, surrounding your organs. As such, it’s different from subcutaneous fat (under your skin, the fat you can squish from the outside), and belongs to the broader category of ectopic fat (ectopic = “out of place”).
While it’s fine for your organs to have a little padding, the problem with excess visceral fat is that it secretes pro-inflammatory adipokines that drive insulin resistance, raise the risk of type 2 diabetes, promote hypertension, contribute to heart disease, and generally bring about (or exacerbate) metabolic syndrome in general.
Although overall weight gain in midlife comes mostly from age and reduced activity, not menopause itself, menopause is a factor—because declining estrogen levels result in the body shifting fat storage from hips and thighs, towards your midsection, increasing visceral fat.
How to measure visceral fat: it cannot be seen externally; waist-to-height ratio is a better guide than BMI; thresholds above 0.5 signal increased risk; imaging such as MRI is required for accurate measurement in research.
Still, if you have a smart scale, it’ll do a decent estimate for you as part of its body composition test, based on conductivity. Just remember, it’s not accurate, so in that case, worry less about the actual numbers, and more about the trends (e.g. whether the visceral fat score is going up or down over time or remaining the same).
Some notes from Dr. Machin on dietary considerations:
- Diet quality for reducing visceral fat: research shows that a mild (!) calorie deficit combined with avoiding saturated fats but enjoying low-GI carbohydrates (i.e: get plenty of fiber with your carbs) reduces visceral fat.
- Whole-food approaches that work: both low-carb and higher carb diets with unprocessed foods reduce visceral fat; avoiding added sugars and refined carbohydrates improves insulin resistance and abdominal fat patterns. No surprises here.
- Why the Mediterranean diet is effective: it promotes whole grains, beans, legumes, olive oil, fish, fruit, vegetables, and nuts; it supports cardiovascular health and reduces visceral fat more effectively than low-fat or low-carb diets in the long term.
- Extra benefits from polyphenols: the green Mediterranean diet, enriched with walnuts, green tea, and other polyphenol-dense foods, produced larger visceral fat reductions than the standard Mediterranean diet in clinical trials.
- Foods rich in polyphenols to include: dark berries, green and black tea, nuts with skins (e.g. almonds!), extra virgin olive oil, cocoa, ground flaxseed, red onions, dark green vegetables, and soy; these all improve waist circumference and metabolic markers.
- Overall eating guidance: enjoy unprocessed whole foods, keep added sugars low, avoid sugary drinks especially, replace refined carbohydrates with whole grains, and aim for a diet you can maintain for decades rather than weeks.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Visceral Belly Fat & How To Lose It
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: