Lupus Sex Differences Are Not What You Might Think
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

This is Dr. Seyhan Yazar, a medical scientist and Research Fellow, whose lab (the Yazar Lab) “focuses on uncovering the complex interplay between genetic susceptibility and environmental triggers in autoimmune diseases”, of which, lupus is one.
So, what does she want us to know?
Sex? It’s not about the X
First, a recap on how lupus works: lupus is an autoimmune disease where the immune system attacks its own tissues, causing inflammation and organ damage (to oversimplify it in very few words).
Next, how lupus is currently treated: mostly with immunosuppressant drugs, which reduce symptoms but have significant side effects, not least of all the fact that your immune system will be suppressed, leaving you vulnerable to infections, cancer, aging, and the like. So, there’s really a “damned if you do, damned if you don’t” aspect here (because untreated lupus will run your immune system into the ground with its chronic inflammation, which will also leave you vulnerable to the aforementioned things).
See also: How to Prevent (or Reduce) Inflammation
Finally, onto the new science from Dr. Yazar: while it’s well-known that lupus disproportionately affects women (with women’s lupus risk being 9x that of men’s, all other things being equal), it hasn’t been known entirely what’s going on with that and how, but Dr. Yazar’s work shines new light on this!
She and her team analyzed over a million (for the curious: 1,267,758) individual immune cells from 982 healthy people, to identify sex-specific genetic switches that shape male and female immune systems differently.
In the immune cell analysis, women had higher levels of B cells and regulatory T cells, with immune activity more strongly biased towards inflammatory pathways, creating a more vigilant immune system that will often better fight infections, but at a cost: it also raises the risk of “friendly fire” against healthy tissues, and that’s what happens in the case of lupus.
On the flipside, men had more monocytes and immune activity focused more on cellular maintenance rather than inflammation, which will tend to reduce autoimmune risk but at its own cost: it raises the risk (and severity) of infections and some cancers.
Notably, these results showed that the sex-specific immune differences aren’t driven by X or Y chromosomes as often assumed, but instead by autosomes—the non-sex chromosomes shared by all sexes.
This is very consistent with what we know of many sex-related disease risk factors being hormonally mediated, rather than mediated by genes.
You can read Dr. Yazar’s paper on all of this, here: The impact of sex on the immune system explored at the single-cell level
As for what can be done about this, the same principle applies as we talked about in Alzheimer’s Sex Differences May Not Be What They Appear but the opposite way around, meaning the solution may be the same as what we talked about in The Hormone Therapy That Reduces Breast Cancer Risk & More.
But! That last part is not yet proven, and is rather more simply a promising avenue for the next leg of the research, so please don’t take that as medical advice.
Want to learn more?
For a much more in-depth treatment of lupus management, you might like this excellent book we reviewed a while back:
The “et al.” in question? Jemima Albayda, MD; Divya Angra, MD; Alan N. Baer, MD; Sasha Bernatsky, MD, PhD; George Bertsias, MD, PhD; Ashira D. Blazer, MD; Ian Bruce, MD; Jill Buyon, MD; Yashaar Chaichian, MD; Maria Chou, MD; Sharon Christie, Esq; Angelique N. Collamer, MD; Ashté Collins, MD; Caitlin O. Cruz, MD; Mark M. Cruz, MD; Dana DiRenzo, MD; Jess D. Edison, MD; Titilola Falasinnu, PhD; Andrea Fava, MD; Cheri Frey, MD; Neda F. Gould, PhD; Nishant Gupta, MD; Sarthak Gupta, MD; Sarfaraz Hasni, MD; David Hunt, MD; Mariana J. Kaplan, MD; Alfred Kim, MD; Deborah Lyu Kim, DO; Rukmini Konatalapalli, MD; Fotios Koumpouras, MD; Vasileios C. Kyttaris, MD; Jerik Leung, MPH; Hector A. Medina, MD; Timothy Niewold, MD; Julie Nusbaum, MD; Ginette Okoye, MD; Sarah L. Patterson, MD; Ziv Paz, MD; Darryn Potosky, MD; Rachel C. Robbins, MD; Neha S. Shah, MD; Matthew A. Sherman, MD; Yevgeniy Sheyn, MD; Julia F. Simard, ScD; Jonathan Solomon, MD; Rodger Stitt, MD; George Stojan, MD; Sangeeta Sule, MD; Barbara Taylor, CPPM, CRHC; George Tsokos, MD; Ian Ward, MD; Emma Weeding, MD; Arthur Weinstein, MD; Sean A. Whelton, MD
The reason we mention this is to render it clear that this isn’t one man’s opinions (as happens with many books about certain topics), but rather, a panel of that many doctors all agreeing that this is correct and good, evidence-based, up-to-date (as of the publication of this latest revised edition all so recently) information.
Want to learn less?
If the aforementioned 848-page opus seems a little too overwhelming, then you might prefer:
The Lupus Solution – by Dr. Tiffany Caplan & Dr. Brent Caplan ← a much slimmer tome; just 182 pages 🙂
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Bell Pepper vs Okra – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing bell pepper to okra, we picked the okra.
Why?
It wasn’t a close one, today!
In terms of macros, okra has nearly 2x the fiber, slightly more carbs, and more than 2x the protein, winning this first round easily.
In the category of vitamins, bell peppers have more of vitamins C and E, while okra has more of vitamins B2, B3, B5, B6, B9, and K, winning by a large margin. You might be wondering about vitamin A; if the bell peppers are red or yellow, then they have more; if the bell peppers are green, then okra has more. Doesn’t change the overall result for the category though; it’s still, on balance, a clear win for okra on vitamins either way.
Looking at minerals, bell peppers are not higher in any minerals, while okra has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, for an even more one-sided victory for okra in this round.
In other considerations, okra is higher in polyphenols, so that’s another point in okra’s favor.
Adding up the sections makes for a very clear overall win for okra, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
A Spectrum Of Specialties: Which Bell Peppers To Pick? ← about the various differences between the assorted colors of bell pepper
Enjoy!
Share This Post
-
Mouthwatering Protein Falafel
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Baking falafel, rather than frying it, has a strength and a weakness. The strength: it is less effort and you can do more at once. The weakness: it can easily get dry. This recipe calls for baking them in a way that won’t get dry, and the secret is one of its protein ingredients: peas! Add to this the spices and a tahini sauce, and you’ve a mouthwatering feast that’s full of protein, fiber, polyphenols, and even healthy fats.
You will need
- 1 cup peas, cooked
- 1 can chickpeas, drained and rinsed (keep the chickpea water—also called aquafaba—aside, as we’ll be using some of it later)
- ½ small red onion, chopped
- 1 handful fresh mint, chopped
- 1 tbsp fresh parsley, chopped
- ½ bulb garlic, crushed
- 1 tbsp lemon juice
- 1 tbsp chickpea flour (also called gram flour, besan flour, or garbanzo bean flour) plus more for dusting
- 2 tsp red chili flakes (adjust per heat preferences)
- 2 tsp black pepper, coarse ground
- 1 tsp ground turmeric
- ½ tsp MSG or 1 tsp low-sodium salt
- Extra virgin olive oil
For the tahini sauce:
- 2 tbsp tahini
- 2 tbsp lemon juice
- ¼ bulb garlic, crushed
- 5 tbsp aquafaba (if for some reason you don’t have it, such as for example you substituted 1 cup chickpeas that you cooked yourself, substitute with water here)
To serve:
- Flatbreads (you can use our Healthy Homemade Flatbreads recipe if you like)
- Leafy salad
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 350℉ / 180℃.
2) Blend the peas and chickpeas in a food processor for a few seconds. You want a coarse mixture, not a paste.
3) Add the rest of the main section ingredients except the olive oil, and blend again for a few more seconds. It should still have a chunky texture, or else you will have made hummus. If you accidentally make hummus, set your hummus aside and start again on the falafels.
4) Shape the mixture into balls; if it lacks structural integrity, fold in a little more chickpea flour until the balls stay in shape. Either way, once you have done that, dust the balls in chickpea flour.
5) Brush the balls in a little olive oil, as you put them on a baking tray lined with baking paper. Bake for 15–18 minutes until golden, turning partway through.
6) While you are waiting, making the tahini sauce by combining the tahini sauce ingredients in a high-speed blender and processing on high until smooth. If you do not have a small enough blender (a bullet-style blender should work for this), then do it manually, which means you’ll have to crush the garlic all the way into a smooth paste, such as with a pestle and mortar, or alternatively, use ready-made garlic paste—and then simply whisk the ingredients together until smooth.
7) Serve the falafels warm or cold, on flatbreads with leafy salad and the tahini sauce.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Tahini vs Hummus – Which is Healthier?
- Our Top 5 Spices: How Much Is Enough For Benefits? ← we scored 4/5 today!
Take care!
Share This Post
-
If You Don’t Have Time To Work Out…
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s easy to think “I don’t have time to exercise” and mean it. It’s easy to procrastinate things until that “starting tomorrow” is six months later. After all, exercise can be done tomorrow whereas many other tasks need to be done today. However, there are still ways we can carve out time for exercise, without sacrificing other things (including sleep etc!). Here’s how:
Bit by bit
The trick is to create momentum by starting small and designing workouts around limited time. For example:
- Temptation bundling: this works the same for a shortage of time as it does for a shortage of motivation. The idea is to pair workouts with low-energy leisure activities (e.g. watching TV, scrolling social media).
- Exercise snacking: take short movement breaks during the day (e.g. 5 minutes between other activities). Each may seem almost irrelevant by itself, but small efforts add up and help build momentum and consistency.
- Focus on frequency first: daily short sessions (10–15 min) are better for habit formation than occasional long workouts, which helps you to build a routine and makes it easier to scale up later.
Then, once you are having dedicated exercise sessions, make the most out of them (but still in a sustainable fashion):
- Set a timer: structure your workout to fit the available time (e.g. 5, 10, or 15 minutes). Timers also create focus and make workouts more efficient; you’ll no longer be getting distracted between sets.
- Use compound movements: focus on exercises that work multiple muscle groups (e.g. squats, push-ups, rows). This allows more muscle engagement and calorie burn in less time.
- Avoid working to failure: perhaps counterintuitive since you’re looking to get the most out of each exercise, but there’s logic here: pushing to exhaustion will tend to lead to sacrificing form, and will increase recovery times. Now, there are reasons why training to exhaustion can be beneficial, but while you’re still at the point of just trying to find enough time to exercise? That’s not the time for training to exhaustion and taking 48 hours to recover.
For more on all of these things, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
How Useful Is “Exercise Snacking”, Really?
Take care!
Share This Post



Related Posts
-

The push for Medicare to cover weight-loss drugs: An explainer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The largest U.S. insurer, Medicare, does not cover weight-loss drugs, making it tougher for older people to get access to promising new medications.
If you cover stories about drug costs in the U.S., it’s important to understand why Medicare’s Part D pharmacy program, which covers people aged 65 and older and people with certain disabilities, doesn’t cover weight-loss drugs today. It’s also important to consider what would happen if Medicare did start covering weight loss drugs. This explainer will give you a brief overview of the issues and then summarize some recent publications the benefits and costs of drugs like semaglutide and tirzepatide.
First, what are these new and newsy weight loss drugs?
Semaglutide is a medication used for both the treatment of type 2 diabetes and for long-term weight management in adults with obesity. It debuted in the United States in 2017 as an injectable diabetes drug called Ozempic, manufactured by Novo Nordisk. It’s part of a class of drugs that mimics the action of glucagon, a substance that the human body makes to aid digestion.
Glucagon-like peptide-1 (GLP-1) drugs like semaglutide help prompt the body to release insulin. But they also cause a minor delay in the pace of digestion, helping people feel sated after eating.
That second effect turned Ozempic into a widely used weight-loss drug, even before the Food and Drug Administration (FDA) gave its okay for this use. Doctors in the United States can prescribe medicines for uses beyond those approved by the FDA. This is known as off-label use.
In writing about her own experience in using the medicine to help her shed 40 pounds, Washington Post columnist Ruth Marcus in June noted that Novo Nordisk mentioned the potential for weight loss in its “ubiquitous cable ads (‘Oh-oh-oh, Ozempic!’)”
The American Society of Health-System Pharmacists has reported shortages of semaglutide due to demand, leaving some people with diabetes struggling to find supply of the medicine.
Novo Nordisk won Food and Drug Administration (FDA) approval in 2021 to market semaglutide as an injectable weight loss drug under the name Wegovy, but with a different dosing regimen than Ozempic. Rival Eli Lilly first won FDA approval of its similar GLP-1 diabetes drug, tirzepatide, in the United States in 2022 and sells it under the brand name Mounjaro.
In November of 2023, Eli Lilly won FDA approval to sell tirzepatide as a weight-loss drug, soon-to-be marketed under the brand name Zepbound. The company said it will set a monthly list price for a month’s supply of the drug at $1,059.87, which the company described as 20% discount to the cost of rival Novo Nordisk’s Wegovy. Wegovy has a list price of $1,349.02, according to the Novo Nordisk website.
Even when their insurance plans officially cover costs for weight loss drugs, consumers may face barriers in seeking that coverage for these drugs. Commercial health plans have in place prior authorization requirements to try to limit coverage of new weight-loss shots to those who qualify for these treatments. The Wegovy shot, for example, is intended for people whose weight reaches a certain benchmark for obesity or who are overweight and have a condition related to excess weight, such as diabetes, high blood pressure or high cholesterol.
State Medicaid programs, meanwhile, have taken approaches that vary by state. For example, the most populous U.S. state, California, provides some coverage to new weight-loss injections through its Medicaid program, but many others, including Texas, the No. 2 state in terms of population, do not, according to an online tool that Novo Nordisk created to help people check on coverage.
Medicare does cover semaglutide for treatment of diabetes, and the insurer reported $3 billion in 2021 spending on the drug under Medicare Part D. Congress last year gave Medicare new tools that might help it try to lower the cost of semaglutide.
Medicare is in the midst of implementing new authority it gained through the Inflation Reduction Act (IRA) of 2022 to negotiate with companies about the cost of certain medicines.
This legislation gave Medicare, for the first time, tools to directly negotiate with pharmaceutical companies on the cost of some medicines. Congress tailored this program to spare drug makers from negotiations for the first few years they put new medicines on the market, allowing them to recoup investment in these products.
Why doesn’t Medicare cover weight-loss drugs?
Congress created the Medicare Part D pharmacy program in 2003 to address a gap in coverage that had existed since the creation of Medicare in 1965. The program long covered the costs of drugs administered by doctors and those given in hospitals, but not the kinds of medicines people took on their own, like Wegovy shots.
In 2003, there seemed to be good reasons to leave weight-loss drugs out of the benefit, write Inmaculada Hernandez of the University of California, San Diego, and coauthors in their September 2023 editorial in the Journal of General Internal Medicine, “Medicare Part D Coverage of Anti-obesity Medications: a Call for Forward-Looking Policy Reform.”
When members of Congress worked on the Part D benefit, the drugs available on the market were known to have limited effectiveness and unpleasant side effects. And those members of Congress were aware of how a drug combination called fen-phen, once touted as a weight-loss miracle medicine, turned out in rare cases to cause fatal heart valve damage. In 1997, American Home Products, which later became Wyeth, took its fen-phen product off the market.
But today GLP-1 drugs like semaglutide appear to offer significant benefits, with far less risk and milder side effects, write Hernandez and coauthors.
“Other than budget impact, it is hard to find a reason to justify the historical statutory exclusion of weight loss drugs from coverage other than the stigma of the condition itself,” they write.
What’s happening today that could lead Medicare to start covering weight loss drugs?
Novo Nordisk and Eli Lilly both have hired lobbyists to try to persuade lawmakers to reverse this stance, according to Senate records. Pro tip: You can use the Senate’s lobbying disclosure database to track this and other issues. Type in the name of the company of interest and then read through the forms.
Some members of Congress already have been trying for years to strike the Medicare Part D restriction on weight-loss drugs. Over the past decade, senators Tom Carper (D-DE) and Bill Cassidy, MD, (R-LA) have repeatedly introduced bills that would do that. They introduced the current version, the Treat and Reduce Obesity Act of 2023, in July. It has the support of 10 other Republican senators and seven Democratic ones, as of Dec. 19. The companion House measure has the support of 41 Democrats and 23 Republicans in that chamber, which has 435 seats.
The influential nonprofit Institute for Clinical and Economic Review conducts in-depth analyses of drugs and medical treatments in the United States. ICER last year recommended passage of a law allowing Medicare Part D to cover weight-loss medications. ICER also called for broader coverage of weight-loss medications in state Medicaid programs. Insurers, including Medicare, consider ICER’s analyses in deciding whether to cover treatments.
While offering these calls for broader coverage as part of a broad assessment of obesity management, ICER also urged companies to reduce the costs of weight-loss medicines.
Most people with obesity can’t achieve sustained weight loss through diet and exercise alone, said David Rind, ICER’s chief medical officer in an August 2022 statement. The development of newer obesity treatments represents the achievement of a long-standing goal of medical research, but prices of these new products must be reasonable to allow broad access to them, he noted.
After an extensive process of reviewing studies, engaging in public debate and processing feedback, ICER concluded that semaglutide for weight loss should have an annual cost of $7,500 to $9,800, based on its potential benefits.
What does academic research say about the benefits and the potential costs of new obesity drugs?
Here are a couple of studies to consider when covering the ongoing story of weight-loss drug costs:
Medicare Part D Coverage of Antiobesity Medications — Challenges and Uncertainty Ahead
Khrysta Baig, Stacie B. Dusetzina, David D. Kim and Ashley A. Leech. New England Journal of Medicine, March 2023In this Perspective piece, researchers at Vanderbilt University create a series of estimates about how much Medicare may have to spend annually on weight-loss drugs if the program eventually covers these drugs.
These include a high estimate — $268 billion — based on an extreme calculation, one reflecting the potential cost if virtually all people on Medicare who have obesity used semaglutide. In an announcement of the study on the Vanderbilt website, lead author Khrysta Baig described this as a “purely hypothetical scenario,” but one that “ underscores that at current prices, these medications cannot be the only way – or even the main way – we address obesity as a society.”
In a more conservative estimate, Bhaig and coauthors consider a case where only about 10% of those eligible for obesity treatment opted for semaglutide, which would result in $27 billion in new costs.
(To put these numbers in context, consider that the federal government now spends about $145 billion a year on the entire Part D program.)
It’s likely that all people enrolled in Part D would have to pay higher monthly premiums if Medicare were to cover weight-loss injections, Baig and coauthors write.
Baig and coauthors note that the recent ICER review of weight-loss drugs focused on patients younger than the Medicare population. The balance of benefits and risks associated with weight-loss drugs may be less favorable for older people than the younger ones, making it necessary to study further how these drugs work for people aged 65 and older, they write. For example, research has shown older adults with a high blood sugar level called prediabetes are less likely to develop diabetes than younger adults with this condition.
SELECTing Treatments for Cardiovascular Disease — Obesity in the Spotlight
Amit Khera and Tiffany M. Powell-Wiley. New England Journal of Medicine, Dec. 14, 2023
Semaglutide and Cardiovascular Outcomes in Patients Without Diabetes
A Michael Lincoff, et. al. New England Journal of Medicine, Dec. 14, 2023.An editorial accompanies the publication of a semaglutide study that drew a lot of coverage in the media. The Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes (SELECT) study was a randomized controlled trial, conducted by Novo Nordisk, which looked at rates of cardiovascular events in people who already had known heart risk and were overweight, but not diabetic. Patients were randomly assigned to receive a once-weekly dose of semaglutide (Wegovy) or a placebo.
In the study, the authors report that of the 8,803 patients who took Wegovy in the trial, 569 (6.5%)
The study also reports a mean 9.4% reduction in body weight among patients taking Wegovy, while those on placebo had a mean loss of 0.88%.
The findings suggest Wegovy may be a welcome new treatment option for many people who have coronary disease and are overweight, but are not diabetic, write Khera and Powell-Wiley in their editorial.
But the duo, both of whom focus on disease prevention in their research, also call for more focus on the prevention and root causes of obesity and on the use of proven treatment approaches other than medication.
“Socioeconomic, environmental, and psychosocial factors contribute to incident obesity, and therefore equity-focused obesity prevention and treatment efforts must target multiple levels,” they write. “For instance, public policy targeting built environment features that limit healthy behaviors can be coupled with clinical care interventions that provide for social needs and access to treatments like semaglutide.”
Additional information:
The nonprofit KFF, formerly known as the Kaiser Family Foundation, has done recent reports looking at the potential for expanded coverage of semaglutide:
Medicaid Utilization and Spending on New Drugs Used for Weight Loss, Sept. 8, 2023
What Could New Anti-Obesity Drugs Mean for Medicare? May 18, 2023
And KFF held an Aug. 4 webinar, New Weight Loss Drugs Raise Issues of Coverage, Cost, Access and Equity, for which the recording is posted here.
This article first appeared on The Journalist’s Resource and is republished here under a Creative Commons license.

Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Can apps and digital resources support your child with autism or ADHD?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Neurodevelopmental conditions such as attention deficit hyperactivity disorder (ADHD) and autism affect about one in ten children. These conditions impact development, behaviour and wellbeing.
But children with these conditions and their caregivers often can’t get the support they need. Families report difficulties accessing health-care providers and experience long wait lists to receive care.
Digital tools, such as apps and websites, are often viewed as a solution to these gaps. With a single click or a download, families might be able to access information to support their child.
There are lots of digital tools available, but it’s hard to know what is and isn’t useful. Our new study evaluated freely available digital resources for child neurodevelopment and mental health to understand their quality and evidence base.
We found many resources were functional and engaging. However, resources often lacked evidence for the information provided and the claimed positive impact on children and families.
This is a common problem in the digital resource field, where the high expectations and claims of impact from digital tools to change health care have not yet been realised.
Fabio Principe/Shutterstock What type of resources?
Our study identified 3,435 separate resources, of which 112 (43 apps and 69 websites) met our criteria for review. These resources all claimed to provide information or supports for child neurodevelopment, mental health or wellbeing.
Resources had to be freely available, in English and have actionable information for children and families.
The most common focus was on autism, representing 17% of all resources. Resources suggested they provided strategies to promote speech, language and social development, and to support challenging behaviours.
Other common areas included language and communication (14%), and ADHD (10%).
Resources had various purposes, including journalling and providing advice, scheduling support, and delivering activities and strategies for parents. Resources delivered information interactively, with some apps organising content into structured modules.
Resources also provided options for alternative and assistive communication for people with language or communication challenges.
Most apps were functional and accessible
Our first question was about how engaging and accessible the information was. Resources that are hard to use aren’t used frequently, regardless of the information quality.
We evaluated aesthetics, including whether digital tools were easy to use and navigate, stylistically consistent, with clean and appealing graphics for users.
Most resources were rated as highly engaging, with strong accessibility and functionality.
Most apps and websites we evaluated were engaging. jamesteohart/Shutterstock But many lacked quality information
We ranked resources on various features from 1 (inadequate) to 5 (excellent), with a ranking of 3 considered acceptable. These ratings looked at how credible the resource was and whether there was evidence supporting it.
Despite their functionality, 37% of reviewed apps did not meet the minimum acceptable standards for information quality. This means many apps could not be recommended. Most websites fared better than apps.
There also wasn’t a lot of scientific evidence to suggest using either apps or digital resources actually helped families. Studies show long-term engagement with digital tools is rare, and downloads don’t correspond to frequent usage or benefits.
Digital tools are often viewed as a panacea to health-care gaps, but the evidence is yet to show they fill such gaps. Digital health is a fast-moving field and resources are often made available before they have been properly evaluated.
What should you look for in digital resources?
We found the highest quality resources were developed in collaboration with institutions, such as health, university or government groups.
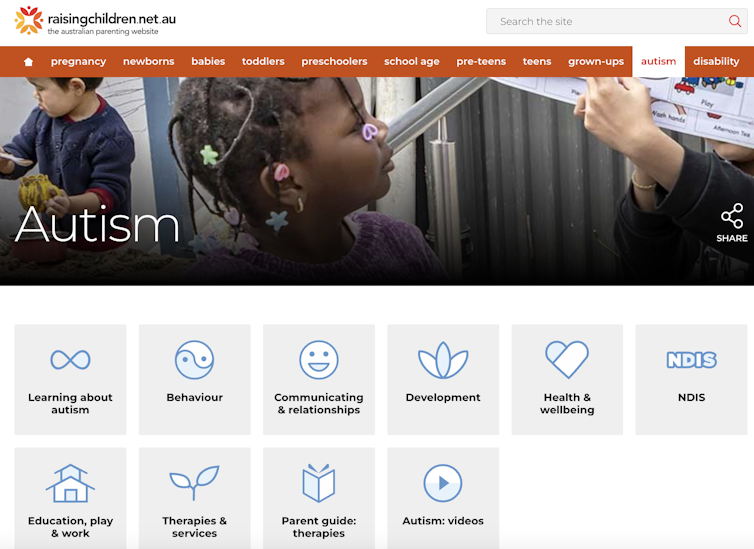
One highly rated resource was the Raising Children’s Network and the associated app, Raising Healthy Minds. These are co-developed with a university and hospital, and by people with appropriate qualifications.
This resource provides information to support children’s overall health, development and wellbeing, with dedicated sections addressing neurodevelopmental needs and concerns.
The Raising Children Network provides resources for child health, including neurodevelopmental needs. Raising Children Network screenshot Our research shows parents can assess whether digital resources are high quality by checking they are:
- factually correct. Look for where the app or resource is getting its information. Does the author have the qualifications and training to provide the information? Are they a registered health expert who is accountable to a regulatory body (such as AHPRA, the Australian Health Practitioners Regulation Agency) for providing information that does not cause harm?
- consistent across multiple credible sources, such as health institutions.
- linked to supporting information. Look for reliable links to reputable institutions. Links to peer-reviewed scientific journals are often helpful as those articles will also usually describe the limitations of the research presented.
- up-to-date. Apps should be frequently updated. For websites, dates of update are usually found on the homepage or at the bottom of individual pages.
Check when information was last updated. fizkes/Shutterstock Beware of red flags
Some things to watch out for are:
- testimonials and anecdotes without evidence and scientific links to back the anecdotes up. If it sounds too good to be true, it probably is.
- no information provided about conflicts of interest. Organisations gain when you click on their links or take their advice (financial, reputation and brand development). Think about what they gain when you use their information to help keep a balanced perspective.
Remember, the app’s star rating doesn’t mean it will contain factual information from a reliable source or be helpful for you and your child.
The role of digital tools
Digital tools won’t usually replace a health professional, but they can support care in many different ways. They may be used to help to educate and prepare for meetings, and to collaborate with health providers.
They may also be used to collect information about daily needs. Studies show reporting on sleep in children can be notoriously difficult, for example. But tracking sleep behaviour with actigraphy, where movement and activity patterns are measured using a wearable device, can provide information to support clinical care. With the promise of artificial intelligence, there will also be new opportunities to support daily living.
Our findings reflect a broader problem for digital health, however. Much investment is often made in developing products to drive use, with spurious claims of health benefits.
What’s needed is a system that prioritises the funding, implementation and evaluation of tools to demonstrate benefits for families. Only then may we realise the potential of digital tools to benefit those who use them.
Kelsie Boulton, Senior Research Fellow in Child Neurodevelopment, Brain and Mind Centre, University of Sydney and Adam Guastella, Professor and Clinical Psychologist, Michael Crouch Chair in Child and Youth Mental Health, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
10 Minoxidil Hacks For The Best Hair Growth
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Shereene Idriss advises:
Keep your hair on…
Ok, we would note that tips 1 and 2 seem to be the same (but honestly, it’s a big myth to bust so it bears saying twice), and tips 4 and 10 are more advice about its limitations than actual tips, but we include them all here so that you know we didn’t short-change you!
Number 3 is great advice in particular, as is number 6 if it applies to you; a lot of people don’t think of it:
- Choose between 2% and 5% minoxidil, regardless of gender—5% is more effective and often more cost-efficient.
- Women can safely use the 5% minoxidil strength; avoid the “pink tax” of products marketed specifically to women at a higher price for a lower concentration.
- Consistency matters more than intensity—use minoxidil several times a week if daily application isn’t realistic, and think of results long-term.
- Expect initial shedding between weeks 2–6; this is temporary and normal—results typically start showing after 3 months.
- Apply minoxidil precisely to target areas to avoid unwanted hair growth on the face or body, and wash your hands after use.
- You can use minoxidil with a spoolie brush to regrow thinning eyebrows—just clean the area after application.
- Microneedling the scalp before applying minoxidil can improve absorption and results, but only if done gently and hygienically.
- Minoxidil is toxic to dogs and cats—store it safely, wash your hands after use, and keep it away from your animals at all times.
- If topical minoxidil causes irritation, oral minoxidil (prescription only) may be an alternative—just be aware of possible systemic side effects like unwanted body hair.
- Minoxidil is not a cure but a maintenance treatment—once you stop, hair loss will likely resume, so combine it with other strategies if needed.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
What’s The Difference Between Minoxidil For Men vs For Women?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: