Broccoli vs Kale – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing broccoli to kale, we picked the kale.
Why?
Both are great, but there was a very clear winner:
In terms of macros, kale has more fiber, carbs, and protein, winning this round.
In the category of vitamins, broccoli has more vitamin B5 and choline, while kale has more of vitamins A, B1, B2, B3, B6, B7, B9, C, E, and K, winning easily.
Looking at minerals, broccoli has more selenium, while kale has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, and zinc, scoring its third win in a row.
In other considerations, kale has more polyphenols, and carotenoids too (which are by definition not polyphenols, but fulfil a similarly beneficial role).
Adding up the sections makes for a clear win for kale, but by all means enjoy either or both; broccoli really is great as well—it just doesn’t look it when standing next to kale!
Want to learn more?
You might like:
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How To Regrow Receding Gums

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One of the problems with the human form is that our teeth evolved to last us for the whole of our life, with plenty of room to spare before our eventual death at the ripe old age of about 35 on average. Dr. Ellie Phillips advises those of us who might be a bit older than that, on how we can avoid becoming “too long in the tooth”—in other words, how to keep our gums, and thus our teeth, in place and healthy.
Getting to the root of the problem
The single biggest cause of gum recession is an acidic environment in the mouth, which harms teeth and gums alike. This acidic environment is produced not merely by consuming acid foods or drinks, but also (and much more often, and more problematically) by sugary foods and drinks, which are not necessarily themselves acidic, but they feed bacteria that release acids as a by-product of their metabolism. If we consume an acidic food or drink, it’s there for a moment, but if we then salivate and/or take a drink of water, it’s pretty much gone in a few seconds. But those bacteria when we feed them sugar? They are there to stay unless we do something more about them than just drink some water.
Other contributing factors to gum recession include teeth grinding, and (ironically) certain oral care products, especially many artificial teeth whiteners.
In case you were wondering: no, brushing will not* generally cause or even worsen gum recession, but flossing can exacerbate it if it’s already underway.
*unless, of course, you are using one of the whiteners we mentioned above
What to do about it: Dr. Phillips recommends:
- use a moderately firm toothbrush to massage gums and promote blood flow
- avoid acidic oral products and homemade remedies even if they’re not acidic but can be caustic, such as baking soda
- rebuild your gums’ and teeth’s protective biofilm (yes, there are “good bacteria” that are supposed to be there) with proper brushing
- avoid cleanings that are more intensive than brushing—skip flossing until your gums have recovered, too
- adjust your diet to avoid acids and (especially) sugars
10almonds note: she also recommends the use of xylitol to promote a healthy oral environment; we don’t recommend that, as while it may be great for the teeth, studies have found it to be bad for the heart.
For more on all of her advices and a bit more of the science of it, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Toothpastes & Mouthwashes: Which Help And Which Harm?
- Flossing Without Flossing?
- Less Common Oral Hygiene Options ← including the miswak “chewing stick”, which even outperformed toothbrushes in clinical trials, by biochemically altering the composition of the saliva while gently cleaning like a toothbrush.
- Fluoride Toothpaste vs Non-Fluoride Toothpaste – Which is Healthier?
- Non-Alcohol Mouthwash vs Alcohol Mouthwash – Which is Healthier?
- Xylitol vs Erythritol – Which is Healthier?
Take care!
Share This Post
-

Surgery is the default treatment for ACL injuries in Australia. But it’s not the only way
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
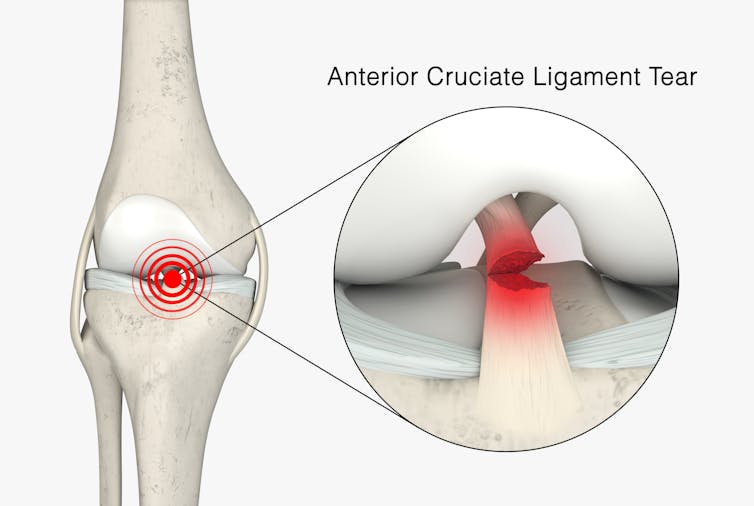
The anterior cruciate ligament (ACL) is an important ligament in the knee. It runs from the thigh bone (femur) to the shin bone (tibia) and helps stabilise the knee joint.
Injuries to the ACL, often called a “tear” or a “rupture”, are common in sport. While a ruptured ACL has just sidelined another Matildas star, people who play sport recreationally are also at risk of this injury.
For decades, surgical repair of an ACL injury, called a reconstruction, has been the primary treatment in Australia. In fact, Australia has among the highest rates of ACL surgery in the world. Reports indicate 90% of people who rupture their ACL go under the knife.
Although surgery is common – around one million are performed worldwide each year – and seems to be the default treatment for ACL injuries in Australia, it may not be required for everyone.

PeopleImages.com – Yuri A/Shutterstock What does the research say?
We know ACL ruptures can be treated using reconstructive surgery, but research continues to suggest they can also be treated with rehabilitation alone for many people.
Almost 15 years ago a randomised clinical trial published in the New England Journal of Medicine compared early surgery to rehabilitation with the option of delayed surgery in young active adults with an ACL injury. Over half of people in the rehabilitation group did not end up having surgery. After five years, knee function did not differ between treatment groups.
The findings of this initial trial have been supported by more research since. A review of three trials published in 2022 found delaying surgery and trialling rehabilitation leads to similar outcomes to early surgery.
A 2023 study followed up patients who received rehabilitation without surgery. It showed one in three had evidence of ACL healing on an MRI after two years. There was also evidence of improved knee-related quality of life in those with signs of ACL healing compared to those whose ACL did not show signs of healing.
Experts used to think an ACL tear couldn’t heal without surgery – now there’s evidence it can. SKYKIDKID/Shutterstock Regardless of treatment choice the rehabilitation process following ACL rupture is lengthy. It usually involves a minimum of nine months of progressive rehabilitation performed a few days per week. The length of time for rehabilitation may be slightly shorter in those not undergoing surgery, but more research is needed in this area.
Rehabilitation starts with a physiotherapist overseeing simple exercises right through to resistance exercises and dynamic movements such as jumping, hopping and agility drills.
A person can start rehabilitation with the option of having surgery later if the knee remains unstable. A common sign of instability is the knee giving way when changing direction while running or playing sports.
To rehab and wait, or to go straight under the knife?
There are a number of reasons patients and clinicians may opt for early surgical reconstruction.
For elite athletes, a key consideration is returning to sport as soon as possible. As surgery is a well established method, athletes (such as Matilda Sam Kerr) often opt for early surgical reconstruction as this gives them a more predictable timeline for recovery.
At the same time, there are risks to consider when rushing back to sport after ACL reconstruction. Re-injury of the ACL is very common. For every month return to sport is delayed until nine months after ACL reconstruction, the rate of knee re-injury is reduced by 51%.
For people who opt to try rehabilitation, the option of having surgery later is still there. PeopleImages.com – Yuri A/Shutterstock Historically, another reason for having early surgical reconstruction was to reduce the risk of future knee osteoarthritis, which increases following an ACL injury. But a review showed ACL reconstruction doesn’t reduce the risk of knee osteoarthritis in the long term compared with non-surgical treatment.
That said, there’s a need for more high-quality, long-term studies to give us a better understanding of how knee osteoarthritis risk is influenced by different treatments.
Rehab may not be the only non-surgical option
Last year, a study looking at 80 people fitted with a specialised knee brace for 12 weeks found 90% had evidence of ACL healing on their follow-up MRI.
People with more ACL healing on the three-month MRI reported better outcomes at 12 months, including higher rates of returning to their pre-injury level of sport and better knee function. Although promising, we now need comparative research to evaluate whether this method can achieve similar results to surgery.
What to do if you rupture your ACL
First, it’s important to seek a comprehensive medical assessment from either a sports physiotherapist, sports physician or orthopaedic surgeon. ACL injuries can also have associated injuries to surrounding ligaments and cartilage which may influence treatment decisions.
In terms of treatment, discuss with your clinician the pros and cons of management options and whether surgery is necessary. Often, patients don’t know not having surgery is an option.
Surgery appears to be necessary for some people to achieve a stable knee. But it may not be necessary in every case, so many patients may wish to try rehabilitation in the first instance where appropriate.
As always, prevention is key. Research has shown more than half of ACL injuries can be prevented by incorporating prevention strategies. This involves performing specific exercises to strengthen muscles in the legs, and improve movement control and landing technique.
Anthony Nasser, Senior Lecturer in Physiotherapy, University of Technology Sydney; Joshua Pate, Senior Lecturer in Physiotherapy, University of Technology Sydney, and Peter Stubbs, Senior Lecturer in Physiotherapy, University of Technology Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
The United States CDC has abandoned science in its new advice about vaccines and autism
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The United States Centers for Disease Control and Prevention (CDC) has revised its long-standing guidance about vaccines and autism.
The guidance once stated clearly and correctly that the evidence shows no link between vaccines and the development of autism.
Now it claims “studies supporting a link [between vaccines and autism] have been ignored by health authorities”. It also says:
The claim “vaccines do not cause autism” is not an evidence-based claim because studies have not ruled out the possibility that infant vaccines cause autism.
Health Secretary Robert F. Kennedy Jr directed the CDC to make these changes, despite promising at his confirmation not to alter the CDC’s vaccine advice.
With this change in wording on the website the CDC has been dragged to a new low. The CDC once stood as a global benchmark of scientific integrity. Sadly, it now risks becoming a megaphone for misinformation and a tool for those whose goal is to undermine science.
Let’s look at the updated CDC statement about vaccines and autism, and how this is at odds with how science works.
Science can’t prove universal negatives
Saying “studies have not ruled out the possibility that infant vaccines cause autism” is in direct conflict with how science works.
Using science, we can demonstrate that two things are linked by showing consistent, reproducible associations that stand up across multiple study designs. We can also test a hypothesis repeatedly and from many angles.
Therefore, for example, when high-quality studies using different methods, populations and measurements, all fail to find a link between vaccines and autism, the rational conclusion is there is no causal connection.
But we cannot prove the universal absence of a link.
If we were to accept this notion, someone could always claim they aren’t convinced by the current evidence because maybe the next study will find something. Using this same logic, it’s impossible to rule out the Earth is flat or that fairies exist.
It’s wrong to reverse the burden of proof
Another dangerous premise in the CDC’s new framing on vaccines and autism is it reverses the burden of proof.
In science, the person making a claim, especially one that argues against the available consensus, must provide the evidence for it.
The rhetorical manoeuvre on the CDC website suggesting proof is required to show the absence of a link, however, flips this principle on its head. It suggests it’s reasonable to expect scientists to defend against an infinite list of hypothetical possibilities.
But as US astronomer Carl Sagan famously put it, “extraordinary claims require extraordinary evidence”. In science, if you want to assert something that contradicts the scientific consensus, the burden is on you to produce evidence strong enough to justify overturning what we already know.
The more implausible a claim is, the higher the bar in providing high quality, reproducible and methodologically sound research to support it.
By asking the CDC to alter its website guidance, RFK Jr wants you to accept the opposite: that he or anyone can make any claim and it’s the responsibility of everyone else to disprove these claims.
It’s also unclear what evidence would change RFK Jr’s mind on vaccines and autism. This leaves the door open for him to claim any amount of evidence that doesn’t support his preferred narrative is insufficient.
But what about the study that claimed to be proof?
Speculation about a link between the measles, mumps and rubella (MMR) vaccine and autism began with a fraudulent and now-retracted 1998 Lancet paper by the discredited doctor Andrew Wakefield.
Even if you accepted everything in Wakefield’s paper as true (it wasn’t) and assumed he was an honest researcher (he wasn’t), you would still be left with nothing more than a case series of 12 children. This study design is incapable of establishing a causal link between the MMR vaccine and autism.
Subsequent investigations also uncovered a long list of damning findings about Wakefield, including:
1) He hid major financial conflicts of interest
Wakefield was paid large sums by lawyers preparing a lawsuit against MMR manufacturers, money he failed to disclose. He was contracted to find evidence supporting a link between MMR and autism.
At the same time, he had filed patents for a single-dose measles vaccine and a diagnostic test that stood to profit if public fear about MMR increased.
2) He committed serious ethical violations
Wakefield falsely claimed the study had ethics approval. It did not. Children with developmental conditions were subjected to invasive procedures, including colonoscopies and lumbar punctures, without valid clinical justification or proper oversight.
3) He misrepresented how the children were recruited
The paper claimed the children were consecutively referred, implying an unbiased clinical sample. In reality, several were recruited through anti-vaccine groups or families involved in the lawsuit funding Wakefield, meaning the sample was deliberately cherry-picked to support his predetermined hypothesis.
4) He altered and falsified data
Comparisons between medical records and the published paper revealed extensive falsification:
- symptoms that began before vaccination were rewritten as occurring after MMR
- gastrointestinal findings were exaggerated or invented
- diagnoses were manipulated to fit his fabricated “autistic enterocolitis” syndrome
- normal clinical results were presented as abnormal.
The tragedy in all this is that a fraudulent study that never should have seen the light of day continues, even now, to erode confidence in life-saving vaccines. This has led to reduced vaccination rates, the resurgence of preventable childhood illnesses, and unnecessary deaths.
It has also inflicted immeasurable harm on autistic people and their families by fuelling stigma and misinformation.
Hassan Vally, Associate Professor, Epidemiology, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post




Related Posts
-

Plant-Based Alternatives for Meat Recipes
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝How about providing a plant-based alternative when you post meat-based recipes? I appreciate how much you advocate for veggie diets and think offering an alternative with your recipes would support that❞
Glad you’re enjoying! And yes, we do usually do that. But: pardon, we missed one (the Tuna Steak with Protein Salad) because it’d be more than a simple this-for-that substitution, we didn’t already have an alternative recipe up (as with the salmon recipes such as the Chili Hot-Bedded Salmon and Thai Green Curry Salmon Burgers).
Our recipes, by the way, will tend towards being vegan, vegetarian, or at least pescatarian. This is for several reasons:
- Good science suggests the best diet for general purpose good health is one that is mostly plants, with optional moderate amounts of fermented dairy products, fish, and/or eggs.
- Your writer here (it’s me, hi) has been vegan for many years, transitioning to such via pescatarianism and ovo-lacto vegetarianism, and so the skill of cooking meat is least fresh in my memory, meaning I’d not be confident writing about that, especially as cooking meat has the gravest health consequences for messing it up.
Note on biases: notwithstanding this writer being vegan, we at 10almonds are committed to reporting the science as it stands with no agenda besides good health. Hence, there will continue to be unbiased information about animal products’ health considerations, positive as well as negative.
See also: Do We Need Animal Products To Be Healthy?
…as well as, of course, some animal-based classics from our archives including:
We Are Such Stuff As Fish Are Made Of & Eggs: All Things In Moderation?
Finishing with one for the vegans though, you might enjoy:
Which Plant Milk? We Compare 6 Of The Most Popular
Some previous articles you might enjoy meanwhile:
- Pinpointing The Usefulness Of Acupuncture
- Science-Based Alternative Pain Relief
- Peripheral Neuropathy: How To Avoid It, Manage It, Treat It
- What Does Lion’s Mane Actually Do, Anyway?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What is ‘doll therapy’ for people with dementia? And is it backed by science?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The way people living with dementia experience the world can change as the disease progresses. Their sense of reality or place in time can become distorted, which can cause agitation and distress.
One of the best ways to support people experiencing changes in perception and behaviour is to manage their environment. This can have profound benefits including reducing the need for sedatives.
One such strategy is the use of dolls as comfort aids.
Jack Cronkhite/Shutterstock What is ‘doll therapy’?
More appropriately referred to as “child representation”, lifelike dolls (also known as empathy dolls) can provide comfort for some people with dementia.
Memories from the distant past are often more salient than more recent events in dementia. This means that past experiences of parenthood and caring for young children may feel more “real” to a person with dementia than where they are now.
Hallucinations or delusions may also occur, where a person hears a baby crying or fears they have lost their baby.
Providing a doll can be a tangible way of reducing distress without invalidating the experience of the person with dementia.
Some people believe the doll is real
A recent case involving an aged care nurse mistreating a dementia patient’s therapy doll highlights the importance of appropriate training and support for care workers in this area.
For those who do become attached to a therapeutic doll, they will treat the doll as a real baby needing care and may therefore have a profound emotional response if the doll is mishandled.
It’s important to be guided by the person with dementia and only act as if it’s a real baby if the person themselves believes that is the case.
What does the evidence say about their use?
Evidence shows the use of empathy dolls may help reduce agitation and anxiety and improve overall quality of life in people living with dementia.
Child representation therapy falls under the banner of non-pharmacological approaches to dementia care. More specifically, the attachment to the doll may act as a form of reminiscence therapy, which involves using prompts to reconnect with past experiences.
Interacting with the dolls may also act as a form of sensory stimulation, where the person with dementia may gain comfort from touching and holding the doll. Sensory stimulation may support emotional well-being and aid commnication.
However, not all people living with dementia will respond to an empathy doll.
It depends on a person’s background. Shutterstock The introduction of a therapeutic doll needs to be done in conjunction with careful observation and consideration of the person’s background.
Empathy dolls may be inappropriate or less effective for those who have not previously cared for children or who may have experienced past birth trauma or the loss of a child.
Be guided by the person with dementia and how they respond to the doll.
Are there downsides?
The approach has attracted some controversy. It has been suggested that child representation therapy “infantilises” people living with dementia and may increase negative stigma.
Further, the attachment may become so strong that the person with dementia will become upset if someone else picks the doll up. This may create some difficulties in the presence of grandchildren or when cleaning the doll.
The introduction of child representation therapy may also require additional staff training and time. Non-pharmacological interventions such as child representation, however, have been shown to be cost-effective.
Could robots be the future?
The use of more interactive empathy dolls and pet-like robots is also gaining popularity.
While robots have been shown to be feasible and acceptable in dementia care, there remains some contention about their benefits.
While some studies have shown positive outcomes, including reduced agitation, others show no improvement in cognition, behaviour or quality of life among people with dementia.
Advances in artificial intelligence are also being used to help support people living with dementia and inform the community.
Viv and Friends, for example, are AI companions who appear on a screen and can interact with the person with dementia in real time. The AI character Viv has dementia and was co-created with women living with dementia using verbatim scripts of their words, insights and experiences. While Viv can share her experience of living with dementia, she can also be programmed to talk about common interests, such as gardening.
These companions are currently being trialled in some residential aged care facilities and to help educate people on the lived experience of dementia.
How should you respond to your loved one’s empathy doll?
While child representation can be a useful adjunct in dementia care, it requires sensitivity and appropriate consideration of the person’s needs.
People living with dementia may not perceive the social world the same way as a person without dementia. But a person living with dementia is not a child and should never be treated as one.
Ensure all family, friends and care workers are informed about the attachment to the empathy doll to help avoid unintentionally causing distress from inappropriate handling of the doll.
If using an interactive doll, ensure spare batteries are on hand.
Finally, it is important to reassess the attachment over time as the person’s response to the empathy doll may change.
Nikki-Anne Wilson, Postdoctoral Research Fellow, Neuroscience Research Australia (NeuRA), UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How Much Can Hypnotherapy Really Do?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sit Back, Relax, And…
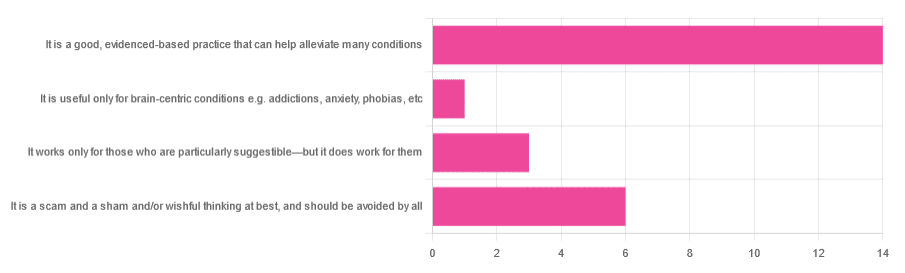
In Tuesday’s newsletter, we asked you for your opinions of hypnotherapy, and got the above-depicted, below-described, set of responses:
- About 58% said “It is a good, evidenced-based practice that can help alleviate many conditions”
- Exactly 25% said “It is a scam and sham and/or wishful thinking at best, and should be avoided by all”
- About 13% said “It works only for those who are particularly suggestible—but it does work for them”
- One (1) person said “It is useful only for brain-centric conditions e.g. addictions, anxiety, phobias, etc”
So what does the science say?
Hypnotherapy is all in the patient’s head: True or False?
True! But guess which part of your body controls much of the rest of it.
So while hypnotherapy may be “all in the head”, its effects are not.
Since placebo effect, nocebo effect, and psychosomatic effect in general are well-documented, it’s quite safe to say at the very least that hypnotherapy thus “may be useful”.
Which prompts the question…
Hypnotherapy is just placebo: True or False?
False, probably. At the very least, if it’s placebo, it’s an unusually effective placebo.
And yes, even though testing against placebo is considered a good method of doing randomized controlled trials, some placebos are definitely better than others. If a placebo starts giving results much better than other placebos, is it still a placebo? Possibly a philosophical question whose answer may be rooted in semantics, but happily we do have a more useful answer…
Here’s an interesting paper which: a) begins its abstract with the strong, unequivocal statement “Hypnosis has proven clinical utility”, and b) goes on to examine the changes in neural activity during hypnosis:
Brain Activity and Functional Connectivity Associated with Hypnosis
It works only for the very suggestible: True or False?
False, broadly. As with any medical and/or therapeutic procedure, a patient’s expectations can affect the treatment outcome.
And, especially worthy of note, a patient’s level of engagement will vastly affect it treatment that has patient involvement. So for example, if a doctor prescribes a patient pills, which the patient does not think will work, so the patient takes them intermittently, because they’re slow to get the prescription refilled, etc, then surprise, the pills won’t get as good results (since they’re often not being taken).
How this plays out in hypnotherapy: because hypnotherapy is a guided process, part of its efficacy relies on the patient following instructions. If the hypnotherapist guides the patient’s mind, and internally the patient is just going “nope nope nope, what a lot of rubbish” then of course it will not work, just like if you ask for directions in the street and then ignore them, you won’t get to where you want to be.
For those who didn’t click on the above link by the way, you might want to go back and have a look at it, because it included groups of individuals with “high/low hypnotizability” per several ways of scoring such.
It works only for brain-centric things, e.g. addictions, anxieties, phobias, etc: True or False?
False—but it is better at those. Here for example is the UK’s Royal College of Psychiatrists’ information page, and if you go to “What conditions can hypnotherapy help to treat”, you’ll see two broad categories; the first is almost entirely brain-stuff; the second is more varied, and includes pain relief of various kinds, burn care, cancer treatment side effects, and even menopause symptoms. Finally, warts and other various skin conditions get their own (positive) mention, per “this is possible through the positive effects hypnosis has on the immune system”:
RCPsych | Hypnosis And Hypnotherapy
Wondering how much psychosomatic effect can do?
You might like this previous article; it’s not about hypnotherapy, but it is about the difference the mind can make on physical markers of aging:
Aging, Counterclockwise: When Age Is A Flexible Number
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: