An Underrated Tool Against Alzheimer’s
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dementia in general, and Alzheimer’s in particular, affects a lot of people, and probably even more than the stats show, because some (estimated to be: about half) will go undiagnosed and thus unreported:
Alzheimer’s: The Bad News And The Good
At 10almonds, we often talk about brain health, whether from a nutrition standpoint or other lifestyle factors. For nutrition, by the way, check out:
Today we’ll be looking at some new science for an underrated tool:
Bilingualism as protective factor
It’s well-known that bilingualism offers brain benefits, but most people would be hard-pressed to name what, specifically, those brain benefits are.
As doctors Kristina Coulter and Natalie Phillips found in a recent study, one of the measurable benefits may be a defense against generalized (i.e. not necessarily language-related) memory loss Alzheimer’s disease.
Specifically,
❝We used surface-based morphometry methods to measure cortical thickness and volume of language-related and AD-related brain regions. We did not observe evidence of brain reserve in language-related regions.
However, reduced hippocampal volume was observed for monolingual, but not bilingual, older adults with AD. Thus, bilingualism is hypothesized to contribute to reserve in the form of brain maintenance in the context of AD.❞
Read in full: Bilinguals show evidence of brain maintenance in Alzheimer’s disease
This is important, because while language is processed in various parts of the brain beyond the scope of this article, the hippocampi* are where memory is stored.
*usually mentioned in the singular as “hippocampus”, but you have one on each side, unless some terrible accident or incident befell you.
What this means in practical terms: these results suggest that being bilingual means we will retain more of our capacity for memory, even if we get Alzheimer’s disease, than people who are monolingual.
Furthermore, while we’re talking practicality:
❝…our subsample may be characterized as mostly late bilinguals (i.e., learning an L2 after age 5), having moderate self-reported L2 ability, and relatively few participants reporting daily L2 use (33 out of 119)❞
(L2 = second language)
This is important, because it means you don’t have to have grown up speaking multiple languages, you don’t even have to speak it well, and you don’t have to be using your second language(s) on a daily basis, to enjoy benefits. Merely having them in your head appears to be sufficient to trigger the brain to go “oh, we need to boost and maintain the hippocampal volume”.
We would hypothesize that using second language(s) regularly and/or speaking second language(s) well offers additional protection, and the data would support this if it weren’t for the fact that the sample sizes for daily and high-level speakers are a bit small to draw conclusions.
But the important part is: simply knowing another language, including if you literally just learned it later in life, is already protective of hippocampal volume in the context of Alzheimer’s disease.
Here’s a pop-science article about the study, that goes into it in more detail than we have room to here:
Bilingualism linked to greater brain resilience in older adults
Want to learn a new language?
Here are some options where you can get going right away:
If you are thinking “sounds good, but learning a language is too much work”, then that is why we included that third option there. It’s specifically for one language, and that language is Esperanto, arguably the world’s easiest language and specifically designed to be super quick and easy to get good at. Also, it’s free!
Do, kial ne lerni novan lingvon rapide kaj facile? 😉
Want to know more?
For ways to reduce your overall Alzheimer’s risk according to science, check out:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Just One Heart – by Dr. Jonathan Fisher

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what this is not: a book to say eat fiber, go easy on the salt, get some exercise, and so forth.
What this rather is: a book about the connection between the heart and mind; often written poetically, the simple biological reality is that our emotional state does have a genuine impact on our heart health, and as such, any effort to look after our heart (healthwise) would be incomplete without an effort to look after our heart (emotionally).
Dr. Fisher talks about the impact of stress and uncertainty, as well as peace and security, on heart health—and then, having sorted emotional states into “heart breakers” and “heart wakers”, he goes about laying out a plan for what is, emotionally and thus also physiologically, good for our heart.
Chapter by chapter, he walks us through the 7 principles to live by:
- Steadiness: how to steady your heart amid chaos
- Wisdom: how to develop a wise heart in uncertain times
- Openness: how to safely open your heart in a threatening world
- Wholeness: how to show up with your whole heart without going to pieces
- Courage: how to lead with a courageous heart when fear surrounds you
- Lightness: how to live with a light heart in a heavy world
- Warmth: how to love with a warm heart when life feels cold
The style is anything but clinical; it’s well-written, certainly, and definitely informed in part by his medical understanding of the heart, but it’s entirely the raw human element that shines throughout, and that makes the ideas a lot more tangible.
Bottom line: if you’d like your heart to be healthy (cardiac health) and your heart to be healthy (emotional health), this book is a very worthwhile read.
Click here to check out Just One Heart, and take care of yours!
Share This Post
-

Is it OK to lie to someone with dementia?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There was disagreement on social media recently after a story was published about an aged care provider creating “fake-away” burgers that mimicked those from a fast-food chain, to a resident living with dementia. The man had such strict food preferences he was refusing to eat anything at meals except a burger from the franchise. This dementia symptom risks malnutrition and social isolation.
But critics of the fake burger approach labelled it trickery and deception of a vulnerable person with cognitive impairment.
Dementia is an illness that progressively robs us of memories. Although it has many forms, it is typical for short-term recall – the memory of something that happened in recent hours or days – to be lost first. As the illness progresses, people may come to increasingly “live in the past”, as distant recall gradually becomes the only memories accessible to the person. So a person in the middle or later stages of the disease may relate to the world as it once was, not how it is today.
This can make ethical care very challenging.

Pikselstock/Shutterstock Is it wrong to lie?
Ethical approaches classically hold that specific actions are moral certainties, regardless of the consequences. In line with this moral absolutism, it is always wrong to lie.
But this ethical approach would require an elderly woman with dementia who continually approaches care staff looking for their long-deceased spouse to be informed their husband has passed – the objective truth.
Distress is the likely outcome, possibly accompanied by behavioural disturbance that could endanger the person or others. The person’s memory has regressed to a point earlier in their life, when their partner was still alive. To inform such a person of the death of their spouse, however gently, is to traumatise them.
And with the memory of what they have just been told likely to quickly fade, and the questioning may resume soon after. If the truth is offered again, the cycle of re-traumatisation continues.
People with dementia may lose short term memories and rely on the past for a sense of the world. Bonsales/Shutterstock A different approach
Most laws are examples of absolutist ethics. One must obey the law at all times. Driving above the speed limit is likely to result in punishment regardless of whether one is in a hurry to pick their child up from kindergarten or not.
Pragmatic ethics rejects the notion certain acts are always morally right or wrong. Instead, acts are evaluated in terms of their “usefulness” and social benefit, humanity, compassion or intent.
The Aged Care Act is a set of laws intended to guide the actions of aged care providers. It says, for example, psychotropic drugs (medications that affect mind and mood) should be the “last resort” in managing the behaviours and psychological symptoms of dementia.
Instead, “best practice” involves preventing behaviour before it occurs. If one can reasonably foresee a caregiver action is likely to result in behavioural disturbance, it flies in the face of best practice.
What to say when you can’t avoid a lie?
What then, becomes the best response when approached by the lady looking for her husband?
Gentle inquiries may help uncover an underlying emotional need, and point caregivers in the right direction to meet that need. Perhaps she is feeling lonely or anxious and has become focused on her husband’s whereabouts? A skilled caregiver might tailor their response, connect with her, perhaps reminisce, and providing a sense of comfort in the process.
This approach aligns with Dementia Australia guidance that carers or loved ones can use four prompts in such scenarios:
- acknowledge concern (“I can tell you’d like him to be here.”)
- suggest an alternative (“He can’t visit right now.”)
- provide reassurance (“I’m here and lots of people care about you.”)
- redirect focus (“Perhaps a walk outside or a cup of tea?”)
These things may or may not work. So, in the face of repeated questions and escalating distress, a mistruth, such as “Don’t worry, he’ll be back soon,” may be the most humane response in the circumstances.
Different realities
It is often said you can never win an argument with a person living with dementia. A lot of time, different realities are being discussed.
So, providing someone who has dementia with a “pretend” burger may well satisfy their preferences, bring joy, mitigate the risk of malnutrition, improve social engagement, and prevent a behavioural disturbance without the use of medication. This seems like the correct approach in ethical terms. On occasion, the end justifies the means.
Steve Macfarlane, Head of Clinical Services, Dementia Support Australia, & Associate Professor of Psychiatry, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Ouch. That ‘Free’ Annual Checkup Might Cost You. Here’s Why.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When Kristy Uddin, 49, went in for her annual mammogram in Washington state last year, she assumed she would not incur a bill because the test is one of the many preventive measures guaranteed to be free to patients under the 2010 Affordable Care Act. The ACA’s provision made medical and economic sense, encouraging Americans to use screening tools that could nip medical problems in the bud and keep patients healthy.
So when a bill for $236 arrived, Uddin — an occupational therapist familiar with the health care industry’s workings — complained to her insurer and the hospital. She even requested an independent review.
“I’m like, ‘Tell me why am I getting this bill?’” Uddin recalled in an interview. The unsatisfying explanation: The mammogram itself was covered, per the ACA’s rules, but the fee for the equipment and the facility was not.
That answer was particularly galling, she said, because, a year earlier, her “free” mammogram at the same health system had generated a bill of about $1,000 for the radiologist’s reading. Though she fought that charge (and won), this time she threw in the towel and wrote the $236 check. But then she dashed off a submission to the KFF Health News-NPR “Bill of the Month” project:
“I was really mad — it’s ridiculous,” she later recalled. “This is not how the law is supposed to work.”
The ACA’s designers might have assumed that they had spelled out with sufficient clarity that millions of Americans would no longer have to pay for certain types of preventive care, including mammograms, colonoscopies, and recommended vaccines, in addition to doctor visits to screen for disease. But the law’s authors didn’t reckon with America’s ever-creative medical billing juggernaut.
Over the past several years, the medical industry has eroded the ACA’s guarantees, finding ways to bill patients in gray zones of the law. Patients going in for preventive care, expecting that it will be fully covered by insurance, are being blindsided by bills, big and small.
The problem comes down to deciding exactly what components of a medical encounter are covered by the ACA guarantee. For example, when do conversations between doctor and patient during an annual visit for preventive services veer into the treatment sphere? What screenings are needed for a patient’s annual visit?
A healthy 30-year-old visiting a primary care provider might get a few basic blood tests, while a 50-year-old who is overweight would merit additional screening for Type 2 diabetes.
Making matters more confusing, the annual checkup itself is guaranteed to be “no cost” for women and people age 65 and older, but the guarantee doesn’t apply for men in the 18-64 age range — though many preventive services that require a medical visit (such as checks of blood pressure or cholesterol and screens for substance abuse) are covered.
No wonder what’s covered under the umbrella of prevention can look very different to medical providers (trying to be thorough) and billers (intent on squeezing more dollars out of every medical encounter) than it does to insurers (who profit from narrower definitions).
For patients, the gray zone has become a billing minefield. Here are a few more examples, gleaned from the Bill of the Month project in just the past six months:
Peter Opaskar, 46, of Texas, went to his primary care doctor last year for his preventive care visit — as he’d done before, at no cost. This time, his insurer paid $130.81 for the visit, but he also received a perplexing bill for $111.81. Opaskar learned that he had incurred the additional charge because when his doctor asked if he had any health concerns, he mentioned that he was having digestive problems but had already made an appointment with his gastroenterologist. So, the office explained, his visit was billed as both a preventive physical and a consultation. “Next year,” Opasker said in an interview, if he’s asked about health concerns, “I’ll say ‘no,’ even if I have a gunshot wound.”
Kevin Lin, a technology specialist in Virginia in his 30s, went to a new primary care provider to take advantage of the preventive care benefit when he got insurance; he had no physical complaints. He said he was assured at check-in that he wouldn’t be charged. His insurer paid $174 for the checkup, but he was billed an additional $132.29 for a “new patient visit.” He said he has made many calls to fight the bill, so far with no luck.
Finally, there’s Yoori Lee, 46, of Minnesota, herself a colorectal surgeon, who was shocked when her first screening colonoscopy yielded a bill for $450 for a biopsy of a polyp — a bill she knew was illegal. Federal regulations issued in 2022 to clarify the matter are very clear that biopsies during screening colonoscopies are included in the no-cost promise. “I mean, the whole point of screening is to find things,” she said, stating, perhaps, the obvious.
Though these patient bills defy common sense, room for creative exploitation has been provided by the complex regulatory language surrounding the ACA. Consider this from Ellen Montz, deputy administrator and director of the Center for Consumer Information and Insurance Oversight at the Centers for Medicare & Medicaid Services, in an emailed response to queries and an interview request on this subject: “If a preventive service is not billed separately or is not tracked as individual encounter data separately from an office visit and the primary purpose of the office visit is not the delivery of the preventive item or service, then the plan issuer may impose cost sharing for the office visit.”
So, if the doctor decides that a patient’s mention of stomach pain does not fall under the umbrella of preventive care, then that aspect of the visit can be billed separately, and the patient must pay?
And then there’s this, also from Montz: “Whether a facility fee is permitted to be charged to a consumer would depend on whether the facility usage is an integral part of performing the mammogram or an integral part of any other preventive service that is required to be covered without cost sharing under federal law.”
But wait, how can you do a mammogram or colonoscopy without a facility?
Unfortunately, there is no federal enforcement mechanism to catch individual billing abuses. And agencies’ remedies are weak — simply directing insurers to reprocess claims or notifying patients they can resubmit them.
In the absence of stronger enforcement or remedies, CMS could likely curtail these practices and give patients the tools to fight back by offering the sort of clarity the agency provided a few years ago regarding polyp biopsies — spelling out more clearly what comes under the rubric of preventive care, what can be billed, and what cannot.
The stories KFF Health News and NPR receive are likely just the tip of an iceberg. And while each bill might be relatively small compared with the stunning $10,000 hospital bills that have become all too familiar in the United States, the sorry consequences are manifold. Patients pay bills they do not owe, depriving them of cash they could use elsewhere. If they can’t pay, those bills might end up with debt-collection agencies and, ultimately, harm their credit score.
Perhaps most disturbing: These unexpected bills might discourage people from seeking preventive screenings that could be lifesaving, which is why the ACA deemed them “essential health benefits” that should be free.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post



Related Posts
-

Aging Well: Exercise, Diet, Relationships
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Questions and Answers at 10almonds
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
This newsletter has been growing a lot lately, and so have the questions/requests, and we love that! In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
I am interested in the following: Aging, Exercise, Diet, Relationships, Purpose, Lowering Stress
You’re going to love our Psychology Sunday editions of 10almonds!
You may particularly like some of these:
- Seriously Useful Communication Skills! ← this is about relationship stuff
- Lower Your Cortisol! (Here’s Why & How) ← about “the stress hormone”
- How To Set Your Anxiety Aside ← these methods work for stress too
(This coming Psychology Sunday will have a feature specifically on stress, so do make sure to read that when it comes out!)
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Probiotics & Gas/Bloating
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝I read about probiotics and got myself some from amazon but having started them, now I have a lot of gas, is this normal?❞
As Tom Jones would say: it’s not unusual.
However, it’s also not necessary, and it is easy enough to get past!
And probiotics certainly have their place; see: How Much Difference Do Probiotic Supplements Make, Really?
What’s going on with your gas is…
We interrupt this article to bring back attention to our regular legal/medical disclaimer; please do remember that we can only speak in general health terms, cannot diagnose you, nor make any firm assurances about your health, nor prescribe treatment. What we can do is share information that we hope is educational, and if it helps you, so much the better. Always speak to your own doctor if you have concerns about your health.
Now, back to the article,,,
What’s going on with your gas is most probably what happens for a lot of people: you’ve just put a lot of bacteria into your gut, and congratulations, they survived (which is definitely not a given, more on that later, but their survival is what you wanted), and they are now thriving sufficiently that the output of their respiratory processes is tangible to you—in the form of abdominal bloating/gas.
Because your gut is a semi-closed system (literally there’s an opening at both ends, but it’s mostly quite self-contained in terms of its ecosystem, unless you have leaky gut syndrome, which is Very Bad™), this will generally fix itself within a few days at most—perhaps it even has by the time you’re reading this.
How does it fix itself you wonder? Because there’s only enough resources to sustain so many bacteria, what happens when we take a probiotic supplement (or food) is initially an overload of more bacteria than the gut can support (because unless you recently took antibiotics, the gut is pretty much always running at maximum capacity, because the bacteria there have no evolutionary reason to leave room for newcomers; they just multiply as best they can until the resources run out), and then the excess (i.e., those that are in excess of how many your gut can support) will die, and then the numbers will be back to normal.
Note: the numbers will be back to normal. However, that doesn’t mean the probiotics did nothing—what you’ve done is add diversity, and specifically, you’ve made it so that percentage-wise, you now have slightly more “good” bacteria in the balance than you did previously.
So, unless there are factors out of the ordinary: this is all usually self-correcting quite quickly.
Tips to make things go as smoothly as possible
Firstly, pay attention to recommended doses. If you take one, and think “that was delicious; I’ll have six more” then the initial effect will be a lot more than six times stronger, because of the nature of how bacteria multiply (i.e. exponentially) within minutes of reaching your gut.
Again, this will normally self-correct, but there’s no reason to cause yourself discomfort unnecessarily.
Secondly, if you take probiotics and do not get even a little gas or abdominal bloating even just a little bit, even just briefly… Then probably one of two things happened:
- The probiotics were dead on arrival (i.e. the supplement was a dud, or a “live culture” product in fact died before it got to you)
- The probiotics were fine, but your gut wasn’t prepared for them, and they died upon arrival
The latter happens a lot, especially if the current gut health is not good. What your probiotics need to survive (and bear in mind, because of their life cycle, they need this in minutes of arrival, which is their multiply-or-die-out window), is:
- Fiber, especially insoluble fiber
- In a place they can get at it (i.e. it was the most recent thing you ate, and is not several feet further down your intestines)
- Not too crowded with competitors (i.e. you just ate it, not last night)
Thus, it can be best to take probiotics on a mostly-empty stomach after enjoying a fibrous snack.
See also: What Do The Different Kinds Of Fiber Do? 30 Foods That Rank Highest
And for that matter: Stop Sabotaging Your Gut ← this covers some common probiotics mistakes/problems
If you’d rather take them on an entirely empty stomach, look for probiotic supplements that come with their own prebiotic fiber (usually inulin); these are often marketed as “symbiotics”.
We don’t sell them, but here’s an example product on Amazon for your convenience 😎
Another thing to bear in mind is that there is (unless your case is unusual) no reason to take the same kind of probiotic for more than one course (i.e. one container of however many servings it has). This is because one of two things will be the case:
- The probiotic worked, in which case, you now have thriving colonies of the bacterial species that that supplement provided
- The probiotic didn’t work, in which case, why buy that one again?
So, if supplementing with probiotics, it can be good to do so with new brand each time, with a gap in between each for your gut to get used to the new order of things.
Finally, if you’re making any drastic dietary change, likely this will result in similar gut disturbances.
In particular, if you are moving away from foods that feed C. albicans (the bad fungus that puts holes in your gut), then it will object strongly, cause you to crave sugar/flour/alcohol/etc, give you mood swings, and generally remind you that it has its roots firmly embedded in your nervous system. If that happens, don’t listen to it; it’s just its death throes and it’ll quieten down soon.
You can read more about that here:
Making Friends With Your Gut (You Can Thank Us Later)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What’s the difference between a heart attack and cardiac arrest? One’s about plumbing, the other wiring
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In July 2023, rising US basketball star Bronny James collapsed on the court during practice and was sent to hospital. The 18-year-old athlete, son of famous LA Lakers’ veteran LeBron James, had experienced a cardiac arrest.
Many media outlets incorrectly referred to the event as a “heart attack” or used the terms interchangeably.
A cardiac arrest and a heart attack are distinct yet overlapping concepts associated with the heart.
With some background in how the heart works, we can see how they differ and how they’re related.
Explode/Shutterstock Understanding the heart
The heart is a muscle that contracts to work as a pump. When it contracts it pushes blood – containing oxygen and nutrients – to all the tissues of our body.
For the heart muscle to work effectively as a pump, it needs to be fed its own blood supply, delivered by the coronary arteries. If these arteries are blocked, the heart muscle doesn’t get the blood it needs.
This can cause the heart muscle to become injured or die, and results in the heart not pumping properly.
Heart attack or cardiac arrest?
Simply put, a heart attack, technically known as a myocardial infarction, describes injury to, or death of, the heart muscle.
A cardiac arrest, sometimes called a sudden cardiac arrest, is when the heart stops beating, or put another way, stops working as an effective pump.
In other words, both relate to the heart not working as it should, but for different reasons. As we’ll see later, one can lead to the other.
Why do they happen? Who’s at risk?
Heart attacks typically result from blockages in the coronary arteries. Sometimes this is called coronary artery disease, but in Australia, we tend to refer to it as ischaemic heart disease.
The underlying cause in about 75% of people is a process called atherosclerosis. This is where fatty and fibrous tissue build up in the walls of the coronary arteries, forming a plaque. The plaque can block the blood vessel or, in some instances, lead to the formation of a blood clot.
Atherosclerosis is a long-term, stealthy process, with a number of risk factors that can sneak up on anyone. High blood pressure, high cholesterol, diet, diabetes, stress, and your genes have all been implicated in this plaque-building process.
Other causes of heart attacks include spasms of the coronary arteries (causing them to constrict), chest trauma, or anything else that reduces blood flow to the heart muscle.
Regardless of the cause, blocking or reducing the flow of blood through these pipes can result in the heart muscle not receiving enough oxygen and nutrients. So cells in the heart muscle can be injured or die.
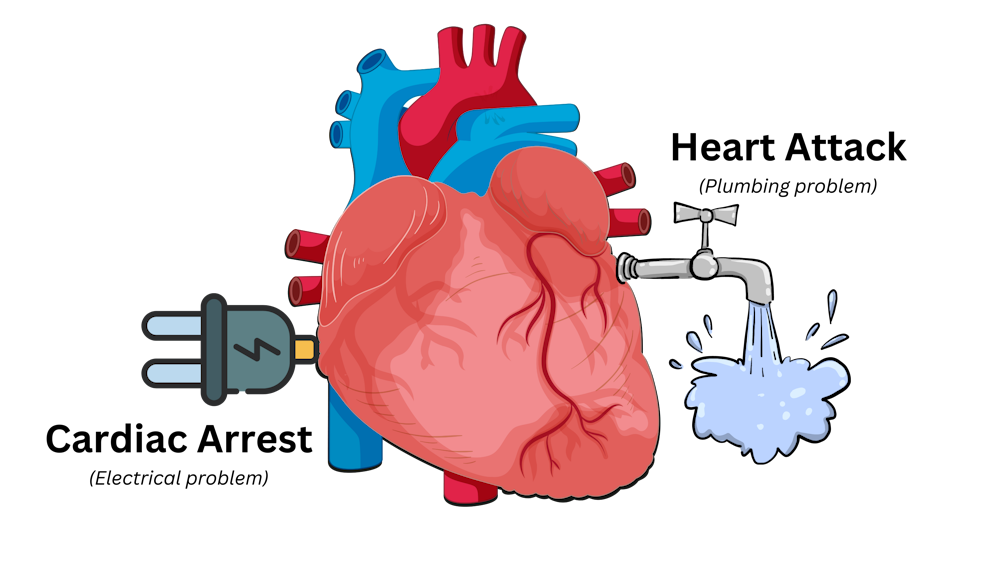
Here’s a simple way to remember the difference. Author provided But a cardiac arrest is the result of heartbeat irregularities, making it harder for the heart to pump blood effectively around the body. These heartbeat irregularities are generally due to electrical malfunctions in the heart. There are four distinct types:
- ventricular tachycardia: a rapid and abnormal heart rhythm in which the heartbeat is more than 100 beats per minute (normal adult, resting heart rate is generally 60-90 beats per minute). This fast heart rate prevents the heart from filling with blood and thus pumping adequately
- ventricular fibrillation: instead of regular beats, the heart quivers or “fibrillates”, resembling a bag of worms, resulting in an irregular heartbeat greater than 300 beats per minute
- pulseless electrical activity: arises when the heart muscle fails to generate sufficient pumping force after electrical stimulation, resulting in no pulse
- asystole: the classic flat-line heart rhythm you see in movies, indicating no electrical activity in the heart.
Remember this flat-line rhythm from the movies? It’s asystole, when there’s no electrical activity in the heart. Kateryna Kon/Shutterstock Cardiac arrest can arise from numerous underlying conditions, both heart-related and not, such as drowning, trauma, asphyxia, electrical shock and drug overdose. James’ cardiac arrest was attributed to a congenital heart defect, a heart condition he was born with.
But among the many causes of a cardiac arrest, ischaemic heart disease, such as a heart attack, stands out as the most common cause, accounting for 70% of all cases.
So how can a heart attack cause a cardiac arrest? You’ll remember that during a heart attack, heart muscle can be damaged or parts of it may die. This damaged or dead tissue can disrupt the heart’s ability to conduct electrical signals, increasing the risk of developing arrhythmias, possibly causing a cardiac arrest.
So while a heart attack is a common cause of cardiac arrest, a cardiac arrest generally does not cause a heart attack.
What do they look like?
Because a cardiac arrest results in the sudden loss of effective heart pumping, the most common signs and symptoms are a sudden loss of consciousness, absence of pulse or heartbeat, stopping of breathing, and pale or blue-tinged skin.
But the common signs and symptoms of a heart attack include chest pain or discomfort, which can show up in other regions of the body such as the arms, back, neck, jaw, or stomach. Also frequent are shortness of breath, nausea, light-headedness, looking pale, and sweating.
What’s the take-home message?
While both heart attack and cardiac arrest are disorders related to the heart, they differ in their mechanisms and outcomes.
A heart attack is like a blockage in the plumbing supplying water to a house. But a cardiac arrest is like an electrical malfunction in the house’s wiring.
Despite their different nature both conditions can have severe consequences and require immediate medical attention.
Michael Todorovic, Associate Professor of Medicine, Bond University and Matthew Barton, Senior lecturer, School of Nursing and Midwifery, Griffith University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: