Squat Variations for Painful Knees (No More Pain!)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Having bad knees can be a bit of a catch-22; you want to squat to make them stronger, but you can’t do that because your knees are not good. But, there are ways to do it!
Dr. Alyssa Kuhn, a doctor of physical therapy, advises:
Gently does it
Ten ways to choose from:
- Pool Squats: performed in a pool for joint-friendly support. Can use both hands, one hand, or no support. Focus on sitting back and standing up, aiming for 10–20 reps.
- Supported Squats: use a sink, rings, or handles for support. Stand a distance away and sit back while keeping your knees behind your heels. Perform 10–20 reps for 2–3 sets.
- Chair Loop Squats: use a resistance band around your knees while sitting on a chair. Press your knees outward as you stand and sit to strengthen hip and knee stability. Do 8–12 reps for 2–3 sets.
- Heel Elevated Squats: place your heels on dumbbells to shift emphasis to thighs and reduce knee strain. Ideal for stiff ankles or back tightness. Perform 10–15 reps for 2–3 sets.
- Sumo Squats: a wide stance squat, good for hip strength and reducing knee stress. Adjust your foot positioning for comfort. Perform 15–20 reps for 2–3 sets.
- Chair Squats: hold a weight close to your chest while sitting and standing from a chair. Can use kettlebells or dumbbells. Do 8–10 reps for 2–3 sets.
- Band Squats: use a resistance band secured behind your knees to provide support and encourage proper squat mechanics. Perform 5–12 reps for 2–3 sets.
- Modified Single Leg Squat: sit-to-stand using one leg with the other as a kickstand. Adjust your foot position for difficulty. Perform 8–12 reps per side for 2–3 sets.
- Weighted Squats: add weight using dumbbells or a barbell. Maintain an upright torso. Adjust the weight and reps based on difficulty, and do 5–10 reps for 2–4 sets.
- Split Squat: a stationary lunge, keeping your feet in place and lowering straight down. Focus on your front leg while keeping balance. Can add weight if you want. Perform 5–12 reps per side based on difficulty.
For more on each of these plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How they did it: STAT reporters expose how ailing seniors suffer when Medicare Advantage plans use algorithms to deny care

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In a call with a long-time source, what stood out most to STAT reporters Bob Herman and Casey Ross was just how viscerally frustrated and angry the source was about an algorithm used by insurance companies to decide how long patients should stay in a nursing home or rehab facility before being sent home.
The STAT stories had a far-reaching impact:
- The U.S. Senate Committee on Homeland Security and Government Affairs took a rare step of launching a formal investigation into the use of algorithms by the country’s three largest Medicare Advantage insurers.
- Thirty-two House members urged the Centers for Medicare and Medicaid Services to increase the oversight of algorithms that health insurers use to make coverage decisions.
- In a rare step, CMS launched its own investigation into UnitedHealth. It also stiffened its regulations on the use of proprietary algorithms and introduced plans to audit denials across Medicare Advantage plans in 2024.
- Based on STAT’s reporting, Medicare Advantage beneficiaries filed two class-action lawsuits against UnitedHealth and its NaviHealth subsidiary, the maker of the algorithm, and against Humana, another major health insurance company that was also using the algorithm.
- Amid scrutiny, UnitedHealth renamed NaviHealth.
The companies never allowed an on-the-record interview with their executives, but they acknowledged that STAT’s reporting was true, according to the news organization.
Ross and Herman spoke with The Journalist’s Resource about their project and shared the following eight tips.
1. Search public comments on proposed federal rules to find sources.
Herman and Ross knew that the Centers for Medicare and Medicaid Services had put out a request for public comments, asking stakeholders within the Medicare Advantage industry how the system could improve.
There are two main ways to get Medicare coverage: original Medicare, which is a fee-for-service health plan, and Medicare Advantage, which is a type of Medicare health plan offered by private insurance companies that contract with Medicare. Medicare Advantage plans have increasingly become popular in recent years.
Under the Social Security Act, the public has the opportunity to submit comments on Medicare’s proposed national coverage determinations. CMS uses public comments to inform its proposed and final decisions. It responds in detail to all public comments when issuing a final decision.
The reporters began combing through hundreds of public comments attached to a proposed Medicare Advantage rule that was undergoing federal review. NaviHealth, the UnitedHealth subsidiary and the maker of the algorithm, came up in many of the comments, which include the submitters’ information.
“These are screaming all-caps comments to federal regulators about YOU NEED TO SOMETHING ABOUT THIS BECAUSE IT’S DISGUSTING,” Ross says.
“The federal government is proposing rules and regulations all the time,” adds Herman, STAT’s business of health care reporter. “If someone’s going to take the time and effort to comment on them, they must have at least some knowledge of what’s going on. It’s just a great tool for any journalist to use to figure out more and who to contact.”
The reporters also found several attorneys who had complained in the comments. They began reaching out to them, eventually gaining access to confidential documents and intermediaries who put them in touch with patients to show the human impact of the algorithm.
2. Harness the power of the reader submission box.
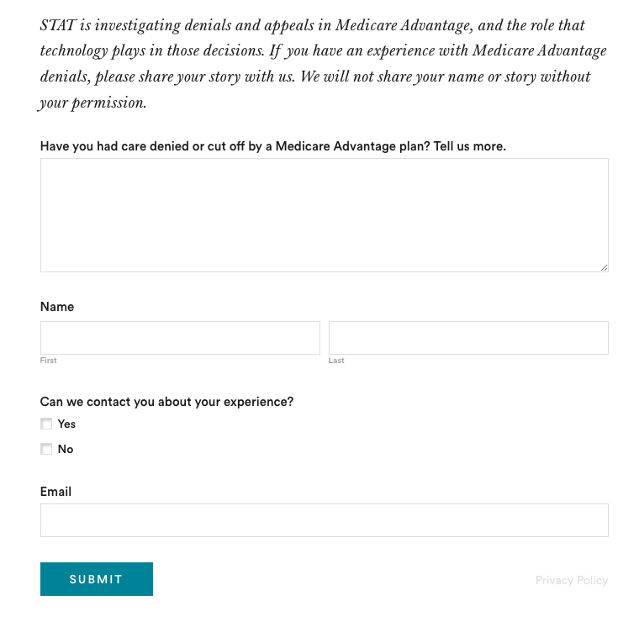
At the suggestion of an editor, the reporters added a reader submission box at the bottom of their first story, asking them to share their own experiences with Medicare Advantage denials.
The floodgates opened. Hundreds of submissions arrived.
By the end of their first story, Herman and Ross had confidential records and some patients, but they had no internal sources in the companies they were investigating, including Navihealth. The submission box led them to their first internal source.

(Screenshot of STAT’s submission box.) The journalists also combed through LinkedIn and reached out to former and current employees, but the response rate was much lower than what they received via the submission box.
The submission box “is just right there,” Herman says. “People who would want to reach out to us can do it right then and there after they read the story and it’s fresh in their minds.”
3. Mine podcasts relevant to your story.
The reporters weren’t sure if they could get interviews with some of the key figures in the story, including Tom Scully, the former head of the Centers for Medicare and Medicaid Services who drew up the initial plans for NaviHealth years before UnitedHealth acquired it.
But Herman and another colleague had written previously about Scully’s private equity firm and they had found a podcast where he talked about his work. So Herman went back to the podcast — where he discovered Scully had also discussed NaviHealth.
The reporters also used the podcast to get Scully on the phone for an interview.
“So we knew we had a good jumping off point there to be like, ‘OK, you’ve talked about NaviHealth on a podcast, let’s talk about this,’” Herman says. “I think that helped make him more willing to speak with us.”
4. When covering AI initiatives, proceed with caution.
“A source of mine once said to me, ‘AI is not magic,’” Ross says. “People need to just ask questions about it because AI has this aura about it that it’s objective, that it’s accurate, that it’s unquestionable, that it never fails. And that is not true.”
AI is not a neutral, objective machine, Ross says. “It’s based on data that’s fed into it and people need to ask questions about that data.”
He suggests several questions to ask about the data behind AI tools:
- Where does the data come from?
- Who does it represent?
- How is this tool being applied?
- Do the people to whom the tool is being applied match the data on which it was trained? “If racial groups or genders or age of economic situations are not adequately represented in the training set, then there can be an awful lot of bias in the output of the tool and how it’s applied,” Ross says.
- How is the tool applied within the institution? Are people being forced to forsake their judgment and their own ability to do their jobs to follow the algorithm?
5. Localize the story.
More than half of all Medicare beneficiaries have Medicare Advantage and there’s a high likelihood that there are multiple Medicare Advantage plans in every county across the nation.
“So it’s worth looking to see how Medicare Advantage plans are growing in your area,” Herman says.
Finding out about AI use will most likely rely on shoe-leather reporting of speaking with providers, nursing homes and rehab facilities, attorneys and patients in your community, he says. Another source is home health agencies, which may be caring for patients who were kicked out of nursing homes and rehab facilities too soon because of a decision by an algorithm.
The anecdote that opens their first story involves a small regional health insurer in Wisconsin, which was using NaviHealth and a contractor to manage post-acute care services, Ross says.
“It’s happening to people in small communities who have no idea that this insurer they’ve signed up with is using this tool made by this other company that operates nationally,” Ross says.
There are also plenty of other companies like NaviHealth that are being used by Medicare Advantage plans, Herman says. “So it’s understanding which Medicare Advantage plans are being sold in your area and then which post-acute management companies they’re using,” he adds.
Some regional insurers have online documents that show which contractors they use to evaluate post-acute care services.
6. Get familiar with Medicare’s appeals databases
Medicare beneficiaries can contest Medicare Advantage denials through a five-stage process, which can last months to years. The appeals can be filed via the Office of Medicare Hearings and Appeals.
“Between 2020 and 2022, the number of appeals filed to contest Medicare Advantage denials shot up 58%, with nearly 150,000 requests to review a denial filed in 2022, according to a federal database,” Ross and Herman write in their first story. “Federal records show most denials for skilled nursing care are eventually overturned, either by the plan itself or an independent body that adjudicates Medicare appeals.”
There are several sources to find appeals data. Be mindful that the cases themselves are not public to protect patient privacy, but you can find the number of appeals filed and the rationale for decisions.
CMS has two quality improvement organizations, or QIOs, Livanta and Kepro, which are required to file free, publicly-available annual reports, about the cases they handle, Ross says.
Another company, Maximus, a Quality Improvement Contractor, also files reports on prior authorization cases it adjudicates for Medicare. The free annual reports include data on raw numbers of cases and basic information about the percentage denials either overturned or upheld on appeal, Ross explains.
CMS also maintains its own database on appeals for Medicare Part C (Medicare Advantage plans) and Part D, which covers prescription drugs, although the data is not complete, Ross explains.
7. Give your editor regular updates.
“Sprinkle the breadcrumbs in front of your editors,” Ross says.
“If you wrap your editors in the process, you’re more likely to be able to get to the end of [the story] before they say, ‘That’s it! Give me your copy,’” Ross says.
8. Get that first story out.
“You don’t have to know everything before you write that first story,” Ross says. “Because with that first story, if it has credibility and it resonates with people, sources will come forward and sources will continue to come forward.”
Read the stories
Denied by AI: How Medicare Advantage plans use algorithms to cut off care for seniors in need
UnitedHealth pushed employees to follow an algorithm to cut off Medicare patients’ rehab care
UnitedHealth used secret rules to restrict rehab care for seriously ill Medicare Advantage patients
This article first appeared on The Journalist’s Resource and is republished here under a Creative Commons license.
Share This Post
-

We looked at 700 plant-based foods to see how healthy they really are. Here’s what we found
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you’re thinking about buying plant-based foods, a trip to the supermarket can leave you bewildered.
There are plant-based burgers, sausages and mince. The fridges are loaded with non-dairy milk, cheese and yoghurt. Then there are the tins of beans and packets of tofu.
But how much is actually healthy?
Our nutritional audit of more than 700 plant-based foods for sale in Australian supermarkets has just been published. We found some products are so high in salt or saturated fat, we’d struggle to call them “healthy”.
We took (several) trips to the supermarket
In 2022, we visited two of each of four major supermarket retailers across Melbourne to collect information on the available range of plant-based alternatives to meat and dairy products.
We took pictures of the products and their nutrition labels.
We then analysed the nutrition information on the packaging of more than 700 of these products. This included 236 meat substitutes, 169 legumes and pulses, 50 baked beans, 157 dairy milk substitutes, 52 cheese substitutes and 40 non-dairy yoghurts.
Plant-based meats were surprisingly salty
We found a wide range of plant-based meats for sale. So, it’s not surprising we found large variations in their nutrition content.
Sodium, found in added salt and which contributes to high blood pressure, was our greatest concern.
The sodium content varied from 1 milligram per 100 grams in products such as tofu, to 2,000mg per 100g in items such as plant-based mince products.
This means we could eat our entire daily recommended sodium intake in just one bowl of plant-based mince.
An audit of 66 plant-based meat products in Australian supermarkets conducted in 2014 found sodium ranged from 316mg in legume-based products to 640mg in tofu products, per 100g. In a 2019 audit of 137 products, the range was up to 1,200mg per 100g.
In other words, the results of our audit seems to show a consistent trend of plant-based meats getting saltier.
Looking for plant-based meat? Check the label for the sodium content.
Michael Vi/Shutterstock
What about plant-based milks?
Some 70% of the plant-based milks we audited were fortified with calcium, a nutrient important for bone health.
This is good news as a 2019-2020 audit of 115 plant-based milks from Melbourne and Sydney found only 43% of plant-based milks were fortified with calcium.
Of the fortified milks in our audit, almost three-quarters (73%) contained the recommended amount of calcium – at least 100mg per 100mL.
We also looked at the saturated fat content of plant-based milks.
Coconut-based milks had on average up to six times higher saturated fat content than almond, oat or soy milks.
Previous audits also found coconut-based milks were much higher in saturated fat than all other categories of milks.
Some plant-based milks were healthier than others.
TY Lim/Shutterstock
A first look at cheese and yoghurt alternatives
Our audit is the first study to identify the range of cheese and yoghurt alternatives available in Australian supermarkets.
Calcium was only labelled on a third of plant-based yoghurts, and only 20% of supermarket options met the recommended 100mg of calcium per 100g.
For plant-based cheeses, most (92%) were not fortified with calcium. Their sodium content varied from 390mg to 1,400mg per 100g, and saturated fat ranged from 0g to 28g per 100g.
So, what should we consider when shopping?
As a general principle, try to choose whole plant foods, such as unprocessed legumes, beans or tofu. These foods are packed with vitamins and minerals. They’re also high in dietary fibre, which is good for your gut health and keeps you fuller for longer.
If opting for a processed plant-based food, here are five tips for choosing a healthier option.
1. Watch the sodium
Plant-based meat alternatives can be high in sodium, so look for products that have around 150-250mg sodium per 100g.
2. Pick canned beans and legumes
Canned chickpeas, lentils and beans can be healthy and low-cost additions to many meals. Where you can, choose canned varieties with no added salt, especially when buying baked beans.
3. Add herbs and spices to your tofu
Tofu can be a great alternative to meat. Check the label and pick the option with the highest calcium content. We found flavoured tofu was higher in salt and sugar content than minimally processed tofu. So it’s best to pick an unflavoured option and add your own flavours with spices and herbs.
4. Check the calcium
When choosing a non-dairy alternative to milk, such as those made from soy, oat, or rice, check it is fortified with calcium. A good alternative to traditional dairy will have at least 100mg of calcium per 100g.
5. Watch for saturated fat
If looking for a lower saturated fat option, almond, soy, rice and oat varieties of milk and yoghurt alternatives have much lower saturated fat content than coconut options. Pick those with less than 3g per 100g.

Laura Marchese, PhD Student at the Institute for Physical Activity and Nutrition, Deakin University and Katherine Livingstone, NHMRC Emerging Leadership Fellow and Senior Research Fellow at the Institute for Physical Activity and Nutrition, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

The Sun Exposure Dilemma
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Sun Exposure Dilemma

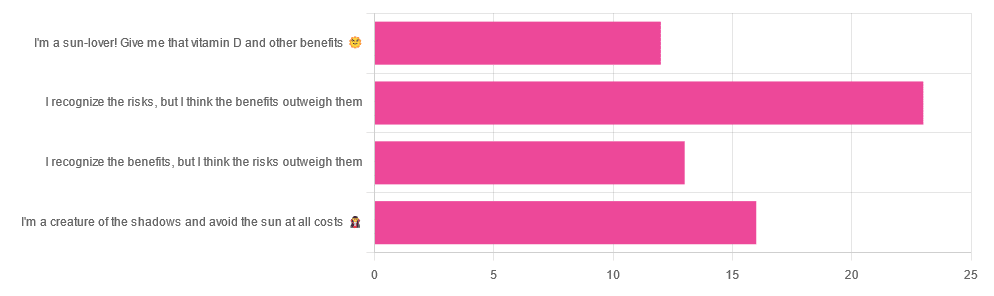
Yesterday, we asked you about your policy on sun exposure, and got the above-pictured, below-described, set of answers:
- A little over a third of respondents chose “I recognize the risks, but I think the benefits outweigh them”
- A quarter of respondents chose “I am a creature of the shadows and I avoid the sun at all costs”
- A little over a fifth of respondents chose “I recognize the benefits, but I think the risks outweigh them”
- A little under a fifth of respondents chose “I’m a sun-lover! Give me that vitamin D and other benefits!”
All in all, this is perhaps the most even spread of answers we’ve had for Friday mythbuster polls—though the sample size was smaller than it often is.
Of those who added comments, common themes were to mention your local climate, and the importance of sunscreen and/or taking vitamin D supplements.
One subscriber mentioned having lupus and living in Florida, which is a particularly unfortunate combination:
Lupus Foundation | Lupus & UV exposure: What you need to know
Another subscriber wrote:
❝Use a very good sunscreen with a high SPF all the time. Reapply after swimming or as needed! I also wear polarized sunglasses anytime I’m outside.❞
…which are important things to note too, and a lot of people forget!
See also: Who Screens The Sunscreens? (on fearing chemical dangers, vs the protection given)
But, onto today’s science for the topic at hand…
We need to get plenty of sun to get plenty of vitamin D: True or False?
True or False, depending on so many factors—to the point that many people get it wildly wrong in either direction.
Whether we are getting enough vitamin D depends on many circumstances, including:
- The climate (and depending on latitude, time of year) where we live
- Our genes, and especially (but not only) our skintone
- The clothes we wear (or don’t)
- Our diet (and not just “how much vitamin D do we consume”)
- Chronic diseases that affect vitamin D metabolism and/or requirements and/or sensitivity to the sun
For a rundown on these factors and more, check out:
Should I be getting my vitamin D levels checked?
Notably, on the topic of whether you should stay in the sun for longer to get more vitamin D…
❝The body can only produce a certain amount of vitamin D at the time, so staying in the sun any longer than needed (which could be just a few minutes, in a sunny climate) is not going to help increase your vitamin D levels, while it will increase your risk of skin cancer.❞
In contrast, she does also note:
❝During winter, catching enough sun can be difficult, especially if you spend your days confined indoors. Typically, the required exposure increases to two to three hours per week in winter. This is because sunlight exposure can only help produce vitamin D if the UVB rays reach us at the correct angle. So in winter we should regularly spend time outside in the middle of the day to get our dose of vitamin D.❞
See also: Vitamin D & Calcium: Too Much Of A Good Thing?
We can skip the sun and get our vitamin D from diet/supplements: True or False?
True! However, vitamin D is not the only health benefit of sun exposure.
Not only is sunlight-induced serotonin production important for many things ranging from mood to circadian rhythm (which in turn affects many other aspects of health), but also…
While too much sun can cause skin cancer, too little sun could cause other kinds of cancer:
Benefits of Sunlight: A Bright Spot for Human Health
Additionally, according to new research, the circadian rhythm benefits we mentioned above may also have an impact on type 2 diabetes:
Can catching some rays help you fight off type 2 diabetes?
Which way to jump?
A lot of it depends on who you are, ranging from the factors we mentioned earlier, to even such things as “having many moles” or “having blonde hair”.
This latter item, blonde hair, is a dual thing: it’s a matter of genetic factors that align with being prone to being more sensitive to the sun, as well as being a lesser physical barrier to the sun’s rays than dark hair (that can block some UV rays).
So for example, if two people have comparably gray hair now, but one of them used to have dark hair and the other blonde, there will still be a difference in how they suffer damage, or don’t—and yes, even if their skin is visually of the same approximate skintone.
You probably already know for yourself whether you are more likely to burn or tan in the sun, and the former group are less resistant to the sun’s damage… But the latter group are more likely to spend longer in the sun, and accumulate more damage that way.
If you’d like a very comprehensive downloadable, here are the guidelines issued by the UK’s National Institute for Health and Care Excellence:
NICE Guidelines | Sunlight exposure: risks and benefits
…and skip to “At risk groups”, if you don’t want to read the whole thing; “Skin type” is also an important subsection, which also uses your hair and eye color as indicators.
Writer’s note: genetics are complicated and not everyone will fall neatly into categories, which is why it’s important to know the individual factors.
For example, I am quite light-skinned with slightly graying dark hair and gray-blue eyes, and/but also have an obscure Sámi gene that means my skin makes vitamin D easily, while simultaneously being unusually resistant to burning (I just tan). Basically: built for the midnight sun of the Arctic circle.
And yet! My hobbies include not getting skin cancer, so I tend to still be quite mindful of UV levels in different weathers and times of day, and make choices (schedule, clothing, sunscreen or not) accordingly.
Bottom line:
That big self-perpetuating nuclear explosion in the sky is responsible for many things, good and bad for our health, so be aware of your own risk factors, especially for vitamin D deficiency, and skin cancer.
- If you have a predisposition to both, that’s unfortunate, but diet and supplementation at least can help with the vitamin D while getting modest amounts of sun at most.
- Remember that you can only make so much vitamin D at once, so sunbathing for health benefits need only take a few minutes
- Remember that sunlight is important for our circadian rhythm, which is important for many things.
- That’s governed by specific photoreceptor cells, though, so we don’t need our skin to be exposed for that; we just need to be able to see sunlight.
- If you’re going to be out in the sun, and not covered up, sunscreen is your friend, and yes, that goes for clear cold days under the winter sun too.
- Most phone weather apps these days have a UV index score as part of the data they give. Get used to checking it as often as you’d check for rain.
Stay safe, both ways around!
Share This Post




Related Posts
-

What is ‘doll therapy’ for people with dementia? And is it backed by science?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The way people living with dementia experience the world can change as the disease progresses. Their sense of reality or place in time can become distorted, which can cause agitation and distress.
One of the best ways to support people experiencing changes in perception and behaviour is to manage their environment. This can have profound benefits including reducing the need for sedatives.
One such strategy is the use of dolls as comfort aids.
Jack Cronkhite/Shutterstock What is ‘doll therapy’?
More appropriately referred to as “child representation”, lifelike dolls (also known as empathy dolls) can provide comfort for some people with dementia.
Memories from the distant past are often more salient than more recent events in dementia. This means that past experiences of parenthood and caring for young children may feel more “real” to a person with dementia than where they are now.
Hallucinations or delusions may also occur, where a person hears a baby crying or fears they have lost their baby.
Providing a doll can be a tangible way of reducing distress without invalidating the experience of the person with dementia.
Some people believe the doll is real
A recent case involving an aged care nurse mistreating a dementia patient’s therapy doll highlights the importance of appropriate training and support for care workers in this area.
For those who do become attached to a therapeutic doll, they will treat the doll as a real baby needing care and may therefore have a profound emotional response if the doll is mishandled.
It’s important to be guided by the person with dementia and only act as if it’s a real baby if the person themselves believes that is the case.
What does the evidence say about their use?
Evidence shows the use of empathy dolls may help reduce agitation and anxiety and improve overall quality of life in people living with dementia.
Child representation therapy falls under the banner of non-pharmacological approaches to dementia care. More specifically, the attachment to the doll may act as a form of reminiscence therapy, which involves using prompts to reconnect with past experiences.
Interacting with the dolls may also act as a form of sensory stimulation, where the person with dementia may gain comfort from touching and holding the doll. Sensory stimulation may support emotional well-being and aid commnication.
However, not all people living with dementia will respond to an empathy doll.
It depends on a person’s background. Shutterstock The introduction of a therapeutic doll needs to be done in conjunction with careful observation and consideration of the person’s background.
Empathy dolls may be inappropriate or less effective for those who have not previously cared for children or who may have experienced past birth trauma or the loss of a child.
Be guided by the person with dementia and how they respond to the doll.
Are there downsides?
The approach has attracted some controversy. It has been suggested that child representation therapy “infantilises” people living with dementia and may increase negative stigma.
Further, the attachment may become so strong that the person with dementia will become upset if someone else picks the doll up. This may create some difficulties in the presence of grandchildren or when cleaning the doll.
The introduction of child representation therapy may also require additional staff training and time. Non-pharmacological interventions such as child representation, however, have been shown to be cost-effective.
Could robots be the future?
The use of more interactive empathy dolls and pet-like robots is also gaining popularity.
While robots have been shown to be feasible and acceptable in dementia care, there remains some contention about their benefits.
While some studies have shown positive outcomes, including reduced agitation, others show no improvement in cognition, behaviour or quality of life among people with dementia.
Advances in artificial intelligence are also being used to help support people living with dementia and inform the community.
Viv and Friends, for example, are AI companions who appear on a screen and can interact with the person with dementia in real time. The AI character Viv has dementia and was co-created with women living with dementia using verbatim scripts of their words, insights and experiences. While Viv can share her experience of living with dementia, she can also be programmed to talk about common interests, such as gardening.
These companions are currently being trialled in some residential aged care facilities and to help educate people on the lived experience of dementia.
How should you respond to your loved one’s empathy doll?
While child representation can be a useful adjunct in dementia care, it requires sensitivity and appropriate consideration of the person’s needs.
People living with dementia may not perceive the social world the same way as a person without dementia. But a person living with dementia is not a child and should never be treated as one.
Ensure all family, friends and care workers are informed about the attachment to the empathy doll to help avoid unintentionally causing distress from inappropriate handling of the doll.
If using an interactive doll, ensure spare batteries are on hand.
Finally, it is important to reassess the attachment over time as the person’s response to the empathy doll may change.
Nikki-Anne Wilson, Postdoctoral Research Fellow, Neuroscience Research Australia (NeuRA), UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Do You Believe In Magic? – by Dr. Paul Offit
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Here at 10almonds, we like to examine and present the science wherever it leads, so this book was an interesting read.
Dr. Offit, himself a much-decorated vaccine research scientist, and longtime enemy of the anti-vax crowd, takes aim at alternative therapies in general, looking at what does work (and how), and what doesn’t (and what harm it can cause).
The style of the book is largely polemic in tone, but there’s lots of well-qualified information and stats in here too. And certainly, if there are alternative therapies you’ve left unquestioned, this book will probably prompt questions, at the very least.
And science, of course, is about asking questions, and shouldn’t be afraid of such! Open-minded skepticism is a key starting point, while being unafraid to actually reach a conclusion of “this is probably [not] so”, when and if that’s where the evidence brings us. Then, question again when and if new evidence comes along.
To that end, Dr. Offit does an enthusiastic job of looking for answers, and presenting what he finds.
If the book has downsides, they are primarily twofold:
- He is a little quick to dismiss the benefits of a good healthy diet, supplemented or otherwise.
- His keenness here seems to step from a desire to ensure people don’t skip life-saving medical treatments in the hope that their diet will cure their cancer (or liver disease, or be it what it may), but in doing so, he throws out a lot of actually good science.
- He—strangely—lumps menopausal HRT in with alternative therapies, and does the exact same kind of anti-science scaremongering that he rails against in the rest of the book.
- In his defence, this book was published ten years ago, and he may have been influenced by a stack of headlines at the time, and a popular celebrity endorsement of HRT, which likely put him off it.
Bottom line: there’s something here to annoy everyone—which makes for stimulating reading.
Click here to check out Do You Believe In Magic, and expand your knowledge!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- He is a little quick to dismiss the benefits of a good healthy diet, supplemented or otherwise.
-

Coenzyme Q10 From Foods & Supplements
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Coenzyme Q10 and the difference it makes
Coenzyme Q10, often abbreviated to CoQ10, is a popular supplement, and is often one of the more expensive supplements that’s commonly found on supermarket shelves as opposed to having to go to more specialist stores or looking online.
What is it?
It’s a compound naturally made in the human body and stored in mitochondria. Now, everyone remembers the main job of mitochondria (producing energy), but they also protect cells from oxidative stress, among other things. In other words, aging.
Like many things, CoQ10 production slows as we age. So after a certain age, often around 45 but lifestyle factors can push it either way, it can start to make sense to supplement.
Does it work?
The short answer is “yes”, though we’ll do a quick breakdown of some main benefits, and studies for such, before moving on.
First, do bear in mind that CoQ10 comes in two main forms, ubiquinol and ubiquinone.
Ubiquinol is much more easily-used by the body, so that’s the one you want. Here be science:
What is it good for?
Benefits include:
- Against aging
- Against skin cancer
- Against breast cancer
- Against prostate cancer
- Against heart failure
- Against obesity
- Against diabetes
- Against Alzheimer’s
- Against Parkinson’s
Can we get it from foods?
Yes, and it’s equally well-absorbed through foods or supplementation, so feel free to go with whichever is more convenient for you.
Read: Intestinal absorption of coenzyme Q10 administered in a meal or as capsules to healthy subjects
If you do want to get it from food, you can get it from many places:
- Organ meats: the top source, though many don’t want to eat them, either because they don’t like them or some of us just don’t eat meat. If you do, though, top choices include the heart, liver, and kidneys.
- Fatty fish: sardines are up top, along with mackerel, herring, and trout
- Vegetables: leafy greens, and cruciferous vegetables e.g. cauliflower, broccoli, sprouts
- Legumes: for example soy, lentils, peanuts
- Nuts and seeds: pistachios come up top; sesame seeds are great too
- Fruit: strawberries come up top; oranges are great too
If supplementing, how much is good?
Most studies have used doses in the 100mg–200mg (per day) range.
However, it’s also been found to be safe at 1200mg (per day), for example in this high-quality study that found that higher doses resulted in greater benefit, in patients with early Parkinson’s Disease:
Effects of coenzyme Q10 in early Parkinson disease: evidence of slowing of the functional decline
Wondering where you can get it?
We don’t sell it (or anything else for that matter), and you can probably find it in your local supermarket or health food store. However, if you’d like to buy it online, here’s an example product on Amazon
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: