High-Protein Plant-Based Diet for Beginners – by Maya Howard with Ariel Warren
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Seasoned vegans (well-seasoned vegans?) will know that getting enough protein from a plant-based diet is really not the challenge that many think it is, but for those just embarking on cutting out the meat, it’s not useful to say “it’s easy!”; it’s useful to show how.
That’s what this book does. And not just by saying “these foods” and leaving people to wonder if they need to eat a pound of tofu each day to get their protein in. Instead, recipes. Enough for a 4-week meal plan, and the idea is that after a month of eating that way, it won’t be nearly so mysterious.
The recipes are very easy to execute, while still having plenty of flavor (which is what happens when one uses a lot of flavorsome main ingredients and then seasons them well too). The ingredients are not obscure, and you should be able to find everything easily in any medium-sized supermarket.
As for the well-roundedness of the diet, we’ll mention that the “with Ariel Warren” in the by-line means that while the book was principally authored by Maya Howard (who is, at time of writing, a nutritionist-in-training), she had input throughout from Ariel Warren (a Registered Dietician Nutritionist) to ensure she didn’t go off-piste anyway and it gets the professional stamp of approval.
Bottom line: if you’d like to cook plant based while still prioritizing protein and you’re not sure how to make that exciting and fun instead of a chore, then this book will show you how to please your taste buds and improve your body composition at the same time.
Click here to check out High-Protein Plant-Based Diet for Beginners, and dig in!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Antidepressants: Personalization Is Key!

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Antidepressants: Personalization Is Key!

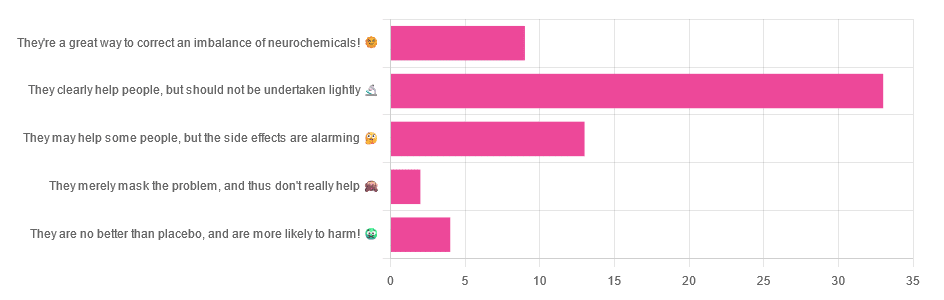
Yesterday, we asked you for your opinions on antidepressants, and got the above-depicted, below-described, set of responses:
- Just over half of respondents said “They clearly help people, but should not be undertaken lightly”
- Just over a fifth of respondents said “They may help some people, but the side effects are alarming”
- Just under a sixth of respondents said “They’re a great way to correct an imbalance of neurochemicals”
- Four respondents said “They are no better than placebo, and are more likely to harm”
- Two respondents said “They merely mask the problem, and thus don’t really help”
So what does the science say?
❝They are no better than placebo, and are more likely to harm? True or False?❞
True or False depending on who you are and what you’re taking. Different antidepressants can work on many different systems with different mechanisms of action. This means if and only if you’re not taking the “right” antidepressant for you, then yes, you will get only placebo benefits:
- Placebo Effect in the Treatment of Depression and Anxiety ← randomly assigned antidepressants are, shockingly, luck of the draw in usefulness
- Antidepressants versus placebo in major depression: an overview ← “wow this science is messy”
- Comparative efficacy and acceptability of 21 antidepressant drugs: a systematic review and network meta-analysis ← “oh look, it makes a difference which antidepressant we give to people”
Rather than dismissing antidepressants as worthless, therefore, it is a good idea to find out (by examination or trial and error) what kind of antidepressant you need, if you indeed do need such.
Otherwise it is like getting a flu shot and being surprised when you still catch a cold!
❝They merely mask the problem, and thus don’t really help: True or False?❞
False, categorically.
The problem in depressed people is the depressed mood. This may be influenced by other factors, and antidepressants indeed won’t help directly with those, but they can enable the person to better tackle them (more on this later).
❝They may help some people, but the side-effects are alarming: True or False?❞
True or False depending on more factors than we can cover here.
Side-effects vary from drug to drug and person to person, of course. As does tolerability and acceptability, since to some extent these things are subjective.
One person’s dealbreaker may be another person’s shrugworthy minor inconvenience at most.
❝They’re a great way to correct an imbalance of neurochemicals: True or False?❞
True! Contingently.
That is to say: they’re a great way to correct an imbalance of neurochemicals if and only if your problem is (at least partly) an imbalance of neurochemicals. If it’s not, then your brain can have all the neurotransmitters it needs, and you will still be depressed, because (for example) the other factors* influencing your depression have not changed.
*common examples include low self-esteem, poor physical health, socioeconomic adversity, and ostensibly bleak prospects for the future.
For those for whom the problem is/was partly a neurochemical imbalance and partly other factors, the greatest help the antidepressants give is getting the brain into sufficient working order to be able to tackle those other factors.
Want to know more about the different kinds?
Here’s a helpful side-by-side comparison of common antidepressants, what type they are, and other considerations:
Mind | Comparing Antidepressants
Want a drug-free approach?
You might like our previous main feature:
The Mental Health First-Aid That You’ll Hopefully Never Need
Take care!
Share This Post
-

Who Screens The Sunscreens?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We Screen The Sunscreens!

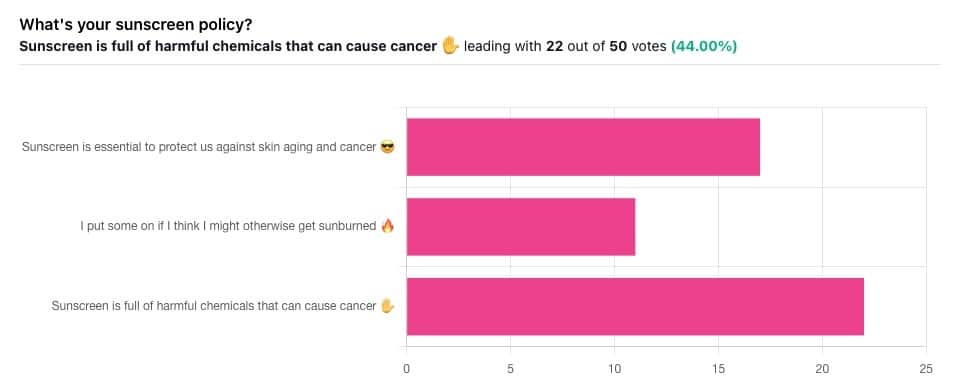
Yesterday, we asked you what your sunscreen policy was, and got a spread of answers. Apparently this one was quite polarizing!
One subscriber who voted for “Sunscreen is essential to protect us against skin aging and cancer” wrote:
❝My mom died of complications from melanoma, so we are vigilant about sun and sunscreen. We are a family of campers and hikers and gardeners—outdoors in all seasons—and we never burn❞
Our condolences with regard to your mom! Life is so precious, and when something like that happens, it tends to stick with us. We’re glad you and your family are taking care of yourselves.
Of the subscribers who voted for “I put some on if I think I might otherwise get sunburned”, about half wrote to express uncertainties:
- uncertainty about how safe it is, and
- uncertainty about how helpful it is
…so we’re going to tackle those questions in a moment. But what of those who voted for “Sunscreen is full of harmful chemicals that can cause cancer”?
Of those, only one wrote a message, which was to say one has to be very careful of what is in the formula.
Let’s take a look, then…
Sunscreen is full of harmful chemicals that can cause cancer: True or False?
False—according to current best science. Research is ongoing!
There are four main chemicals (found in most sunscreens) that people tend to worry about:
- Abobenzone
- Oxybenzone
- Octocrylene
- Ecamsule
Now, these two sound like four brands of rocket fuel, but then, dihydrogen monoxide (DHMO), which is also found in most sunscreens, sounds like a deadly toxin too. That’s water, by the way.
But what of these four chemicals? Well, as we say, research is ongoing, but we found a study that measured all four, to see how much got into the blood, and what adverse effects, if any, this caused.
We’ll skip to their conclusion:
❝In this preliminary study involving healthy volunteers, application of 4 commercially available sunscreens under maximal use conditions resulted in plasma concentrations that exceeded the threshold established by the FDA for potentially waiving some nonclinical toxicology studies for sunscreens. The systemic absorption of sunscreen ingredients supports the need for further studies to determine the clinical significance of these findings. These results do not indicate that individuals should refrain from the use of sunscreen.❞
Now, “exceeded the threshold established by the FDA for potentially waiving some nonclinical toxicology studies for sunscreens” sounds alarming, so why did they close with the words “These results do not indicate that individuals should refrain from the use of sunscreen”?
Let’s skip back up to a line from the results:
❝The most common adverse event was rash, which developed in 1 participant with each sunscreen.❞
This was most probably due to the oxybenzone, which can cause allergic skin reactions in some people.
Let us take a moment to remember the most common adverse event that occurs from not wearing sunscreen: sunburn!
You can read the full study here:
None of those ingredients have been found to be carcinogenic, even at the maximal blood plasma concentrations studied, from applications 4x/day to 75% of the body.
UVA rays, on the other hand, are absolutely very much known to cause cancer, and the effect is cumulative.
Sunscreen is essential to protect us against skin aging and cancer: True or False?
True, unequivocally, unless we live indoors and/or otherwise never go about under sunlight.
“But our ancestors—” lived under the same sun we do, and either used sunscreen or got advanced skin aging and cancer.
Sunscreen of times past ranged from mud to mineral lotions, but it’s pretty much always existed. Even non-human animals that have skin and don’t have fur or feathers, tend to take mud-baths in sunny parts of the world.
If you’d like to avoid oxybenzone and other chemicals, though, you might have your reasons. Maybe you’re allergic, or maybe you read that it’s a potential endocrine disruptor with estrogen-like and anti-androgenic properties that you don’t want.
There are other options, to include physical blockers containing zinc and titanium dioxide, which are generally recognized as safe and effective ingredients.
If you’re interested, you can even make your own sunscreen that blocks both UVA and UVB rays (UVA is what causes skin cancer; UVB is “milder” and is what causes sunburn):
Share This Post
-

Too Much Or Too Little Testosterone?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One Man’s Saw Palmetto Is Another Woman’s Serenoa Repens…
Today we’re going to look at saw palmetto. So, first:
What is it?
Saw palmetto is a type of palm native to the southeastern United States. Its scientific name is “Serenoa repens”, so if that name appears in studies we cite, it’s the same thing. By whichever name, it’s widely enjoyed as a herbal supplement.
Why do people take it?
Here’s where it gets interesting, because people take it for some completely opposite reasons…
Indeed, searching for it on the Internet will cause Google to suggest “…for men” and “…for women” as the top suggestions.
That’s because it works on testosterone, and testosterone can be a bit of a double-edged sword, so some people want to increase or decrease certain testosterone-related effects on their body.
And it works for both! Here be science:
- Testosterone (henceforth, “T”) is produced in the human body.
- Yes, all human bodies, to some extent.
- An enzyme called 5-alpha-reductase converts T in to DHT (dihydrogen testosterone)
- DHT is a much more potent androgen (masculinizing agent) than T alone, such that its effects are often unwanted, including:
- Enlarged prostate (if you have one)
- Hair loss (especially in men)
- New facial hair growth (usually unwanted by women)
- Women are more likely to get this due to PCOS and/or the menopause
To avoid those effects, you really want less of your T to be converted into DHT.
Saw palmetto is a 5α-reductase inhibitor, so if you take it, you’ll have less DHT, and you’ll consequently lose less hair, have fewer prostate problems, etc.
^The above study showed that saw palmetto extract performed comparably to finasteride. Finasteride is the world’s main go-to prescription drug for treating enlarged prostate and/or hair loss.
See also: Natural Hair Supplement: Friend or Foe? Saw Palmetto, a Systematic Review in Alopecia
Hair today… Growing tomorrow!
So, what was that about increasing T levels?
Men usually suffer declining T levels as they get older, with a marked drop around the age of 45. With lower T comes lower energy, lower mood, lower libido, erectile dysfunction, etc.
Guess what… It’s T that’s needed for those things, not DHT. So if you block the conversion of T to DHT, you’ll have higher blood serum T levels, higher energy, higher mood, higher libido, and all that.
(the above assumes you have testicles, without which, your T levels will certainly not increase)
Saw Palmetto Against Enlarged Prostate?
With higher DHT levels in mid-late life, prostate enlargement (benign prostatic hyperlasia) can become a problem for many men. The size of that problem ranges from urinary inconvenience (common, when the prostate presses against the bladder) to prostate cancer (less common, much more serious). Saw palmetto, like other 5α-reductase inhibitors such as finasteride, may be used to prevent or treat this.
Wondering how safe/reliable it is? We found a very high-quality fifteen-year longitudinal observational study of the use of saw palmetto, and it found:
❝The 15 years’ study results suggest that taking S. repens plant extract continuously at a daily dose of 320 mg is an effective and safe way to prevent the progression of benign prostatic hyperplasia.❞
Want a second opinion? We also found a 10-year study (by different researchers with different people taking it), which reached the same conclusion:
❝The results of study showed the absence of progression, both on subjective criteria (IPSS, and QoL scores), and objective criteria (prostate volume, the rate of urination, residual urine volume). Furthermore, patients had no undesirable effects directly related to the use of this drug.❞
- IPSS = International Prostate Symptom Score
- QoL = Quality of Life
❝But wait a minute; I, a man over the age of 45 with potentially declining T levels but a fabulous beard, remember that you said just a minute ago that saw palmetto is used by women to avoid having facial hair; I don’t want to lose mine!❞
You won’t. Once your facial hair follicles were fully developed and activated during puberty, they’ll carry on doing what they do for life. That’s no longer regulated by hormones once they’re up and running.
The use of saw palmetto can only be used to limit facial hair if caught early—so it’s more useful at the onset of menopause, for those who have (or will have) such, or else upon the arrival of PCOS symptoms or hirsuitism from some other cause.
Take The Test!
Do you have a prostate, and would like to know your IPSS score, and what that means for your prostate health?
(takes 1 minute, no need to pee or go probing for anything)
Bottom Line on Saw Palmetto
- It blocks the conversion of T into DHT
- It will increase blood serum T levels, thus boosting mood, energy, libido, etc in men (who typically have more T, but whose T levels decline with age)
- It will decrease DHT levels, thus limiting hair loss (especially in men) and later-life new facial hair growth (especially in women).
- It can be used to prevent or treat prostate enlargement
- Bonus: it’s a potent antioxidant and thus reduces general inflammation (in everyone)
Want To Try Saw Palmetto?
We don’t sell it (or anything else), but for your convenience…
Share This Post
- Testosterone (henceforth, “T”) is produced in the human body.
-

Soap vs Sanitizer – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing soap to sanitizer, we picked the soap.
Why?
Both are good at killing bacteria / inactivating viruses, but there are several things that set them apart:
- Soap doesn’t just kill them; it slides them off and away down the drain. That means that any it failed to kill are also off and down the drain, not still on your hands. This is assuming good handwashing technique, of course!
- Sanitizer gel kills them, but can take up to 4 minutes of contact to do so. Given that people find 20 seconds of handwashing laborious, 240 seconds of sanitizer gel use seems too much to hope for.
Both can be dehydrating for the hands; both can have ingredients added to try to mitigate that.
We recommend a good (separate) moisturizer in either case, but the point is, the dehydration factor doesn’t swing it far either way.
So, we’ll go with the one that gets rid of the germs the most quickly: the soap
10almonds tip: splash out on the extra-nice hand-soaps for your home—this will make you and others more likely to wash your hands more often! Sometimes, making something a more pleasant experience makes all the difference.
Want to know more?
Check out:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Powerful Constraints on Medical Care in Catholic Hospitals Across America
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Nurse midwife Beverly Maldonado recalls a pregnant woman arriving at Ascension Saint Agnes Hospital in Maryland after her water broke. It was weeks before the baby would have any chance of survival, and the patient’s wishes were clear, she recalled: “Why am I staying pregnant then? What’s the point?” the patient pleaded.
But the doctors couldn’t intervene, she said. The fetus still had a heartbeat and it was a Catholic hospital, subject to the “Ethical and Religious Directives for Catholic Health Care Services” that prohibit or limit procedures like abortion that the church deems “immoral” or “intrinsically evil,” according to its interpretation of the Bible.
“I remember asking the doctors. And they were like, ‘Well, the baby still has a heartbeat. We can’t do anything,’” said Maldonado, now working as a nurse midwife in California, who asked them: “What do you mean we can’t do anything? This baby’s not going to survive.”
The woman was hospitalized for days before going into labor, Maldonado said, and the baby died.
Ascension declined to comment for this article.
The Catholic Church’s directives are often at odds with accepted medical standards, especially in areas of reproductive health, according to physicians and other medical practitioners.
The American College of Obstetricians and Gynecologists’ clinical guidelines for managing pre-labor rupture of membranes, in which a patient’s water breaks before labor begins, state that women should be offered options, including ending the pregnancy.
Maldonado felt her patient made her wishes clear.
“Under the ideal medical practice, that patient should be helped to obtain an appropriate method of terminating the pregnancy,” said Christian Pettker, a professor of obstetrics, gynecology, and reproductive sciences at the Yale School of Medicine, who helped author the guidelines.
He said, “It would be perfectly medically appropriate to do a termination of pregnancy before the cessation of cardiac activity, to avoid the health risks to the pregnant person.”
“Patients are being turned away from necessary care,” said Jennifer Chin, an OB-GYN at UW Medicine in Seattle, because of the “emphasis on these ethical and religious directives.”
They can be a powerful constraint on the care that patients receive at Catholic hospitals, whether emergency treatment when a woman’s health is at risk, or access to birth control and abortions.
More and more women are running into barriers to obtaining care as Catholic health systems have aggressively acquired secular hospitals in much of the country. Four of the 10 largest U.S. hospital chains by number of beds are Catholic, according to federal data from the Agency for Healthcare Research and Quality. There are just over 600 Catholic general hospitals nationally and roughly 100 more managed by Catholic chains that place some religious limits on care, a KFF Health News investigation reveals.
Maldonado’s experience in Maryland came just months before the Supreme Court’s ruling in 2022 to overturn Roe v. Wade, a decision that compounded the impact of Catholic health care restrictions. In its wake, roughly a third of states have banned or severely limited access to abortion, creating a one-two punch for women seeking to prevent pregnancy or to end one. Ironically, some states where Catholic hospitals dominate — such as Washington, Oregon, and Colorado — are now considered medical havens for women in nearby states that have banned abortion.
KFF Health News analyzed state-level birth data to discover that more than half a million babies are born each year in the U.S. in Catholic-run hospitals, including those owned by CommonSpirit Health, Ascension, Trinity Health, and Providence St. Joseph Health. That’s 16% of all hospital births each year, with rates in 10 states exceeding 30%. In Washington, half of all babies are born at such hospitals, the highest share in the country.
“We had many instances where people would have to get in their car to drive to us while they were bleeding, or patients who had had their water bags broken for up to five days or even up to a week,” said Chin, who has treated patients turned away by Catholic hospitals.
Physicians who turned away patients like that “were going against evidence-based care and going against what they had been taught in medical school and residency,” she said, “but felt that they had to provide a certain type of care — or lack of care — just because of the strength of the ethical and religious directives.”
Following religious mandates can be dangerous, Chin and other clinicians said.
When a patient has chosen to end a pregnancy after the amniotic sac — or water — has broken, Pettker said, “any delay that might be added to a procedure that is inevitably going to happen places that person at risk of serious, life-threatening complications,” including sepsis and organ infection.
Reporters analyzed American Hospital Association data as of August and used Catholic Health Association directories, news reports, government documents, and hospital websites and other materials to determine which hospitals are Catholic or part of Catholic systems, and gathered birth data from state health departments and hospital associations. They interviewed patients, medical providers, academic experts, advocacy organizations, and attorneys, and reviewed hundreds of pages of court and government records and guidance from Catholic health institutions and authorities to understand how the directives affect patient care.
Nationally, nearly 800,000 people have only Catholic or Catholic-affiliated birth hospitals within an hour’s drive, according to KFF Health News’ analysis. For example, that’s true of 1 in 10 North Dakotans. In South Dakota, it’s 1 in 20. When care is more than an hour away, academic researchers often define the area as a hospital desert. Pregnant women who must drive farther to a delivery facility are at higher risk of harm to themselves or their fetus, research shows.
Many Americans don’t have a choice — non-Catholic hospitals are too far to reach in an emergency or aren’t in their insurance networks. Ambulances may take patients to a Catholic facility without giving them a say. Women often don’t know that hospitals are affiliated with the Catholic Church or that they restrict reproductive care, academic research suggests.
And, in most of the country, state laws shield at least some hospitals from lawsuits for not performing procedures they object to on religious grounds, leaving little recourse for patients who were harmed because care was withheld. Thirty-five states prevent patients from suing hospitals for not providing abortions, including 25 states where abortion remains broadly legal. About half of those laws don’t include exceptions for emergencies, ectopic pregnancies, or miscarriages. Sixteen states prohibit lawsuits against hospitals for refusing to perform sterilization procedures.
“It’s hard for the ordinary citizen to understand, ‘Well, what difference does it make if my hospital is bought by this other big health system, as long as it stays open? That’s all I care about,’” said Erin Fuse Brown, who is the director of the Center for Law, Health & Society at Georgia State University and an expert in health care consolidation. Catholic directives also ban medical aid in dying for terminally ill patients.
People “may not realize that they’re losing access to important services, like reproductive health [and] end-of-life care,” she said.
‘Our Faith-Based Health Care Ministry’
After the Supreme Court ended the constitutional right to abortion in June 2022, Michigan resident Kalaina Sullivan wanted surgery to permanently prevent pregnancy.
Michigan voters in November that year enshrined the right to abortion under the state constitution, but the state’s concentration of Catholic hospitals means people like Sullivan sometimes still struggle to obtain reproductive health care.
Because her doctor worked for the Catholic chain Trinity Health, the nation’s fourth-largest hospital system, she had the surgery with a different doctor at North Ottawa Community Health System, an independent hospital near the shores of Lake Michigan.
Less than two months later, that, too, became a Catholic hospital, newly acquired by Trinity.
To mark the transition, Cory Mitchell, who at the time was the mission leader of Trinity Health Muskegon, stood before his new colleagues and offered a blessing.
“The work of your hands is what makes our faith-based health care ministry possible,” he said, according to a video of the ceremony Trinity Health provided to KFF Health News. “May these hands continue to bring compassion, compassion and healing, to all those they touch.”
Trinity Health declined to answer detailed questions about its merger with North Ottawa Community Health System and the ethical and religious directives. “Our commitment to high-quality, compassionate care means informing our patients of all appropriate care options, and trusting and supporting our physicians to make difficult and medically necessary decisions in the best interest of their patients’ health and safety,” spokesperson Jennifer Amundson said in an emailed statement. “High-quality, safe care is critical for the women in our communities and in cases where a non-critical service is not available at our facility, the physician will transfer care as appropriate.”
Leaders in Catholic-based health systems have hammered home the importance of the church’s directives, which are issued by the U.S. Conference of Catholic Bishops, all men, and were first drafted in 1948. The essential view on abortion is as it was in 1948. The last revision, in 2018, added several directives addressing Catholic health institution acquisitions or mergers with non-Catholic ones, including that “whatever comes under control of the Catholic institution — whether by acquisition, governance, or management — must be operated in full accord with the moral teaching of the Catholic Church.”
“While many of the faithful in the local church may not be aware of these requirements for Catholic health care, the local bishop certainly is,” wrote Sister Doris Gottemoeller, a former board member of the Bon Secours Mercy Health system, in a 2023 Catholic Health Association journal article. “In fact, the bishop should be briefed on a regular basis about the hospital’s activities and strategies.”
Now, for care at a non-Catholic hospital, Sullivan would need to travel nearly 30 miles.
“I don’t see why there’s any reason for me to have to follow the rules of their religion and have that be a part of what’s going on with my body,” she said.
Risks Come With Religion
Nathaniel Hibner, senior director of ethics at the Catholic Health Association, said the ethical and religious directives allow clinicians to provide medically necessary treatments in emergencies. In a pregnancy crisis when a person’s life is at risk, “I do not believe that the ERDs should restrict the physician in acting in the way that they see medically indicated.”
“Catholic health care is committed to the health of all women and mothers who enter into our facilities,” Hibner said.
The directives permit care to cure “a proportionately serious pathological condition of a pregnant woman” even if it would “result in the death of the unborn child.” Hibner demurred when asked who defines what that means and when such care is provided, saying, “for the most part, the physician and the patients are the ones that are having a conversation and dialogue with what is supposed to be medically appropriate.”
It is common for practitioners at any hospital to consult an ethics board about difficult cases — such as whether a teenager with cancer can decline treatment. At Catholic hospitals, providers must ask a board for permission to perform procedures restricted by the religious directives, clinicians and researchers say. For example, could an abortion be performed if a pregnancy threatened the mother’s life?
How and when an ethics consultation occurs depends on the hospital, Hibner said. “That ethics consultation can be initiated by anyone involved in the direct care of that situation — the patient, the surrogate of that patient, the physician, the nurse, the social worker all have the ability to request a consultation,” he said. When asked whether a consultation with an ethics board can occur without a request, he said “sometimes it could.”
How strictly directives are followed can depend on the hospital and the views of the local bishop.
“If the hospital has made a difficult decision about a critical pregnancy or an end-of-life care situation, the bishop should be the first to know about it,” Gottemoeller wrote.
In an interview, Gottemoeller said that even when pregnancy termination decisions are made on sound ethical grounds, not informing the bishop puts him in a bad position and hurts the church. “If there’s a possibility of it being misunderstood, or misinterpreted, or criticized,” Gottemoeller said, the bishop should understand what happened and why “before the newspapers call him and ask him for an opinion.”
“And if he has to say, ‘Well, I think you made a mistake,’ well, all right,” she said. “But don’t let him be blindsided. I mean, we’re one church and the bishop has pastoral concern over everything in his diocese.”
Katherine Parker Bryden, a nurse midwife in Iowa who works for MercyOne, said she regularly tells pregnant patients that the hospital cannot perform tubal sterilization surgery, to prevent future pregnancies, or refer patients to other hospitals that do. MercyOne is one of the largest health systems in Iowa. Nearly half of general hospitals in the state are Catholic or Catholic-affiliated — the highest share among all states.
The National Catholic Bioethics Center, an ethics authority for Catholic health institutions, has said that referrals for care that go against church teaching would be “immoral.”
“As providers, you’re put in this kind of moral dilemma,” Parker Bryden said. “Am I serving my patients or am I serving the archbishop and the pope?”
In response to questions, MercyOne spokesperson Eve Lederhouse said in an email that its providers “offer care and services that are consistent with the guidelines of a Catholic health system.”
Maria Rodriguez, an OB-GYN professor at Oregon Health & Science University, said that as a resident in the early 2000s at a Catholic hospital she was able to secure permission — what she calls a “pope note” — to sterilize some patients with conditions such as gestational diabetes.
Annie Iriye, a retired OB-GYN in Washington state, said that more than a decade ago she sought permission to administer medication to hasten labor for a patient experiencing a second-trimester miscarriage at a Catholic hospital. She said she was told no because the fetus had a heartbeat. The patient took 10 hours to deliver — time that would have been cut by half, Iriye said, had she been able to follow her own medical training and expertise. During that time, she said, the patient developed an infection.
Iriye and Chin were part of an effort by reproductive rights groups and medical organizations that pushed for a state law to protect physicians if they act against Catholic hospital restrictions. The bill, which Washington enacted in 2021, was opposed by the Washington State Hospital Association, whose membership includes multiple large Catholic health systems.
State lawmakers in Oregon in 2021 enacted legislation that beefed up powers to reject health care mergers if they would reduce access to the types of care constrained by Catholic directives. The hospital lobby has sued to block the statute. Washington state lawmakers introduced similar legislation last year, which the hospital association opposes.
Hibner said Catholic hospitals are committed to instituting systemic changes that improve maternal and child health, including access to primary, prenatal, and postpartum care. “Those are the things that I think rural communities really need support and advocacy for,” he said.
Maldonado, the nurse midwife, still thinks of her patient who was forced to stay pregnant with a baby who could not survive. “To feel like she was going to have to fight to have an abortion of a baby that she wanted?” Maldonado said. “It was just horrible.”
KFF Health News data editor Holly K. Hacker contributed to this report.
Click to open the methodology Methodology
By Hannah Recht
KFF Health News identified areas of the country where patients have only Catholic hospital options nearby. The “Ethical and Religious Directives for Catholic Health Care Services” — which are issued by the U.S. Conference of Catholic Bishops, all men — dictate how patients receive reproductive care at Catholic health facilities. In our analysis, we focused on hospitals where babies are born.
We constructed a national database of hospital locations, identified which ones are Catholic or Catholic-affiliated, found how many babies are born at each, and calculated how many people live near those hospitals.
Hospital Universe
We identified hospitals in the 50 states and the District of Columbia using the American Hospital Association database from August 2023. We removed hospitals that had closed or were listed more than once, added hospitals that were not included, and corrected inaccurate or out-of-date information about ownership, primary service type, and location. We excluded federal hospitals, such as military and Indian Health Service facilities, because they are not open to everyone.
Catholic Affiliation
To identify Catholic hospitals, we used the Catholic Health Association’s member directory. We also counted as Catholic a handful of hospitals that are not part of this voluntary membership group but explicitly follow the Ethical and Religious Directives, according to their mission statements, websites, or promotional materials.
We also tracked Catholic-affiliated hospitals: those that are owned or managed by a Catholic health system, such as CommonSpirit Health or Trinity Health, and are influenced by the religious directives but do not necessarily adhere to them in full. To identify Catholic-affiliated hospitals, we consulted health system and hospital websites, government documents, and news reports.
We combined both Catholic and Catholic-affiliated hospitals for analysis, in line with previous research about the influence of Catholic directives on health care.
Births
To determine the share of births that occur at Catholic or Catholic-affiliated hospitals, we gathered the latest annual number of births by hospital from state health departments. Where recent data was not publicly available, we submitted records requests for the most recent complete year available.
The resulting data covered births in 2022 for nine states and D.C., births in 2021 for 23 states, births in 2020 for nine states, and births in 2019 for one state. We used data from the 2021 American Hospital Association survey, the latest available at the time of analysis, for the eight remaining states that did not provide birth data in response to our requests. A small number of hospitals have recently opened or closed labor and delivery units. The vast majority of the rest record about the same number of births each year. This means that the results would not be substantially different if data from 2023 were available.
We used this data to calculate the number of babies born in Catholic and Catholic-affiliated hospitals, as well as non-Catholic hospitals by state and nationally.
We used hospitals’ Catholic status as of August 2023 in this analysis. In 10 cases where the hospital had already closed, we used Catholic status at the time of the closure.
Because our analysis focuses on hospital care, we excluded births that occurred in non-hospital settings, such as homes and stand-alone birth centers, as well as federal hospitals.
Several states suppressed data from hospitals with fewer than 10 births due to privacy restrictions. Because those numbers were so low, this suppression had a negligible effect on state-level totals.
Drive-Time Analysis
We obtained hospitals’ geographic coordinates based on addresses in the AHA dataset using HERE’s geocoder. For addresses that could not be automatically geocoded with a high degree of certainty, we verified coordinates manually using hospital websites and Google Maps.
We calculated the areas within 30, 60, and 90 minutes of travel time from each birth hospital that was open in August 2023 using tools from HERE. We included only hospitals that had 10 or more births as a proxy for hospitals that have labor and delivery units, or where births regularly occur.
The analysis focused on the areas with hospitals within an hour’s drive. Researchers often define hospital deserts as places where one would have to drive an hour or more for hospital care. (For example: [1] “Disparities in Access to Trauma Care in the United States: A Population-Based Analysis,” [2] “Injury-Based Geographic Access to Trauma Centers,” [3] “Trends in the Geospatial Distribution of Inpatient Adult Surgical Services Across the United States,” [4] “Access to Trauma Centers in the United States.”)
We combined the drive-time areas to see which areas of the United States have only Catholic or Catholic-affiliated birth hospitals nearby, both Catholic and non-Catholic, non-Catholic only, or none. We then joined these areas to the 2021 census block group shapefile from IPUMS NHGIS and removed water bodies using the U.S. Geological Survey’s National Hydrography Dataset to calculate the percentage of each census block group that falls within each hospital access category. We calculated the number of people in each area using the 2021 “American Community Survey” block group population totals. For example, if half of a block group’s land area had access to only Catholic or Catholic-affiliated hospitals, then half of the population was counted in that category.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Fitness Walking and Bodyweight Exercises – by Frank S. Ring
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A lot of exercise manuals assume that the reader has a “basic” body (nothing Olympian, but nothing damaged either). As we get older, increasingly few of us fall into the “but nothing damaged either” category!
Here’s where Ring brings to bear his decades of experience as a coach and educator, and also his personal recovery from a serious back injury.
The book covers direct, actionable exercise advice (with all manner of detail), and also offers mental health tips he’s learned along the way.
Ring, like us, is a big fan of keeping things simple, so he focusses on “the core four” of bodyweight exercises:
- Pushups
- Squats
- Lunges
- Planks
These four exercises get a whole chapter devoted to them, though! Because there are ways to make each exercise easier or harder, or have different benefits. For example, adjustments include:
- Body angle
- Points of contact
- Speed
- Pausing
- Range of motion
This, in effect, makes a few square meters of floor (and perhaps a chair or bench) your fully-equipped gym.
As for walking? Ring enjoys and extols the health benefits, and/but also uses his walks a lot for assorted mental exercises, and recommends we try them too.
A fine book for anyone who wants to gain and/or maintain good health, but doesn’t pressingly want to join a gym or start pumping iron!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: